Article Text

Statistics from Altmetric.com
Introduction
Family Integrated Care (FIC) is a new model of neonatal care which supports parents to be primary caregivers, as partners with the clinical team.1
The inspiration for FIC comes from lower resource settings where families provide care through necessity rather than choice.2 3 This approach has been adapted for modern neonatal intensive care by pioneering FIC teams in Canada, Scandinavia and the UK. Trials in preterm infants have demonstrated improved rate of weight gain, reduced parental stress and shorter length of stay.4 5 By supporting and combining the benefits of breast feeding, kangaroo mother care (KMC) and parental presence, FIC may have even greater long-term benefits for infants and their families.6
FIC builds on the foundations of Family-Centred Care, a well-established approach with accepted standards supported by Unicef and the neonatal charity Bliss.7 8 FIC takes parental involvement to a new level placing families at the centre of care and empowering them as primary caregivers (table 1).
Comparison of FCC and FIC at RHC, Glasgow
Though the concept of FIC is intuitive and the potential benefits compelling, delivering this model of care may be challenging. We took on this challenge in our neonatal unit, the largest unit in Scotland with approximately 1000 admissions per year and over 200 staff. Our patients include extremely preterm infants as well as those requiring specialist medical and surgical care including extracorporeal membrane oxygenation (ECMO). Implementing FIC in a unit of this size and diversity has its own specific challenges, but has been hugely rewarding. In this article, we share our approach and lessons learnt, and describe the transformative effect on families and staff.
The challenges of implementing FIC
FIC means not just physically involving families, but equally importantly changing the culture and relationships with staff.9 10
Staff engagement is potentially the greatest challenge. FIC requires a change in professional roles, particularly for nurses who must transition from direct caregiver to become mentor, teacher and friend. In our unit, as in others, many staff already felt overburdened and stressed by their work, blunting enthusiasm for change.11 12 Staff also had reasonable concerns about patient safety, the legal responsibility for care, or that the needs of the family might overshadow those of the baby. Others felt that they lacked the knowledge and confidence to teach and support parents.13
There are parental barriers too. Families may be busy due to work and family life. Lack of accommodation, facilities, parking or money prevents them from being present round the clock to care for their baby.14 15 There may be communication issues, if families cannot understand the language or terminology. They may feel uncomfortable and unwelcome, or too stressed or depressed to be fully engaged carers.16–19 Most importantly, they may not have the knowledge, skills, support or confidence to care for a sick infant.20 21
Third, there may be institutional barriers. In the busy neonatal unit, communicating and coordinating change across all staff and families is time consuming. Traditional hierarchies may stifle engagement and innovative thinking. Any additional resource, even to drive quality improvement, may be hard to identify.
We encountered many of these barriers but discovered that most were surmountable by enabling staff and families to lead change and apply innovative approaches to FIC.
A grass roots model of FIC
We formed the Helping Us Grow Group (HUGG) in 2016 to develop our model of FIC. HUGG is a unique collaboration of families together with nursing, medical and allied heath staff in the neonatal unit. We believed that FIC could not be imposed as a ‘top-down’ initiative. Instead, our approach was ‘ground up’, engaging staff and families in all stages of planning and implementation.22 23 Three key principles guided our work: listening to parents and staff, empowering them to lead change and applying innovation.
Listening to families and staff
Active listening has been the most powerful element in our model of FIC. We learnt to put aside assumptions and hear the views of families and staff.24 This was critically important to understand the practical needs of families, to create new collaboration between staff and families and to engage all staff giving them a voice in shaping our work.
We use monthly ‘HUGG meetings’ to listen to staff and parents. These informal, non-hierarchical meetings are open to families, past and present, and all staff in the Unit, who come together to share experiences and develop ideas. They have had a profound effect. Families feel valued and part of our team. Staff heard directly how it feels to be a parent in the Unit, and are motivated by this. For any team embarking on FIC, we recommend taking the time to regularly sit down with families and hear their voice.
We also created surveys, in electronic and paper format, to listen to those staff and families who were unable to attend meetings. By gathering everyone’s opinions, we formed a consensus model of FIC and hoped to reassure staff that change was guided by them.
