Article Text

Abstract
Objective Distinction on clinical grounds between acute lymphoblastic leukaemia presenting with arthropathy (ALLarthropathy) and juvenile idiopathic arthritis (JIA) is difficult, as the clinical and paraclinical signs of leukaemia may be vague. The primary aim was to examine the use of lectin complement pathway proteins as markers to differentiate ALLarthropathy from JIA. The secondary aims were to compare the protein levels at baseline and follow-up in a paired number of children with ALL and to examine the correlation with haematology counts, erythrocyte sedimentation reaction (ESR), C-reactive protein (CRP), blasts, relapse and death.
Study design In this observational study, we measured M-ficolin, CL-K1 and MASP-3 in serum from children with ALL (n=151) and JIA (n=238) by time-resolved immunofluorometric assays. Logistic regression was used for predictions of ALL risk, considering the markers as the respective exposures. We performed internal validation using repeated ‘10-fold cross-validation’ with 100 repetitions computing the area under the curve (AUC) as well as positive and negative predictive values in order to evaluate the predictive performance.
Results The level of M-ficolin was higher in JIA than ALLtotal and the ALLarthropathy subgroup. The M-ficolin level normalised after remission of ALL. M-ficolin could differentiate ALL from JIA with an AUC of 94% and positive predictive value (PPV) of 95%, exceeding CRP and haemoglobin. In a dichotomised predictive model with optimal cut-offs for M-ficolin, platelets and haemoglobin, AUC was 99% and PPV 98% in detecting ALL from JIA.
Conclusion M-ficolin is a valuable marker to differentiate the child with ALL from JIA.
- rheumatology
- statistics
- cell biology
- pain
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The following are freely available as supplementary appendices: (1) Clinical characteristics of patients in a paired ALL cohort (n = 73) at baseline, 29 days and 6 months of follow-up. (2) Correlation between M-ficolin, CL-K1, MASP-3 with age and laboratory values for patients with acute lymphoblastic leukemia at baseline (n = 151), 29 days (n = 88) and 6 months (n = 92) of follow-up. (3)Scatter plot illustrating the association between neutrophils and M-ficolin for the children with acute lymphoblastic leukemia in a paired cohort (n = 73) at baseline, 29 days and 6 months of follow-up (4) Correlation between M-ficolin, CL-K1, MASP-3 and age, laboratory values and joint activity for 238 children with JIA at baseline. (5) Supplementary material S5. Associations between lectin pathway proteins at baseline and blasts in peripheral blood, minimal residual disease day 29, relapse and death.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Acute lymphoblastic leukaemia (ALL) presents with arthropathy in up to 20% of cases.
These patients have only vague signs of leukaemia and up to three-quarters of them are misdiagnosed as juvenile idiopathic arthritis (JIA).
In JIA, M-ficolin has been suggested as a marker of disease activity with the highest serum levels in the systemic subtype.
What this study adds?
Serum levels of M-ficolin were significantly higher in patients with JIA than ALL as well as in ALL patients with arthropathy.
In a univariable predictive model, M-ficolin could differentiate ALL from JIA with an area under the curve (AUC) of 93% and PPV of 94%, exceeding CRP and haemoglobin.
In a dichotomised multivariable predictive model with optimal cut-offs for M-ficolin, platelets and haemoglobin, the AUC was 99.4% in differentiating ALL from JIA.
