Article Text

Abstract
Introduction Children requiring multiple blood transfusions are at high risk of transfusion-transmissible infections (TTIs). Lao People’s Democratic Republic is a low-resource setting where donor blood screening faces challenges. This study aimed to determine the burden of TTIs in children in Vientiane Capital.
Methods 300 children with transfusion history and 300 controls were recruited. In addition, 49 newly diagnosed transfusion recipients were followed for up to 12 months. Serum was tested for hepatitis B surface antigen and IgG antibodies against parvovirus B19, hepatitis B, C and E viruses.
Results The patients had a similar prevalence of anti-hepatitis B core antibodies (56; 18.7%) and hepatitis B surface antigen (8; 2.7%) as the controls (58; 19.3% and 9; 3.0%, respectively). However, there was a higher prevalence of an antibody profile suggestive of hepatitis B vaccination (anti-hepatitis B surface antibody positive/anti-hepatitis B core antibody negative) in the transfused group (140/299; 46.8%) than in controls (77/300; 25.7%, p<0.01). All other markers were similar in the patients and controls or higher in the controls: anti-hepatitis C virus (2.7% and 3.3%, p=0.6), anti-hepatitis E virus (7.5% and 12.7%, p=0.006) and anti-parvovirus B19 (2.4% and 8.5%, p=0.001). The longitudinal cohort did not show an increase in any marker over time.
Conclusion Our results suggest no significant role of TTIs in Lao children. The higher prevalence of the hepatitis B vaccination profile in transfusion recipients showed that recommendations to vaccinate before commencing transfusions is at least partially implemented, although there is room for improvement.
- communicable diseases
- epidemiology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The burden of hepatitis B virus (HBV) and other transfusion-transmissible infections (TTIs) has not yet been investigated in Lao children with thalassemia and other reasons for multiple blood transfusions, but is important to know because some infections are vaccine-preventable.
WHAT THIS STUDY ADDS
The study showed that in the investigated cohort of Lao children receiving transfusions, TTI did not play an important role.
The transfused children had a higher prevalence of the HBV vaccination profile than the controls, while the prevalence of markers of previous infection with different diseases was not significantly different or higher in the controls.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The study suggested that HBV vaccination prior to transfusion start is at least partially implemented, but the realisation of this recommendation by doctors in charge of transfusion recipients can and should still be improved.
Long-term follow-up studies are required to better estimate the risk of TTI and to define improvements to current donor blood screening procedures.
Introduction
In 2019, there were 117.4 million blood transfusions worldwide, with more than half given to children aged less than 5 years old in low-income countries.1
Hepatitis B virus (HBV), hepatitis C virus (HCV), syphilis and HIV are the main pathogens causing transfusion-transmissible infections (TTIs), and blood donors are routinely screened for these diseases. Other TTIs are not routinely screened, especially in resource-limited settings.2 3 For example, parvovirus B19 (primate erythroparvovirus 1) can cause aplastic crisis in patients with hemoglobinopathies,4–6 and hepatitis E virus (HEV) infection is usually asymptomatic but can lead to acute chronic liver failure or chronic infection in immunocompromised people.7
Lao People’s Democratic Republic (PDR), which is located in Southeast Asia and has a population of approximately 7 million people, exhibits a high morbidity and mortality due to HBV infection. Vaccination was introduced in 2001 and combined diphtheria, tetanus, pertussis, hepatitis B and Haemophilus influenzae vaccine is currently scheduled at 6, 10 and 14 weeks of age.8 Since 2003, birth-dose vaccination is recommended in addition.9 Maternal HBV screening (by HBsAg rapid test) is also recommended, but is unevenly implemented in the country.10 11 In a study from 2006, we found that 43.7% of voluntary Lao first-time blood donors had anti-HBc antibodies and 9.6% were HBsAg positive.12 In a follow-up study from 2013 to 2015, prevalence rates of 44.1% and of 9.2% were detected among first-time donors, while repeat donors had an anti-HBc prevalence of 37.0% and an HBsAg prevalence of 3.9%.13 Importantly, a high frequency (approximately 4%) of Lao blood donors had occult HBV infection (HBsAg negative, DNA positive). These infections would not be detected by routine blood screening, which