Empowerment
Empowering staff was the next step in our model of FIC. They create the environment and relationships to support families as carers. Many of our ‘early adopters’ were staff nurses, who were willing to challenge current practice to improve care. HUGG allowed them to develop as leaders by bringing them together, inspiring them with visits to other FIC centres, listening to their ideas and giving them permission and support to work across traditional groups and hierarchies.
Not all staff were ready to embrace FIC at first. Some worried that FIC would be imposed without consultation, that parents would be trained to perform complex care (such as blood-taking or endotracheal suction), or that it was a strategy to reduce nursing numbers. We learnt to slow our pace, listen to everyone’s views and took every opportunity to have informal, honest discussion with colleagues about FIC. We used ‘myths and truths of FIC’ posters to dispel misconceptions. We also shared powerful positive feedback from families, in our meetings, newsletters and information videos sent by email to all staff. Opinions began to change as staff saw the benefits for families, and also for themselves as part of more cohesive, social and happier team.25 For those staff with ongoing concerns, a simple but important question often helped: what would you want if you were a parent in the neonatal unit?
Empowering families is also key to FIC, both as primary caregivers for their baby and as team members working with staff to design and implement our model of FIC.26 The simple process of listening to parents, at HUGG meetings in particular, gave them power to shape our model. They helped us develop a practical framework and innovative ideas to empower all families as primary caregivers.
Implementing innovative FIC
We identified five key areas for implementing FIC. These were based on the ‘Four Pillars of FIC’, described by the FIC team at Mount Sinai Hospital, Toronto (www.familyintegratedcare.com): parent education, staff education, peer-to-peer support, and resources and environment. To these we added a fifth area of FIC of our own: communication.
Subgroups of staff and parents formed to lead improvement in each of these areas, coordinating their work using WhatsApp to communicate rapidly across our large and busy staff.27 Each subgroup was encouraged to think ‘outside the box’, developing innovative solutions to the challenges of FIC, as discussed in more detail below and summarised in table 2.
Five areas of FIC implementation at RHC, Glasgow
Communication
To improve communication, we introduced simple shared whiteboards at each cot space for families and staff to leave messages. This ‘frugal innovation’ had a profound effect, creating a new connection, and as one family put it ‘a voice for our baby’.28
Another idea came from a father who asked if we could send short videos of his son when he could not be in the neonatal unit. We worked with a commercial provider, and local governance team to develop and pilot a system for families (www.vcreate.tv/secure-video-messaging). Staff create short messages, often overnight, and send these securely to parents. Receiving a video message reassures families and helps form a connection with staff. Mothers report that receiving videos of their baby reduced their anxiety, helped them express breast milk and sleep.
Parent education
Parent education is central to FIC. To empower parents with the skills and knowledge to be primary carers, we organise daily family awareness sessions (figure 1). Topics are suggested by parents and sessions are led by nurses, nursing assistants, physiotherapists, pharmacists, dieticians, psychologists, neonatologists and ‘graduate’ parents. Sessions are informal with time for questions and discussion. All parents and family members are welcome to attend, to learn new skills and support each other.29

Family awareness sessions, example of monthly calendar. Sessions are suggested by parents and led by staff, bringing parents together to learn, share and support each other. NICU, neonatal intensive care unit. Source: Images are owned by Helping Us Grow Group (HUGG), Royal Hospital for Children, Glasgow. (Permission for publication is granted on behalf of HUGG).
Parent feedback from initial sessions was excellent, however attendance was variable. Families told us that they often forgot to attend. Our solution was to send parents an automated text message reminder (www.getflorence.co.uk) before each session and follow-up texts with links to relevant online resources including breast feeding support and resuscitation training.30
Peer-to-peer support
Enabling parents to meet, share experiences and support each other is an important component of our FIC programme.31 Many families have developed strong and lasting connections after meeting regularly at our family awareness sessions. One mother told us that these sessions were the ‘only sane hour of her day’.
We also organise an annual reunion party for ‘graduate’ families. These maintain ongoing relationships, celebrate the progress of former patients and are an opportunity to gather parents’ views and engage them as ‘veteran parents’.