Introduction
Children with acute lymphoblastic leukaemia (ALL) present with arthralgia in 16%–20% and arthritis in 6%–9% of cases, and other signs of leukaemia may be weak or missing.1–4 In previous studies, we found that even a high number of joints involved does not exclude ALL.5 In the literature, 26%–76% of children with ALLarthropathy are misdiagnosed as juvenile idiopathic arthritis (JIA), and up to 70% receive treatment with intra-articular or even systemic corticosteroids, which may conceal the signs of leukaemia.2 4 6–8
The lectin complement pathway is, along with the classical and alternative pathway, an essential part of the complement system.9–12 The lectin pathway-mediated activation of the complement system proceeds through recognition of pathogens or other unnormal structures by the soluble pattern recognition molecules: mannan-binding lectin (MBL), ficolins (M, L and H-ficolin), and collagen-containing C-type lectins (collectins), kidney collectin CL-K1 and liver collectin CL-L1.13–15 These circulating lectins are found in complex with serine proteases named MBL-associated serine proteases (MASPs), comprising MASP-1, MASP-2 and MASP-3 as well as two non-enzymatic proteins called MAp19 and MAp44.14 Studies on the lectin pathway proteins in JIA,10 16 17 and especially in ALL, are scarce.18 M-ficolin has been investigated in one study of children with cancer, including a subgroup of 41 children with ALL, having lower M-ficolin compared with a healthy, age-matched control group.18 In JIA, M-ficolin has been proven as a marker of disease activity with the highest level in the systemic subtype.10 17 CL-K1 and MASP-3 have been suggested as indicators of inflammation and disease activity in JIA.10 17 Levels of CL-K1 and MASP-3 have not previously been investigated in children with ALL. As the only study of the lectin pathway in children with ALL indicate low M-ficolin levels and M-ficolin has proven to be a marker of disease activity in JIA, we hypothesised that it would be possible to differentiate ALL from JIA by M-ficolin.
The primary aim of our study was to evaluate the predictive value of M-ficolin, CL-K1 and MASP-3 in order to differentiate the child with ALLarthropathy from JIA. The secondary aims were to compare the level of the lectin pathway proteins at baseline and follow-up in ALL and to examine the correlation with haematology counts, ESR, CRP, blasts, relapse and death.
Methods
We included consecutive cases of newly diagnosed patients with JIA from defined geographical areas of Denmark, Finland, Norway and Sweden, as previously described in detail.19 20 They had disease onset from 1 January 1997 to 30 June 2000. The Finnish part of the original cohort had no access to storage of blood samples at baseline, and accordingly, this centre was not included in the present study (figure 1). JIA was diagnosed according to the International League of Associations for Rheumatology (ILAR).21 We collected the following data of children with JIA: age, sex, disease category, number of active and cumulative joints with arthritis, haemoglobin, platelets, erythrocyte sedimentation reaction (ESR), C-reactive protein (CRP),and Juvenile Arthritis Disease Activity Score for 71 joints (JADAS71 score). The baseline samples were collected between inclusion and the baseline visit performed as close to 6 months after disease onset.

