Article Text

Statistics from Altmetric.com
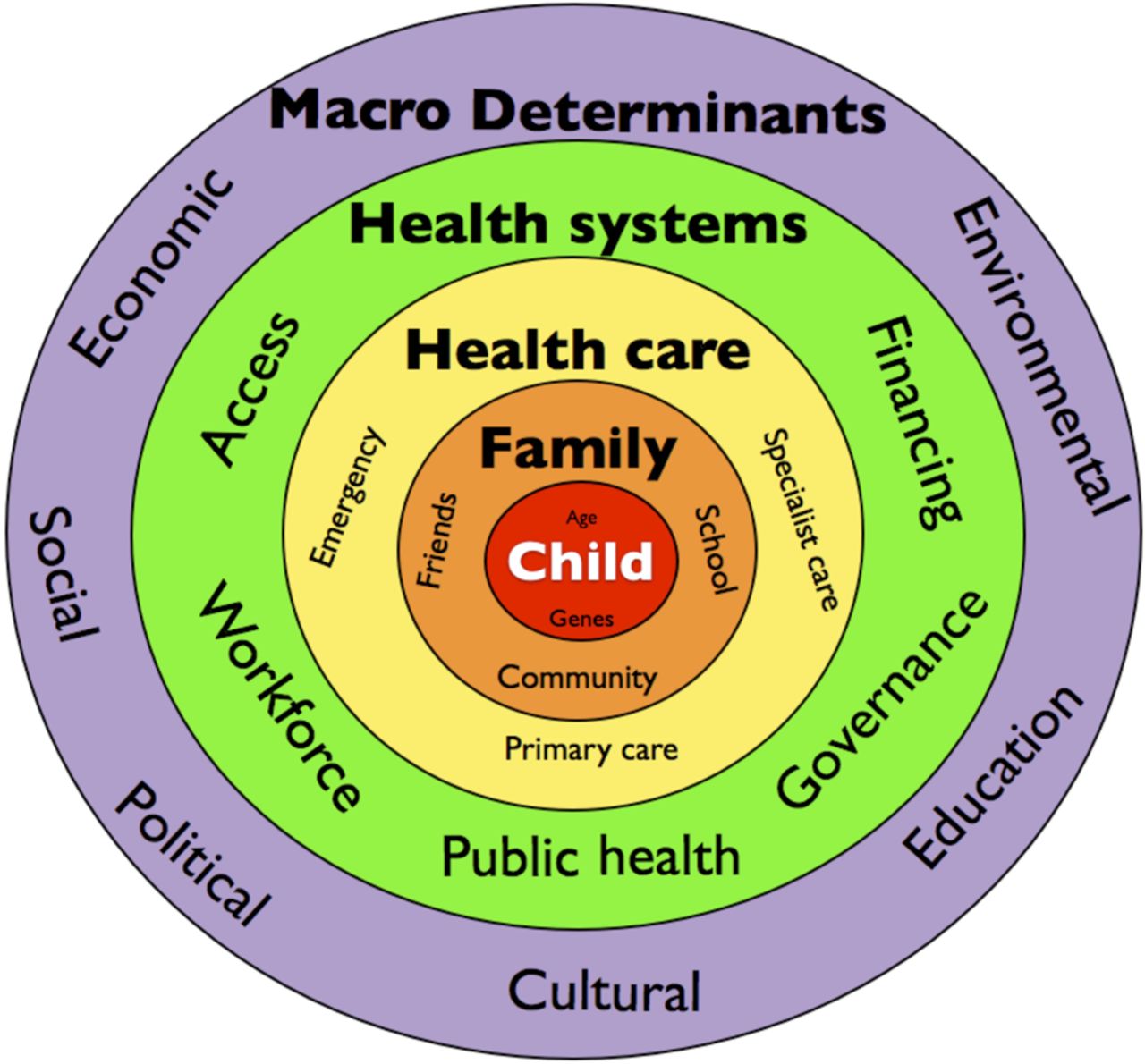
There is growing concern that the UK is not performing as well as it should in securing and promoting health for children and young people.1 The reasons behind the UK's child health problems are complex, including socioeconomic conditions and other upstream determinants of health, and health systems and healthcare factors, as shown in figure 1. A comprehensive strategy to improve UK child health should therefore include action across all the domains and determinants of health. Integrated care is about joining things up in order to meet health needs, and in ways that make sense to children and families. Therefore, it should make an important contribution towards improving child health. Although this hypothesis is plausible, and is the basis of a great deal of policy, evidence is still indirect and limited. A concerted effort towards improving healthcare and child health must be supported by a strong drive to improve children's health services and systems research.

