Article Text

Statistics from Altmetric.com
The efficacy and safety, including arrhythmia and sudden death,1,2 of intravenous methylprednisolone pulse (IVMP) therapy in patients with Kawasaki disease (KD) are uncertain.
We conducted a control study in KD patients with persistent or recurrent fever (⩾37.5°C) 48 hours after a single infusion of initial intravenous immunoglobulin (IVIG) 2 g/kg. At enrolment (day 1), the subjects were randomised to receive IVMP (30 mg/kg/day of methylprednisolone for three days), or additional IVIG (2 g/kg). Heparin was also continuously infused (15–20 units/kg/h) in the IVMP group. The study was halted prematurely because of adverse effects of IVMP when 22 patients were recruited; they accounted for 13% of KD patients treated with initial IVIG.
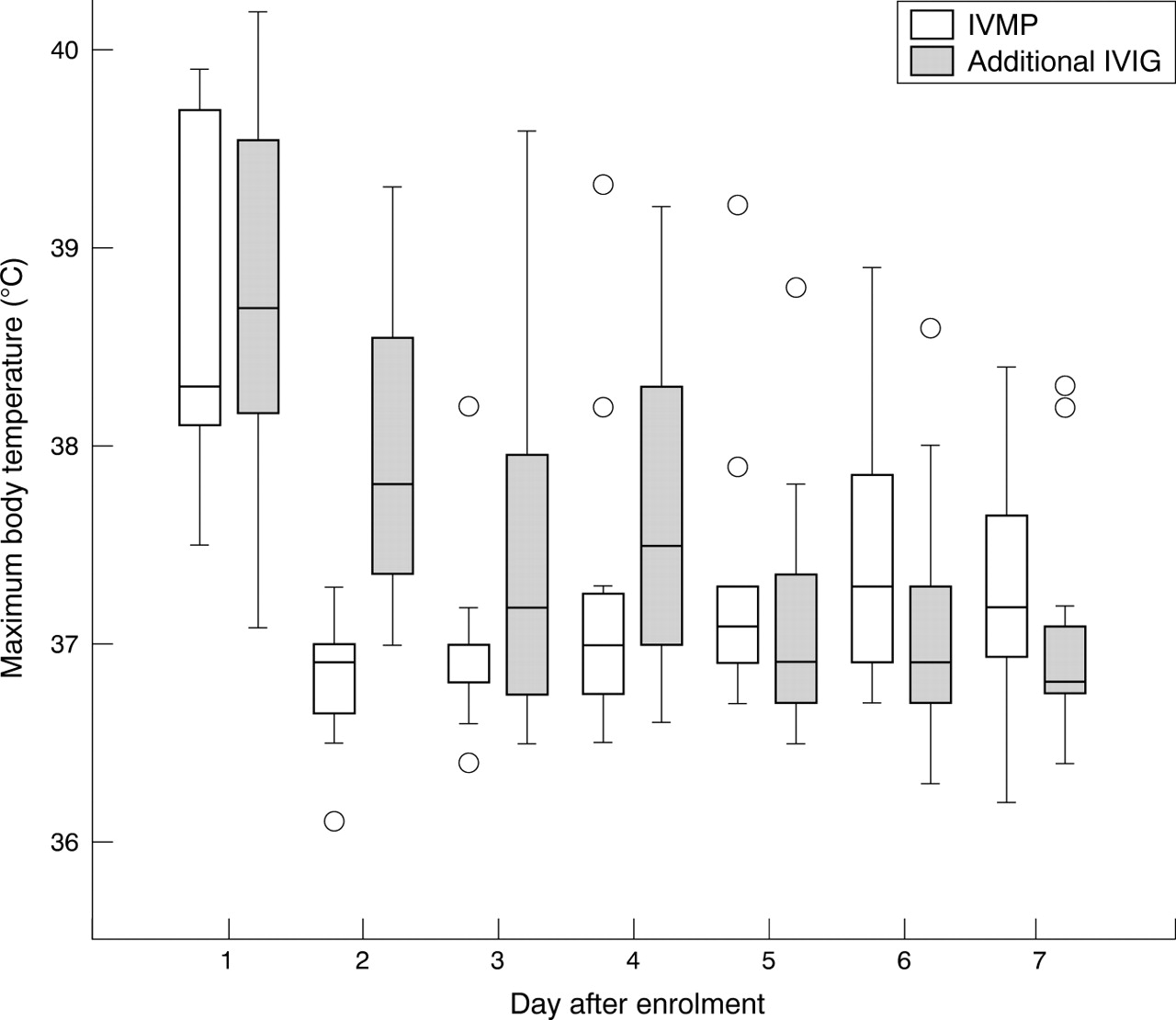
The antipyretic effect of IVMP was superior to that of additional IVIG on day 2 (p = 0.02, repeated measures analysis), but not on day 3 and later (fig 1). The fraction of febrile patients was significantly lower in the IVMP group until day 3 (1/11 v 8/11, p < 0.001, Fisher exact test), but not on day 4 and later (6/11 v 6/11). Coronary artery dimensions and the prevalence of coronary artery lesions (2/11 v 3/11) were similar in the two groups. Regarding adverse effects, sinus bradycardia and hyperglycaemia occurred more often in the IVMP group (table 1). Hypertension occurred in 91% of the IVMP group, but the fraction did not differ significantly, probably due to the small sample size. All of the adverse effects were transient. There were no convulsions, gastrointestinal symptoms, infection, malignant arrhythmia, or sudden death in any subjects.
Adverse effects

{kind=link}
Changes in the maximum body temperature attained each day after treatment with IVMP or additional IVIG. The starting day of IVMP or additional IVIG was defined as day 1. Body temperature dropped more rapidly in the IVMP group than in the additional IVIG group (p = 0.006, repeated measures analysis); the antipyretic effect of IVMP was superior to that of additional IVIG on day 2 (p = 0.02, repeated measures analysis), but not on day 3 and later. The upper and lower ends of a box show the first and third quartiles, and the line inside the box the median value. The upper fence of a whisker represents the largest value within 1.5 times the interquartile range above the third quartile and the lower fence of a whisker the smallest value within 1.5 times the interquartile below the first quartile. Values beyond the fences are marked with circles.
KD patients refractory to initial IVIG should be treated with additional IVIG,3,4 because IVMP induced faster but temporary resolution of fever and more adverse effects. Further investigations with steroid therapy are necessary to determine the indication and the appropriate dose in KD.
Acknowledgments
We are grateful to Mr Mitio Inokuti of Argonne National Laboratory for critical reading of an earlier manuscript.
Footnotes
-
Competing interests: none declared