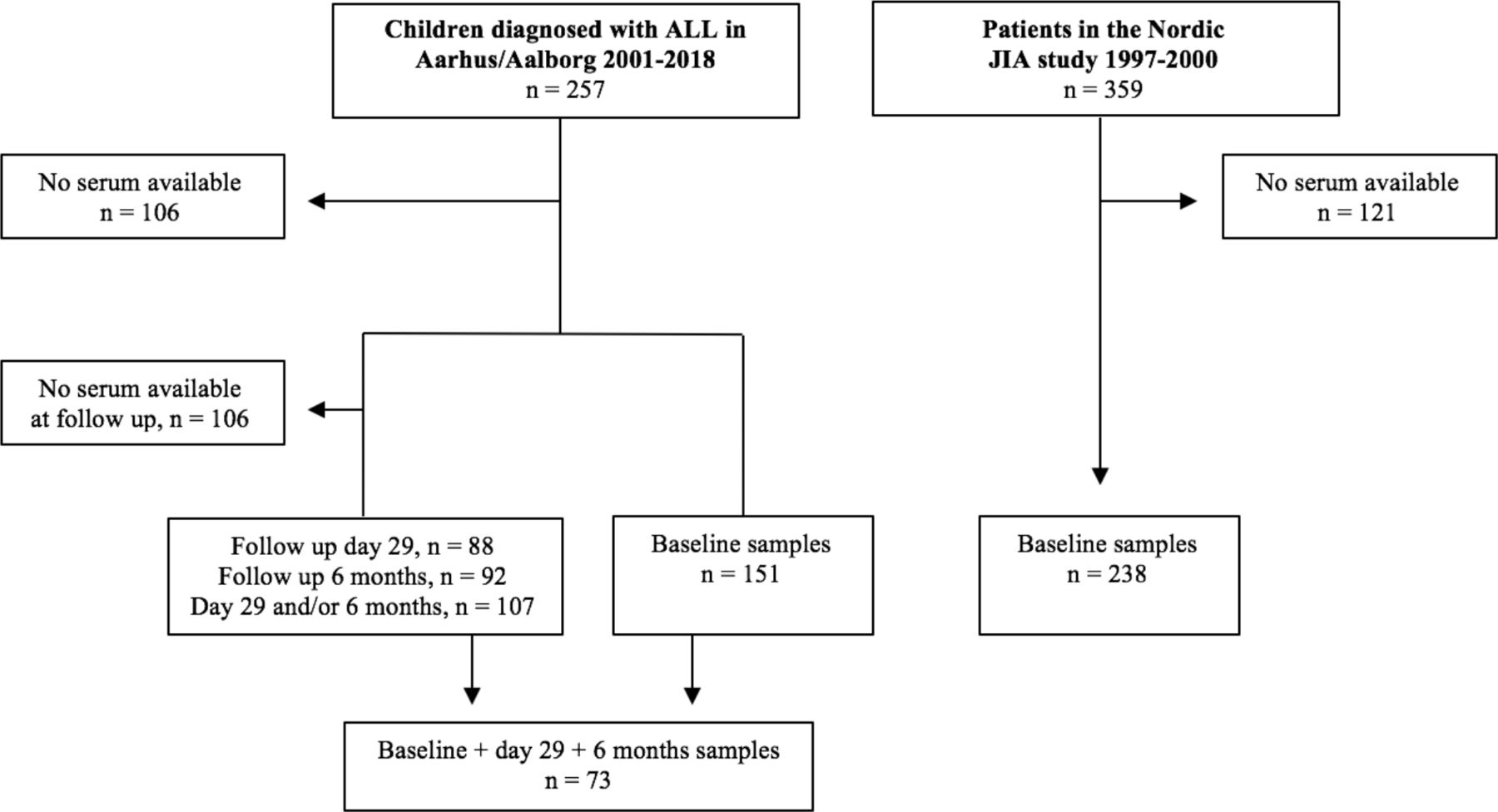
Flow chart of the study population. ALL, acute lymphoblastic leukaemia; JIA, juvenile idiopathic arthritis.
We further included consecutive, newly diagnosed children with ALL from a non-selected, population-based Danish ALL cohort, with inclusion from 1 January 2001 to 31 December 2018 from Aalborg and Aarhus University Hospitals, Denmark (figure 1). We collected following data at baseline, at day 29 and after 6 months of the children with ALL: age, sex, risk group, number of active and cumulative joints with arthritis, haemoglobin, platelets, leukocytes, differential count, ESR, CRP, lactate dehydrogenase (LDH), uric acid, blasts in peripheral blood, minimal residual disease at day 29, relapse and death. Baseline data were collected as close to diagnosis as possible (±1 week) and the follow-up samples from ALL were during remission.
Time-resolved immunofluorometric assays
Serum was collected and stored at – 80°C. Serum concentrations of M-ficolin, CL-K1 and MASP-3 were determined using validated in-house time-resolved immunofluorometric assays (TRIFMAs).22–24 Microtitre wells were coated with specific capture antibody, followed by the addition of diluted samples and subsequent specific detection of bound protein using biotinylated detection antibody. This was followed by binding of europium-labelled streptavidin and reading of signal in the wells by time-resolved fluorometry (Victor X5VR, PerkinElmer, Waltham, Massachusetts, USA). Sample dilution and loading on microtitre plates were automated using a pipetting robot (JANUS, PerkinElmer, Hamburg, Germany). All serum samples were analysed in duplicate, and the analysis was repeated if the coefficient of variation (%CV) between the wells was >15%. Three internal controls were used on all microtitre plates to ensure the reproducibility of the assay; the %CVs of these were below 15%. All analyses were performed blinded to patient data.
Statistical analysis
Data were non-normally distributed (evaluated by QQ-plots and histograms), and therefore, the results are presented as medians with IQR for continuous variables, and comparisons were made by Mann-Whitney U and Kruskal-Wallis test. Fisher’s exact test was used for comparison of dichotomous variables. For comparison of follow-up in paired patient data, we used Wilcoxon signed-rank test for continuous variables and McNemar’s test for dichotomous variables. All comparisons within follow-up times were only made for children with full follow-up time. The median of follow-up for children with ALL was calculated as the reverse Kaplan-Meier estimate. Correlation of the biomarkers with laboratory values at baseline and follow-up was analysed using Spearman’s rank-order correlation.