Determinants of child health.
Why is integrated care needed?
Currently there is a mismatch between health needs, which are increasingly about chronic conditions (physical and mental), and the health system that exists to meet health needs. Problems in healthcare partly explain the mismatch. Services are still largely centred around urgent care, but despite the focus on these services quality is variable and sometimes poor, and demand continues to rise.2 ,3 Planned care for children with long-term conditions often takes second place, and management of children with long-term conditions is suboptimal, leading to reduced quality of life and increased costs as these young people move into adulthood. Furthermore, workforce data suggest that our model of healthcare for children is not sustainable, but more importantly it is not fit for purpose in terms of outcomes.4 The resultant combination of poor health, suboptimal care outcomes and inefficient services is unaffordable in both human and economic costs.5
There are considerable challenges in achieving an optimal balance between access and expertise in urgent care. And since urgent care takes precedence, this balance is crucial to ensure effective and efficient services with enough resource left for planned proactive comprehensive care for children with long-term conditions. All countries struggle with these challenges, and there is less evidence to guide optimal health service configurations than there should be. For example, the concept of a hierarchical service of primary, secondary and tertiary care was borrowed from education, where a linear progression through the system makes sense.6 However in health, the appropriate entry points to urgent and planned care can be in primary or secondary settings, and a linear progression through a service hierarchy is not always best. A joined-up approach to urgent and planned care, balancing access with expertise across settings, makes sense as the basis for integrating care. However, if we are effectively to optimise health, prevent disease and maximise well-being, we need to think beyond healthcare and do better in providing health promotion, disease prevention and health policies that address the upstream determinants of chronic disease.
Integrated care seems to hold the solution to many of the problems facing children's health services and systems in the UK and throughout Europe. It is defined by the WHO as health services organised and managed so that people get the care they need, when they need it, in ways that are user-friendly, achieve the desired results and provide value for money.7 Integrated care therefore seems to offer a way of adapting the health system to be more effective and responsive. Integrated care means rebalancing resources in favour of primary care and public health, through better configuring services within healthcare and between health and other sectors. There is a paucity of evidence, however, about how best to achieve integrated care for children and young people. A systematic review of integrated care models (in progress) has suggested significant limitations to many of the studies identified. Problems include poor quality methods and limited generalisability. For example, many cost-effectiveness studies were conducted in the USA with a fee-for-service and insurance-based system, so evidence is unlikely to apply to the National Health Service (NHS). The available evidence for integrated care models in children and young people, including chronic care models, transmural care and the medical home model, suggests that improved care processes, some outcomes and patient experience are possible, but there is as yet limited consistent evidence of improved outcomes.8 A welcome exception is a recently published meta-analysis of trials of integrated medical and behavioural care which demonstrated improved outcomes.9 Although the findings may not be wholly generalisable in the UK and Europe, the paper amply demonstrates the feasibility of high-quality research in children's integrated care.
A plethora of government and non-government documents, policies and initiatives about integrated care have been produced in recent years.10 Most of the national discourse on integration, however, focuses on the needs of the elderly. Since many older people are reliant on social care, and the effects of inefficient or over stretched social services are distinctly felt in healthcare, much of the policy around integration emphasises better join-up between health and social care. Children have different social and healthcare needs. The majority of children are well. They rely on their families for support, on education and universal health services to optimise their development and promote healthy lifestyles, and urgent care for occasional acute illness, and less frequently need specialist health and/or education services to address illness or disability. Although small numbers of children need social services and some may have high levels of need, this is the exception rather than the rule. This is illustrated in figure 2. A nuanced and distinct policy response to problems in child health is required.

Children and the elderly often depend on different sources of support when they are ill, so different policy responses are required.
What should integrated care mean practically for children and young people?
Children have the right to the highest standard of healthcare, and to a standard of living and social security that facilitates full physical, mental, spiritual, moral and social development.11 The UN Convention on the Rights of The Child provides a basis for our aim as children's health professionals to promote optimal health and development of infants, children and young people. As shown in figure 1, the forces that influence and shape child health and development stretch far beyond healthcare. Integrated care at its best ought to be about ensuring that health services are part of a whole system of prevention and care that is coordinated and comprehensive, and promotes the best possible chances for children. A life course approach to integrated care means that the distinct needs of each life stage are considered and catered for.12 These ideals can be conceptualised through four dimensions of integration that include health systems, wider determinants of health and healthcare:
Vertical: linking primary and secondary care into a unified team that overcomes unhelpful divisions between physical and mental health and achieves a balance between access and experitise that best suits children and young people.