is done by HBsAg rapid test or ELISA, and are therefore a potential threat for transfusion recipients. HBV transmission rates from positive donors to transfusion recipients have been reported to vary from 3% to 48%.12 The risk of HBV transmission depends on the type and amount of the blood product transfused, viral load in the donor and the presence of anti-HBs antibodies in the donor and recipient.14 15 Blood donations in Lao PDR are also screened for HCV, HIV and syphilis by rapid test and/or ELISA, but not for HEV or human parvovirus B19 (Dr Chanthala Souksakhone, personal communication). HEV is transmitted mainly via the faecal-oral (genotypes 1 to 4) and/or foodborne (genotypes 3 and 4) routes and the majority of cases are asymptomatic or show self-limiting disease. In our previous studies in Lao PDR, we found significant HEV exposure and people in close contact with swine or cattle had higher anti-HEV seroprevalence in comparison with the general population.16 17 In contrast, parvovirus B19, which is mostly transmitted through respiratory secretions and normally has a mild clinical presentation in children, does not appear to be widespread in Lao PDR, although there are limited data.18
Most multiple transfusions for children in Lao PDR are due to thalassemia major, a disorder of haemoglobin in red blood cells caused by different mutations.19 20 Thalassemia major causes severe anaemia from early childhood on and requires lifelong blood transfusions,21 22 mostly with packed red blood cells.23 Iron overload in transfused children is monitored by checking serum ferritin levels and if the value is above 1000 ng/mL, iron chelation therapy is started according to local guidelines.23 The number of patients with thalassemia in Lao PDR is high due to the prevalence of beta thalassemia haemoglobin (Hb E; 30.1% in pregnant women)24 and other countries reported increased TTI in such patients.2 Despite a number of studies on the epidemiology of thalassemia in Lao PDR,25 26 the burden of TTI has not been investigated in this context. Thus, the aim of this study was to determine the burden of HBV and other TTI in Lao children with thalassemia and other reasons for multiple blood transfusions.
Materials and methods
This study was conducted in the Children’s Hospital, Vientiane, Lao PDR between March 2017 and December 2019. The cross-sectional cohort included all children aged less than 18 years old who came for a repeat transfusion as well as an age-matched and sex-matched non-transfused control group recruited from the outpatient department (OPD) and the allergy and immunology department in the same hospital. The longitudinal cohort recruited 49 children with newly diagnosed illness and no history of transfusion and they were sampled at each subsequent visit.
The participant’s legal representatives were informed of the objectives and methods of the study, and written informed consent was obtained before enrolment. A questionnaire was administered including the medical history (diagnosis, number of blood transfusions, volume of blood given), age and sex.
Five millilitres of blood was taken for the study and allowed to clot. Serum was separated by centrifugation and kept at −80°C for long-term storage. For the cross-sectional cohort, only one blood sample was taken before transfusion, while for the longitudinal cohort, blood was taken before the first and before each subsequent transfusion within the study period.
After collection, the samples were tested with a rapid test for the hepatitis B surface antigen (HBsAg; ONE STEP HBsAg TEST, SD BIOLINE). The results of the rapid testing were communicated to the doctor in charge, who counselled all patients and their parents on the same day or at the next appointment.
Commercial ELISA kits were used to test for anti-HBs and anti-HBc antibodies (Diasorin). Anti-HBs positive (≥10 mIU/mL) and anti-HBc negative profile was interpreted as protection through vaccination, and anti-HBc positive results as exposure to HBV. Anti-HBc positive and anti-HBs negative sera were tested for HBsAg, a marker for acute and chronic HBV infection, also by ELISA (qualitative; Diasorin). Additionally, commercial ELISA kits were used to determine anti-HCV (qualitative; Diasorin), anti-HEV (qualitative; Diasorin) and anti-parvovirus B19 (quantitative; Serion) antibody prevalence. Due to limited serum volume, one sample from the cross-sectional cohort could not be tested for anti-HEV antibodies and another sample from the same cohort was not screened for anti-HBs, anti-HCV, anti-parvovirus B19 and anti-HEV antibodies. Borderline results from anti-parvovirus B19 and anti-HEV testing were classified as negative.