In order to establish a prediction model for ALL detection, we initially identified potential predictor variables being M-ficolin, CL-K1, MASP-3, haemoglobin, platelets and CRP. Logistic regression was used for the predictions, considering ALL status as the outcome. As the predictors did not fulfil the linearity assumption in the logistic regression model, they were fitted using restricted cubic splines with three knots. We performed internal validation using repeated ‘10-fold cross-validation’ with 100 repetitions computing the optimism corrected area under the ROC curve (AUC) in order to evaluate the predictive performance of the final models. Furthermore, sensitivity, specificity, positive and negative predictive values were computed using a threshold of 0.5 for the predicted probabilities of ALL. In the cross-validation process, the same random seed was used for each model for comparison. Percentiles (2.5% and 97.5%) of the cross-validated estimates from all repetitions were computed as confidence limits. Univariable models were fitted for the predictors M-ficolin, CL-K1 and MASP-3, to find the one with the best performance. Of the three univariable biomarker models, M-ficolin had the highest cross-validated AUC value. Three multivariable models were then fitted, the first one included M-ficolin, platelets and haemoglobin; the second included M-ficolin and CRP; and the third included haemoglobin, platelets and CRP. For the multivariable model with the best performance in the cross-validation process, we identified optimal cut-off values of the included variables in univariable models on the full data set. This was done by ROC analyses with the goal of a sensitivity of minimum 95% due to the severity of ALL.
All statistical tests were performed under a two-sided significance level of 0.05. We used STATA1 V.16.1 (StataCorp) and RV.3.6.325 for the statistical analysis.
Ethics
The investigation was approved by the Medical Ethics Committee1–10 and the Danish Data Protection Agency.1–16 For the data and samples of the JIA cohort, it was approved by the national research committees (1-10-72-280-13, 2012/2051, Dnr 2014/413-31, 174/13/03/03/2014), and all patients gave their written informed consent.
Results
Of the original Nordic JIA cohort of 359 children, serum samples from Norway, Sweden and Denmark were available for 238 patients at baseline (figure 1). The distribution of JIA categories at baseline was as follows: oligoarticular JIA: 121 (51%), RF-negative polyarticular JIA: 47 (20%), undifferentiated JIA: 32 (13%), enthesitis-related arthritis: 20 (8%), systemic JIA: 11 (5%), RF-positive polyarticular JIA: 5 (2%), juvenile psoriatic arthritis: 2 (1%). Previously, further details of the JIA cohort have been published.17 20
Of children diagnosed with ALL at Aalborg and Aarhus University Hospitals in Denmark, serum samples were available in 151 out of 257 at baseline and in 73 at both baseline, follow-up day 29 and 6 months (figure 1). The cohort included 128 (85%) with pre-B ALL and 23 (15%) with T-ALL. At baseline, arthropathy occurred in 26 (20%) of the children with pre-B ALL, including 7 (5%) diagnosed with arthritis (median two active joints (range 1–8)). One child with T-ALL presented with arthropathy.
Baseline laboratory values for patients with ALL and JIA are shown in table 1. The median level of M-ficolin was fourfold higher in children with JIA compared with the total ALL cohort as well as the ALLarthropathy subgroup (table 1, figure 2). M-ficolin levels were higher in patients with T-ALL: 1.42 µg/mL (IQR 0.86–2.77) compared with the patients with pre-B ALL: 0.55 µg/mL (IQR 0.31–1.00), p<0.001. M-ficolin levels gradually increased with the risk groups: standard risk (n=73): 0.51 µg/mL (IQR 0.31–1.00, p<0.001), intermediate risk (n=45): 0.54 µg/mL (IQR 0.28–0.93, p<0.001) and high risk (n=33): 0.68 µg/mL (IQR 0.31–1.12, p=0.004). The children with systemic JIA (n=11) had an even higher level of M-ficolin of 4.2 µg/mL (IQR 3.4–6.3) than the other JIA categories, p<0.05. The children with JIA, who received disease-modifying anti-rheumatic drugs (DMARD) (45/238) had a higher level of M-ficolin of 3.40 µg/mL (IQR 2.80–4.32) compared with the children without, 2.93 µg/mL (IQR 2.37–3.76), p=0.01, and a markedly higher level than the children with ALL, 0.65 (IQR 0.32–1.21), p<0.001. CL-K1 was moderately decreased and MASP-3 was moderately elevated in children with JIA as compared with the total ALL group and to the ALLarthropathy (table 1, figure 2). CL-K1 and MASP-3 did not differentiate between the subgroups in ALL or JIA. Patients with ALLarthropathy (n=27) had higher levels of haemoglobin and platelet count compared with ALL patients without arthropathy (n=124).