Horizontal: linking health and education and social care for a whole child approach to care.
Longitudinal: linking services across the life course stages for smooth transitions.
Population: linking healthcare with public health for a comprehensive pathway-based approach including health promotion, disease prevention and reactive healthcare.
The four dimensions of integration are shown in figure 3, with exemplars for each early life stage linking to each other longitudinally. These are embedded within public health interventions and policies for the population to promote health, prevent disease and address the upstream and social determinants of health. The cumulative effect of comprehensively integrated services should be to ensure that children have the best possible chances of optimal health and development.13 The Family Friendly Framework offers such a whole systems approach to planning and delivering services based on a comprehensive approach to care, similar to an integrated or extended chronic care model. The objective is to achieve a service model that includes and optimises prevention, urgent and planned care, while fostering an active partnership between patient and healthcare team.14 ,15 Illustrative examples of how fully integrated care could better serve children's health are shown in the box (see online supplementary table).

Four dimensions of integration for infants, children and young people.
Supplementary table
What needs to change to achieve integrated care for children and young people?
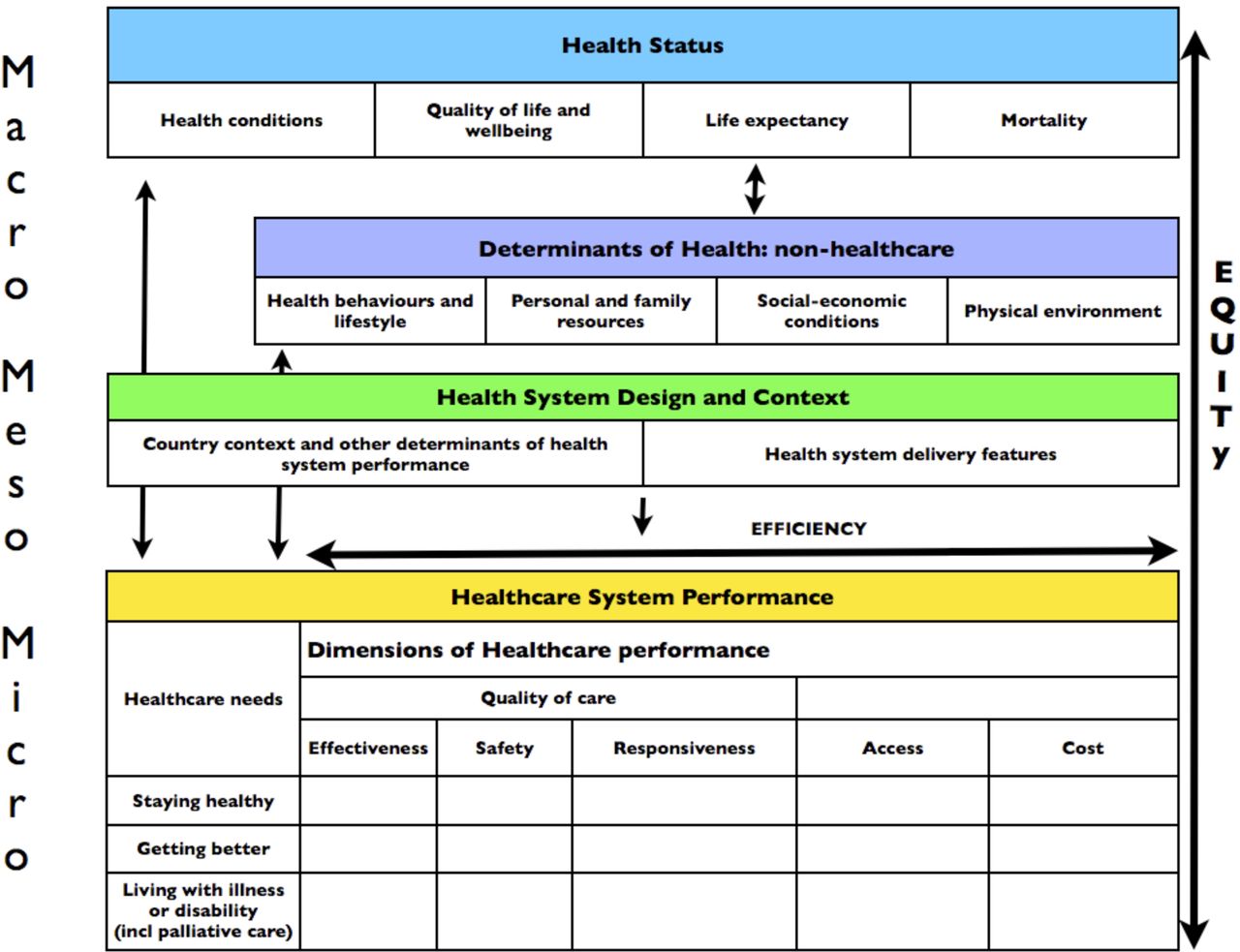
Aspects of health systems, non-healthcare determinants and healthcare should be considered to ensure that child health improvement strategies are comprehensive. These are illustrated in figure 4, an adapted health system performance assessment framework.16 ,17

Health systems assessment framework to guide a comprehensive approach to child health systems strengthening (adapted from Arah et al).