Staff education
From the outset, staff told us they needed education and support to provide FIC. However, in view of initial resistance to FIC, we elected to take a gradual, stepwise approach, rather than imposing a broad training package. We started by focusing on the one element of care that 100% of staff agreed parents should perform KMC. We were surprised how quickly attitudes and practice changed. Initially, only 33% of staff reported feeling confident to support KMC. One month later, 75% of families were performing KMC, supported by staff. No significant intervention had been made in the meantime. We believe that simply asking the question ‘nudged’ staff to reflect and change their own practice.32 To test our theory, we asked if it was possible for all families to hold their baby. We set this friendly challenge on Christmas Day and were delighted when staff proved it could be done, and even created a video of the day to share with their colleagues.
Resources and environment
We wanted to create an environment where families feel at home, to encourage them to be present and involved. Parents told us they became anxious and frustrated waiting at the security door. We installed a biometric (fingerprint) scanner so parents could let themselves in, reinforcing the message that parents are not visitors.
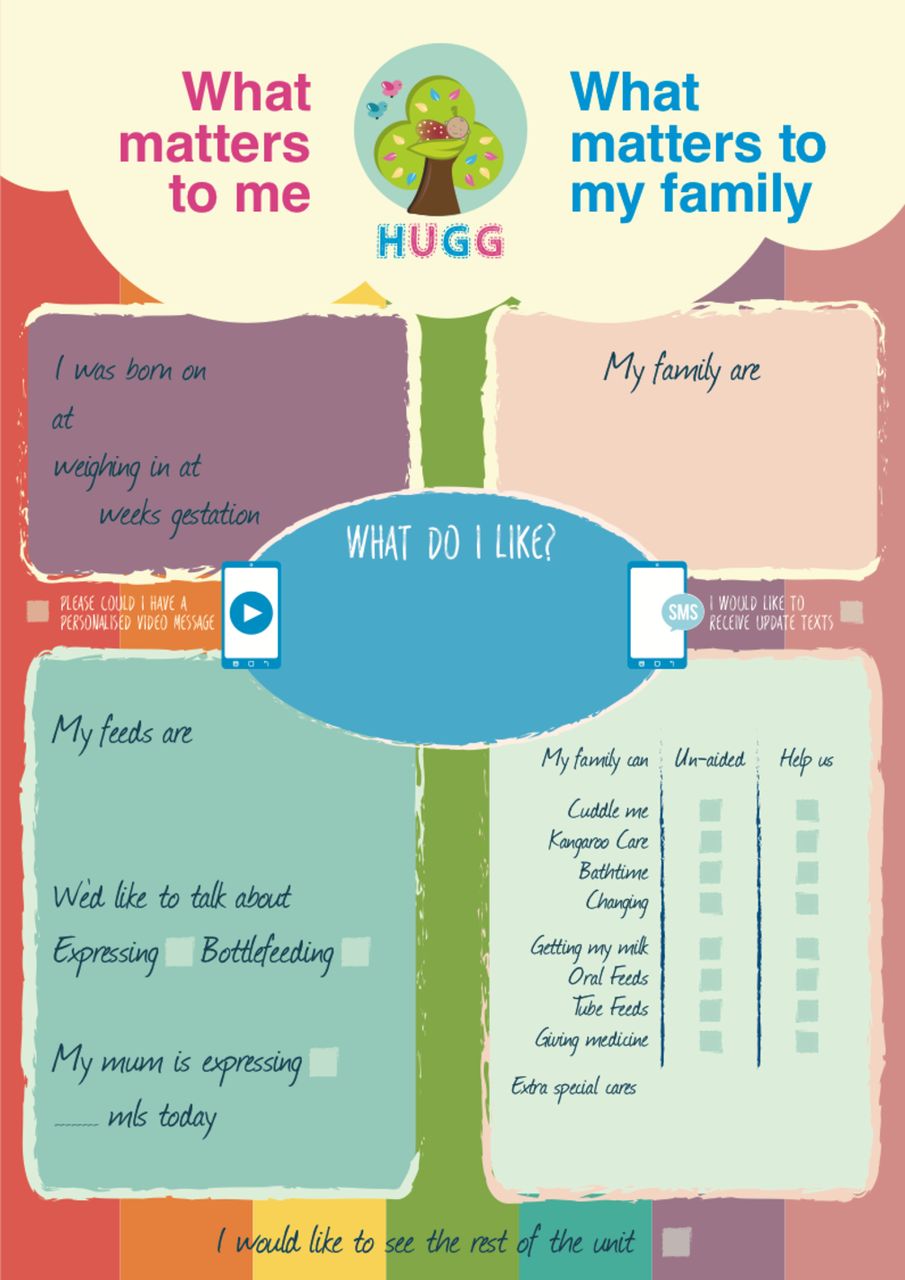
We also engaged parents in the design of resources in the Unit. They chose our name and logo, and designed cot-side family update charts (figure 2). These charts are completed daily by parents and act as highly visual prompts for staff. They are simple but effective, empowering parents to indicate which care they want to provide for their baby and request training when they are ready.