Box plots illustrating for the concentration of CL-K1, M-ficolin and MASP-3 in all (n=151), ALLarthropathy (n=27) and JIA (n=238) at baseline and in all in a paired cohort (n=73) at baseline, 29 days and 6 months of follow-up. ALLarthropathy, acute lymphoblastic leukaemia presenting with arthropathy; JIA, juvenile idiopathic arthritis.
Baseline clinical characteristics and level of lectin pathway proteins of patients with respectively total ALL (n=151) vs JIA (n=238) and for ALLarthropathy (n=27) vs JIA (n=238)
M-ficolin and CL-K1 gradually increased with time to follow-up, whereas MASP-3 significantly decreased at day 29 and rose at 6 months of follow-up (figure 2, online supplemental data S1). In the children with ALL, M-ficolin levels were positively related to haemoglobin, platelets, leucocytes, neutrophils, monocytes, lymphocytes as well as LDH and negatively to CRP and ESR (online supplemental data S2). Data on neutrophils were only available in the children with ALL. There was medium and strong correlation between M-ficolin and neutrophil levels at baseline and follow-up and the associations are shown in scatterplots (online supplemental data S3). In the children with JIA, M-ficolin levels were positively related to platelets, CRP and ESR, and negatively related to haemoglobin and age (online supplemental data S4).
Supplemental material
For the children with ALL, median time of follow-up was 7.5 years (IQR 5.0–10.2); during this period, 15 (10%) died and 14 (9%) had relapsed. The baseline level of M-ficolin, CL-K1 and MASP-3 did not differ whether or not the children had blasts in peripheral blood, minimal residual disease at day 29, relapse or died (online supplemental data S5).
We evaluated the predictive performance of M-ficolin, CL-K1 and MASP-3 individually and in combination with haemoglobin, platelets and CRP to differentiate ALL from JIA. The study population included 324 individuals, 140 patients with ALL and 184 patients with JIA. Cross-validated AUC values on the individual performance of M-ficolin, CL-K1 and MASP-3 showed the highest value for M-ficolin, at 93.5 (95% CI 82.7 to 100.0). CL-K1 and MASP-3 had insufficient discrimination ability and were therefore not included in the predictive models. AUC values estimating the performance of M-ficolin increased in combination with CRP and in combination with platelets and haemoglobin (table 2). ROC curves on the full dataset are illustrated in figure 3, showing the performances of M-ficolin, haemoglobin, platelets and CRP individually with optimal cut-offs and in combination (figure 3). A slight decrease in the cross-validated AUC was seen in the model when including M-ficolin, platelets and haemoglobin as dichotomised variables according to the optimal cut-offs, instead of the continuous versions (table 2).

{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristics curves with optimal cut-offs for non-optimism corrected models. CRP, C-reactive protein.
Predictive value of M-ficolin, CRP, haemoglobin and platelets as univariable and multivariable models to detect acute lymphoblastic leukaemia from juvenile idiopathic arthritis
Discussion
The level of M-ficolin was higher in children with JIA compared with the total ALL group and to the ALLarthropathy subgroup. In univariable as well as multivariable predictive models, we found M-ficolin to be a valuable marker to identify the child with ALLarthropathy from the child with JIA. Other components of the lectin complement pathway like CL-K1 and MASP-3 had insufficient discrimination ability.