Health systems: important characteristics of health systems include universal coverage, freely accessible services, delivery system design that promotes prevention of ill health, supportive information technology to enable population health planning and management, electronic records and facilities to support self-management. Importantly, a coherent whole system that supports the comprehensive care of a population is needed.16 Although the NHS provides universal freely accessible care, the current delivery system design falls short in providing the conditions for optimal health promotion, effective use of information technology and a coherent whole strategy for child health. Moreover, the current system of fragmented commissioning, competing providers and numerous regulators lacks clear simple accountability for the quality of children's healthcare. Child health systems strengthening is made more challenging since children's health services, systems and policy research is still in relatively early stages, and there is no comprehensive set of valid, practical and comparable child health service quality measures.5 ,18
What change is needed? There are two main issues of health systems policy to be addressed. First, the tensions, expense and conflicts of interest that are a consequence of the purchaser–provider split and competitive tendering, and the gaps between providers and tiers of the health services—especially primary and secondary care providers. In many countries there has been a policy shift to abandon competition and focus on collaboration and integration among providers in order to improve efficiency and continuity.19 Second, the frequent tendency for policy to focus on the urgent, expensive and immediate needs of the frail elderly. It is apparent that the economic burden of caring for the elderly will always take the largest portion of health and social care budgets, but within the financial envelope that is available for children's health and healthcare, it is important that their different needs are recognised, and that children's policy has a distinct focus. Current financial incentives are not designed to maximise cooperation. No one healthcare model is likely to solve all the problems policymakers face in trying to shift the system from a reactive acute model of care to a proactive coordinated model of care that consistently delivers the highest quality of care. However, it is increasingly clear that enabling healthcare professionals to work across organisational boundaries and pool financial risk requires strong clinical leadership and a vision tailored to local need. Year-of-care financing mechanisms for children with long-term conditions and shared capitated budgets based on delivery of outcomes for specific populations, such as well children, may prove to be useful means of supporting cooperative working in the best interests of the child.
Finally, a framework for monitoring of outcomes, a system for reviewing results and an oversight mechanism with power to ensure accountability for the results and enable remedying action are needed to ensure continuous improvement.
Non-healthcare determinants: these include conditions to foster self-management, and all the public health interventions and policies that address social and economic determinants of health, personal and family resources and the physical environment.16 ,17 Although the current child health system and wider environment are delivering improvements in child health, the UK is failing to keep up with the pace of child health improvements that comparable European countries are achieving.20 ,21 European comparisons highlight the differences that policy choices can make to children's lives and health. For example, the UK disproportionately disadvantages its young; a greater proportion of whom live in poverty or social disadvantage than the elderly.20 ,22 ,23 However, other countries make macroeconomic and social protection policy choices that lead to more equitable outcomes.
What change is needed? Macroeconomic and social policies can save lives and promote optimal health and well-being. A cross-government strategy to secure children's health and well-being would focus on reducing poverty, inequalities and social disadvantage while strengthening the health system and healthcare services to meet the specific needs of children and young people.
Healthcare: healthcare qualities that enable an effective system include strong primary care delivered by multidisciplinary teams, integrated generalist and specialist care, coordinated care and population management.4 ,5 ,15 ,16 Delivering such integrated healthcare for children may require overcoming professional, organisational and financial barriers.