{kind=link}
{kind=link}
Family update chart. A concept and design by parents to support family involvement in every baby’s care. Source: Images are owned by Helping Us Grow Group (HUGG), Royal Hospital for Children, Glasgow. (Permission for publication is granted on behalf of HUGG.)
As staff acceptance of FIC increased, we felt ready to address more thorny issues including developing our policy of unrestricted 24/7 parental presence. Nursing handover was a particularly divisive issue, 21% of staff felt parents should never be present, 19% felt they should always be present during handover. Again, listening was key to addressing this impasse. We surveyed all nursing staff and used their ideas to create a new policy that supports parents to be present but includes procedures to ensure safe handover of confidential information.
Similarly, we grappled with parent involvement on ward rounds. We wanted to support their active participation but worried about confidentiality. Staff could not agree, but parents gave us a workable solution. The majority told us that they did not mind other families being present, had no interest in eavesdropping and understood if they were asked to step out. They favoured a flexible, pragmatic policy and trusted staff to manage this.
The cost of FIC
FIC need not be expensive. Our team were motivated to develop and spread our work in addition to their normal clinical duties. In doing so, we hoped to embed FIC in everyone’s normal practice. We continue to assess the long-term potential of FIC to pay for itself by improving long-term outcomes and reducing length of stay.
The impact of FIC
We use quantitative and qualitative measures, including structured interviews and electronic surveys to assess our work. Between 2015 and August 2017, we have seen consistent and widespread improvement. Parental reporting of being involved in care increased from 76% to 89%, of being with their baby whenever they wanted increased from 56% to 73% and the proportion who felt at home in the unit increased from 83% to 92%.
We have also learnt to manage expectations, acknowledging that participation is an individual choice of each family and tailoring our support to suit them. We celebrate and share our successes, in newsletters, our WhatsApp groups, and using video messages for staff too. These are an important opportunity to acknowledge the team’s achievements and engage other staff.
The change in culture in our unit is hard to measure but just as real. There is a new common sense of purpose, collaboration and cohesion, which has been very timely in our large and newly amalgamated Unit. As we grow in skills and experience together we are creating a happier unit.33 We are discovering, as others have before us, that the ‘family’ in FIC extends to staff too.
Acknowledgments
We are grateful to all staff and families of the Neonatal Unit at the Royal Hospital for Children, Glasgow, for their contribution to our work. We thank Glasgow Children’s Hospital Charity, Treasured MemoRory’s, VCreate and Bliss for their support, and the FIC teams at Mount Sinai Hospital Toronto, St James’ University Hospital Leeds, Birmingham Womens’ Hospital, Imperial College London, and Neonatal Services Swansea for sharing their experience. We also extend special thanks to Nashwa Matta, Emma Gallacher, Ros Montgomerie and Cate Nicholl for their helpful comments on this manuscript.
References
Footnotes
Contributors All of the authors contributed to the planning and writing of this manuscript. JW and AB designed the artwork presented in the figures. All of the authors have seen and approved the original and revised versions of this manuscript.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.