The level of M-ficolin in the present ALL cohort (0.65 µg/mL) was consistent with data from another study with 41 children with ALL: 0.58 µg/mL.18 The level of M-ficolin in 94 children with different cancer diagnoses was consistent with age-matched controls (1.6 µg/mL vs 1.7 μg/mL, p=0.92).18 26
After induction therapy (29 days) and later follow-up (6 months), M-ficolin levels in patients with ALL increased to levels comparable to healthy controls pointing towards the close correlation of low M-ficolin levels in ALL being related to the state of the disease. The level of M-ficolin in the present JIA cohort has been described previously17 and is consistent with the findings of Petri et al,10 who reported that M-ficolin levels were higher in patients with systemic JIA than in persistent oligoarticular JIA. The increased levels in the systemic JIA category reflects the increased inflammatory activity and elevated ESR, CRP, platelets, leukocytes and neutrophils, to which they correlated.10
Identifying the child with ALLarthropathy from JIA is challenging when no or few cell lines are involved and in the absence of blasts in peripheral blood.5 6 M-ficolin level was equally low whether or not the child had blasts in peripheral blood, and lowest with standard risk, strengthening the clinical value of M-ficolin.
A limitation of this study is the number of patients with unavailable serum samples with the risk of selection bias in both the ALL and JIA cohort. Though, we found no differences in age or categories for either ALL or JIA when comparing the included with the group excluded. Only seven children had arthritis in the group of children with ALL, which reduces the ability to compare the number of affected joints among the groups.
Baseline samples for the JIA group were collected at diagnosis, or at least within 6 months after disease onset, and 81% of the patients were treatment-naïve when the samples were taken. A concern could be the long-term stability of complement proteins over such a long storage period as the very long-term stability of the proteins is not fully elucidated and might have affected the results. Although the baseline samples are almost similar to the levels found by previous studies with shorter storage periods.10 27 Though, these issues may have influenced the protein levels and conceivably have impaired the predictive abilities of the lectin proteins.
To evaluate the inherent problem of overfitting in predictive models, we divided the covariables, giving three instead of two models and performed internal validation using ‘repeated 10-fold cross-validation’. External validation in future studies would ensure that the diagnostic performance is reproducible.
In conclusion, we found M-ficolin to be a valuable marker to identify the child with ALLarthropathy from the child with JIA in both univariable as well as multivariable predictive models. The M-ficolin level normalised after remission of ALL. M-ficolin may lead to earlier diagnosis of ALL in children with onset of arthritis misdiagnosed to have JIA. Our prediction model calls for a validation of M-ficolin as a biomarker repeating the study in another non-selected cohort.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The following are freely available as supplementary appendices: (1) Clinical characteristics of patients in a paired ALL cohort (n = 73) at baseline, 29 days and 6 months of follow-up. (2) Correlation between M-ficolin, CL-K1, MASP-3 with age and laboratory values for patients with acute lymphoblastic leukemia at baseline (n = 151), 29 days (n = 88) and 6 months (n = 92) of follow-up. (3)Scatter plot illustrating the association between neutrophils and M-ficolin for the children with acute lymphoblastic leukemia in a paired cohort (n = 73) at baseline, 29 days and 6 months of follow-up (4) Correlation between M-ficolin, CL-K1, MASP-3 and age, laboratory values and joint activity for 238 children with JIA at baseline. (5) Supplementary material S5. Associations between lectin pathway proteins at baseline and blasts in peripheral blood, minimal residual disease day 29, relapse and death.
Ethics statements
Patient consent for publication
Acknowledgments
The authors acknowledge Søren Lundbye-Christensen from the Unit of Clinical Biostatistics, Aalborg University Hospital for statistical assistance.
The authors acknowledge Karen Møller, Department of Paediatric and Adolescent Medicine, Aarhus University for handling the serum samples and Annette Gudmann Hansen for laboratory assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators The Nordic Study Group of Pediatric Rheumatology (NoSPeR) group.
Contributors All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to submission. TH, HH and NB contributed to the design and conception of the study. NB was responsible for acquisition of all data from the patients with ALL at baseline and additional characteristics at follow-up. BK was responsible for acquisition of blood samples at follow-up for the TRIFMA analysis in the children with ALL. MG, LB, AF, SN, EN, MR and TH were responsible for acquisition of all data and serum samples from the JIA patients. ST and CEM were responsible for testing samples for proteins of the lectin pathway. RGS and NB performed the statistical analyses and Figs. TH and HH contributed to the interpretation of data. All authors have revised and approved the final paper.
Funding This project received grants from: Arvid Nilsson’s (grant number 1780631), Danish Childhood Cancer Foundation (grant number 2017-1945) and Ølufgård Memorial Fund (grant number 25734).
Disclaimer No sponsors or funders (other than the named authors) played any role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.