Data were analysed with STATA software V.13. Descriptive data included independent variables such as age, sex, diagnosis, number of blood transfusions and blood volume received during that visit. Bivariate analysis was used to test the association between serological profiles and independent variables. The χ2 test or Fisher’s exact test was used as appropriate.
Results
Longitudinal cohort
More than half of the newly diagnosed participants were female (32/49; 65.3%). The mean age was 7.2 years (age range 1–15 years). More than half of the children (32/49; 65.3%) were diagnosed with thalassemia during their hospital consultation. None of the 49 participants were positive for HBsAg by rapid test or for anti-parvovirus and only one patient each was positive for anti-HBc and anti-HCV. Four patients were anti-HEV seropositive. During the study period, only seven newly diagnosed children received transfusions; two had only a single transfusion, two had two transfusions and three had three transfusions. Before transfusion, one out of seven was anti-HEV positive and one out of seven was anti-HCV positive. None were positive for HBsAg, anti-HBc or anti-parvovirus B19 antibodies. No seroconversion was observed during the study period.
Cross-sectional cohort
A total of 300 children (50.7% female) were enrolled in the cross-sectional cohort as cases and 300 age-matched children served as controls (50.3% female). Among the 300 transfused children, 28.0% were ≤5 years, 41.7% were 6–10 years and 30.3% were more than 10 years old (mean age was 8.5). Nearly all children (n=298, 99.3%) had thalassemia and only 2 (0.7%) had undiagnosed anaemia at the time of recruitment. In the control group, the most common diagnoses were pharyngitis (35.7%) and acute diarrhoea (36.3%, table 1). The vast majority (63.3%) of transfused children had received more than 15 transfusions, usually with a volume of more than 250 mL of packed red blood cells per transfusion (75.3%, table 1).
Sociodemographic and medical data of the cross-sectional cohort
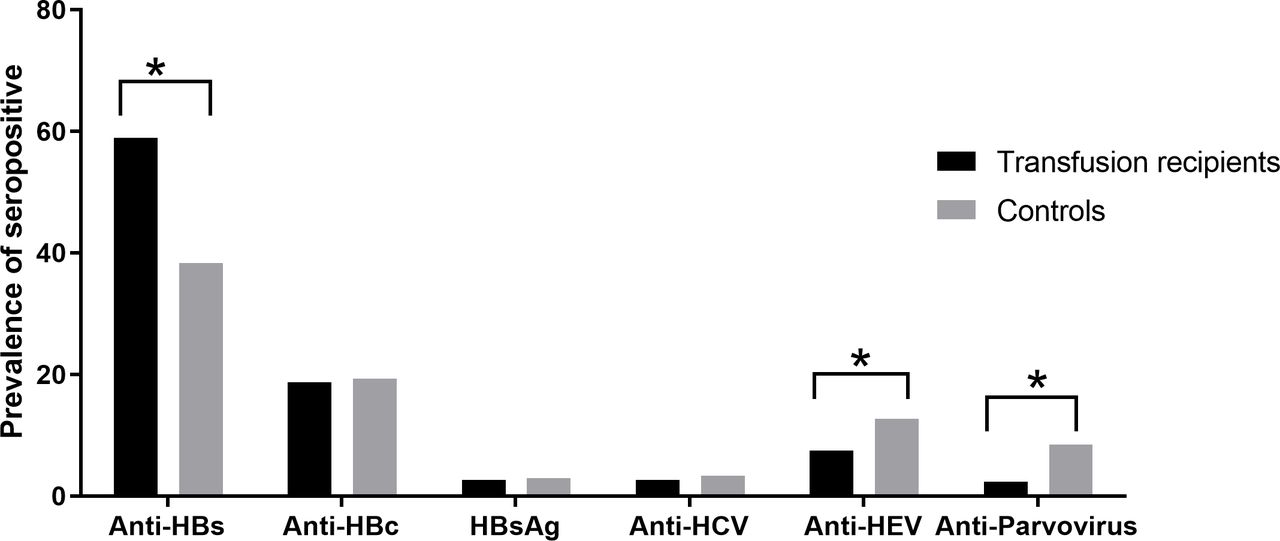
Anti-HBs antibody seroprevalence was significantly higher in the transfusion recipients (176/299; 58.9%) than the controls (115/300; 38.3%; p<0.001; figure 1, online supplemental table). The serological profile indicating vaccination (anti-HBs positive, anti-HBc negative) was also more common among transfused patients (140/299; 46.8%) compared with controls (77/300; 25.7%; p<0.01). Prior exposure to HBV, as indicated by anti-HBc antibodies, was not significantly different