The most practical way to deliver integrated care is likely to be through physical or virtual colocation of services provided by a team of children's health professionals encompassing traditional primary and secondary care, physical and mental health and health promotion. All this could likely be achieved through community-based health and care centres such as the multispecialty community provider model or primary and acute care systems recently proposed.10 However, it is important to ensure a maternal child focus, such as exists in Sweden's child health centres for example.5 ,24 It is a matter of considerable concern that there is scant emphasis on the distinct needs of children and young people in developing new service models. The recent nationally profiled and supported Pioneer and Vanguard integration programmes, for example, have not promoted service development specifically for children.25 ,26
The current workforce configuration in the UK is still based more on traditional professional boundaries rather than the current and evolving needs of children. Doctors are trained to work in existing environment and structures rather than starting with a consideration of the needs of the majority of children. It is apparent that the vast majority of medical consultations for children are managed effectively by general practitioners. However, there is still a large number of children and young people requiring more paediatric expertise or clinical time than is currently available in primary care, but whose healthcare needs do not necessitate the skills of a specialist paediatrician or the facilities of a hospital. Many other countries meet these needs through a different skill mix that addresses the gap between primary and secondary care. There is a strong policy imperative to combine high-quality care with value for money, and considering these international models can provide essential insights.
What change is needed? Healthcare that is tailored to meet current and evolving needs of children and young people should emphasise health promotion, disease prevention and primary care-based treatment of acute minor illness and long-term conditions. It is inevitable that shifting care to the community and strengthening primary care will mean a reduction in emphasis on inpatient and hospital-based care. Bold policymakers and supportive financing will be required to ensure that the health system operates as a whole to serve the best interests of children. Flexible strong primary care models for children require a transformative approach to the health workforce.6 Options include paediatricians trained in general paediatrics, integrated care, public health and mental health which would remain an essential part of the hospital team but work in primary care networks. This model would support delivery of the newly released Facing the Future Together standards, for example by providing a link paediatrician for every general practice.27 Crucially, these paediatricians would work to complement and supplement, but not to replace the role of general practitioners in delivering a service outside hospital, providing more convenient and appropriate care for children and young people who do not need inpatient management or complex investigation and treatment. There should be scope to evolve a portfolio career over time with options for gaining credentials after completing specialist qualifications. Duration of training should be determined by the needs of children and young people rather than existing training pathways.
Health visitors, midwives, school nurses and others play a vital role in providing universal services for children in the community. There are worrying workforce shortages in several of these groups, as well as in the numbers of trained children's nurses, who are a key part of new ways of working, able to support children with acute care needs and complex long-term conditions in a range of environment including hospital, school, home, children's centres and primary care settings. The Children and Young People's Health Outcomes Forum strongly supports the concept of a ‘children's nurse fit for the future’, trained in physical health, mental health and learning disability.28 Such nurses would have considerable flexibility to develop their careers, specialising in diverse roles ranging from paediatric or neonatal intensive care, to health visiting, school nursing or more general hospital or community-based children's nursing.
It is outside the scope of this paper to elaborate the full spectrum of essential professionals who would also form part of this networked team, from community pharmacists to child and adolescent mental health services staff and allied health professionals. However, it is equally important to note that many professionals outside health such as teachers, youth workers, social workers and nursery staff have a profound effect on children's health outcomes and life chances, and all need shared core competencies in children's health and care.
Making it happen
Improving child health will require strengthening health systems, non-healthcare determinants and healthcare for children. A fully comprehensive approach to integrating care is likely to help achieve all three, delivering maximal health gain for the population through focusing efforts on the health concerns of the majority of children. This is illustrated in figure 5, adapted from Geoffrey Rose.29 Translating these ambitions to reality will be difficult, and in the short term will require investment. This is extremely challenging when providers and commissioners of care face significant and mounting pressures to deliver improved outcomes and greater efficiencies. Achieving these things without rigorous comprehensive evidence is even more challenging. Integrated care services may be expensive to develop and test, and there may be a period of increased costs while improvements are confirmed or refuted through evaluation. The return on investment may be slow. Integrated care may deliver better quality of care and at less cost, but we do not yet fully know the answers. There should be fiscal space to test new services. Children's health services and systems research is still an underdeveloped field, and although progress is slow there seems to be a growing recognition that capacity building and targeted research funding are essential.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Shifting the population distribution of health by focusing on the needs of the largest part of the population delivers maximal health gain.
A cross-government strategy dedicated to the rights and needs of children would help ensure that policies affecting children receive the attention, coherence, budget and accountability they urgently need. To be maximally effective, a prominent and powerful policy lead for children should be required at all governance levels: from national to local government, from health and well-being boards to clinical commissioning groups.
Beyond integrated care other important elements are needed: aspiration and ambition. Many of the problems outlined here have potential solutions, yet progress seems slow. As a country we should aim higher for our young people. We can and must provide the best possible conditions for children to survive and thrive.
References
Footnotes
Contributors IW conceived the paper and wrote the first draft. CL and HC contributed to it. IW is the guarantor.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.