between the transfused patients (56/300; 18.7%) and controls (58/300; 19.3%; p=0.5). Similarly, HBsAg prevalence was not significantly different in transfusion recipients (8/300; 2.7%) compared with controls (9/300; 3.0%; p=0.8). Out of 17 HBsAg ELISA positive participants, 13 were positive and four were negative by HBsAg rapid test, while all samples tested positive with the rapid test were confirmed as positive by ELISA.
Supplemental material

{kind=link}
Percentage of antibody or antigen positives among transfusion recipients and controls. *p<0.05. HCV, hepatitis C virus; HEV, hepatitis E virus.
The serological profile indicating vaccination was significantly more often found in cases than controls in age groups 6–10 years (57/125; 45.6% and 26/112; 23.2%, respectively, p=0.001) and >10 years (51/104, 49.0% and 25/111, 22.5%; p<0.001; table 2). Controls more often lacked antibodies against both the core and surface antigens than cases in age groups 6–10 years (52/125, 41.6% and 67/112, 59.8%; p=0.005) and >10 years (27/104, 26.0% and 56/111, 50.5%; p<0.001).
Serology results stratified by age group
Anti-HCV antibody seroprevalence in transfusion recipients (8/299, 2.7%) was similar than in the control group (10/300, 3.3%; p=0.6). Anti-HEV IgG prevalence in transfusion recipients (22/293, 7.5%) was significantly lower than in the control group (36/284 12.7%; p=0.006). Likewise, human parvovirus B19 IgG antibodies were detected in 7 out of 297 (2.4%) transfused patients in comparison with 25 out of 295 (8.5%, p<0.001 in the control group (figure 1, online supplemental table)).
The seroprevalence of anti-HEV and of anti-parvovirus B19 was significantly higher in controls than cases among 6–10 year olds (7/125, 5.6% vs 14/112, 12.5%; p=0.05 and 1/125, 0.8% vs 10/112, 8.9%; p=0.003, respectively) (table 2). There were no significant associations between serology results and sex, diagnosis, thalassemia typing, number of transfusions received or volume received per transfusion.
Discussion
Without regular blood transfusion to control haemoglobin and haematocrit levels, patients with thalassemia develop severe and often fatal complications.27 However, multiply transfused patients are at risk of TTI, especially in resource-limited settings, where blood donor screening is not optimal. This study aimed to assess the burden of TTI in transfused children in Lao PDR.
Overall, we did not find a higher exposure rate among the transfused children compared with the control group composed of children who never had blood transfusion.
HBV prevalence is high in Lao blood donors (9.2% HBsAg positives among first-time donors and 3.9% among repeat donors as determined by ELISA).13 Although HBsAg positive blood is discarded, it is possible that HBsAg negative but HBV DNA positive blood (from ‘occult infected’ donors) enters the blood donation pool. Indeed, Lao blood banks do not screen blood by molecular techniques for HBV DNA and a previous study found 3.9% of donated blood was DNA positive (estimated lower limit of detection of the PCR was 20 IU/mL) but HBsAg negative using the AxSYM HBsAg V2 kit.12 Nevertheless, in the current study, we did not find evidence of increased exposure or a higher rate of chronic infections in multiply transfused children. This may reflect the low infectivity of blood from occult-infected donors28 or rarely from early window phase donations, appropriate screening of donor blood and/or the fact that the transfused children are supposed to receive three doses of HBV vaccine prior to transfusion. Higher vaccination rates in the transfusion group are also reflected by the high anti-HBs antibody seroprevalence as compared with non-transfused controls, especially in the older age groups, where non-transfused controls may have been born at a time when vaccination coverage was still low9 or where anti-HBs antibody titres may have decreased below seropositivity level (10 mIU/mL).29 Since mostly packed red blood cells with a reduced volume of plasma as compared with full blood are given in Lao PDR, passive transfer of antibodies is probably not playing an important role in our cohort of transfusion recipients.
Anti-HCV seroprevalence was not significantly different between the transfused group and controls (approximately 2.7 and 3.3%). This contrasts to studies in areas where HCV is highly prevalent in the general population. For instance, Egyptian patients with thalassemia had an anti-HCV seroprevalence of about 40% with an increase after blood transfusions.1 Blood donations in Lao PDR are screened for HCV and positive blood is discarded. The similar seroprevalence in the transfused and control groups in this study is likely due to the blood screening process and the moderate seroprevalence in the general population.10 The fact that exposure to HBV and HCV was similar in cases and controls suggests that infection occurs early in life, but is not related to blood transfusions during childhood.
Our previous studies found high anti-HEV seroprevalence in Lao adults—approximately 41% (57/139) in those who had and 18% (38/210) in those who had no contact with swine.16 Although HEV can be transmitted through blood transfusion,30 31 we did not find any increase in seroprevalence in the transfused group, suggesting that transmission of HEV via blood transfusion is either not very efficient32 or not very common in Lao PDR.
Anti-parvovirus B19 seroprevalence was lower in transfused patients than controls (2.4% and 8.5%, respectively). Thus, our findings contrast with other studies where transfusion recipients had significantly higher rates of anti-parvovirus B19 IgG positivity than controls.5 33 We cannot exclude that a few controls consulting the OPD and the allergy and immunology department of the hospital suffered from HEV or parvovirus B19 infection and already had detectable IgG antibodies and/or that patients with thalassemia pay in general more attention to hygiene and disease prevention due to their fragile condition.34 While our results do not suggest that HEV and parvovirus B19 infections through blood transfusions play a role in Lao PDR, further studies are required to assess the cost-benefit of screening blood donations for these two pathogens.
Conclusion
Our results did not suggest an important role of TTI in children from Lao PDR, but a long-term follow-up study of newly diagnosed patients could further clarify TTI burden. The significantly higher prevalence of the HBV vaccination profile in cases showed that the recommendation to vaccinate prior to the start of transfusions is at least partially implemented, although there is still room for improvement with less than half of the cases showing the serological profile suggestive of previous vaccination.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Lao National Ethics Committee (Reference number 038/NECHR 2016). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Deceased SB deceased.
Contributors VK, APB, CPM and JMH were involved in study design and drafting the proposal. SS, BS and SM were responsible for patient recruitment and SB coordinated the clinical aspects of the study. VK and BV were responsible for sample collection, VK also for data collection and BV for laboratory testing. VK, CJS, APB, CPM and JMH were involved in data analysis and interpretation. VK, APB and JMH prepared the article, the other authors reviewed the manuscript and CJS and CPM contributed revisions. VK is guarantor.
Funding This work was supported by the Luxembourg Ministry of Foreign and European Affairs and the Luxembourg Institute of Health (project 'Luxembourg-Laos Partnership for Research and Capacity Building in Infectious Disease Surveillance II').
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.