Article Text

Statistics from Altmetric.com
Bilateral cerebral palsy
Gradually developing deformity can be an insidious complication of bilateral cerebral palsy and it is one which can all too easily be overlooked by the paediatrician already coping with the many other developmental, social, and educational problems presented by these children and their families. Although the orthopaedic management of some deformity can be deferred, this is not so for all deformities. Hip and spinal deformities can benefit from early intervention.
Gradually developing hip instability
In the past, gradual hip subluxation, often leading to dislocation, has often been referred to as ‘developmental dislocation’, but this term has become associated with congenital dislocation of the hip and it is confusing to continue its use in cerebral palsy and similar situations where there is no primary abnormality of the hip joint. The medium to long term consequences of increasing hip deformity are subluxation/dislocation of the hip. Subsequently, loss of hip flexion causes kyphotic sitting with an increased risk of spinal deformity and, in a significant number of children and young adults, nursing/daily living problems increase, often accompanied by hip pain.1 Asymmetrical deformity will cause pelvic obliquity with a greatly increased risk of scoliosis.2 The hip of a child with hemiplegic cerebral palsy appears to avoid this complication, although a child diagnosed as having ‘hemiplegia’, but in reality having a markedly asymmetrical bilateral disorder, can be affected.
From our review of the children who had attended one tertiary referral orthopaedic clinic over a period of 17 years and of the publications relating to hip problems in cerebral palsy, it was obvious that certain basic information from a prospective population based study of this complication was lacking and so the incidence and natural history were not known, although the severity of cerebral palsy and the age of pulling to stand were useful indicators of risk.3
Reasons for surveillance and early management
There is a body of opinion that considers the acetabulum to be more able to develop a stable socket for the femoral head if the head is well located (‘centred’) before the age of around 4–5 years.4-6 It has also been noted that children who acquire their encephalopathy after that age rarely develop gradual hip instability, however severe their movement disorder.3 Thus it seems important to be able to refer children with hips at risk for orthopaedic management in time to allow the orthopaedic surgeon (by whatever method) to ‘centralise’ the femoral head by that age.
The study
Paediatricians, physiotherapists, and orthopaedic surgeons within the former South East Thames Health Region were asked to notify our register of children with bilateral cerebral palsy born from 1989 to 1992 to mothers resident within the health region at the time of the birth (all ethnic groups included). The primary purposes of the study were to establish the prevalence of hip dysplasia, to collect data on its natural history, and from that data create a surveillance protocol for paediatricians allowing early referral for orthopaedic management.
All children with bilateral cerebral palsy were included. The term cerebral palsy has been taken to include all non-progressive disorders of movement and posture caused by a defect or lesion in the brain before 18 months, corrected for gestational age, and not part of another syndrome which has a motor component. Any child who had cerebral palsy, but who also had a disorder which might affect musculoskeletal development or structure, was excluded.
PREVALENCE OF BILATERAL CEREBRAL PALSY
The estimated prevalence varies, but for our current prospective population based study in the former South East Thames Health Region it is 1.7/1000 live births for 1989–91 inclusive (a total of 262 children).
Inevitably, some families had moved out of the health region before diagnosis, thus the prevalence figure is a minimum prevalence for bilateral cerebral palsy and so (perhaps) the quoted percentage incidence of hip problems within this population may be slightly too high. Nevertheless, the actual number of problems found by 5 years of age shows the extent of this complication and the service needed to manage it.
Although this sample encompasses the whole range of problems met in such a population, these surveillance measures are not intended to cover all eventualities. They are being formulated for the sole purpose of selecting for orthopaedic assessment those hips which are subluxing/dislocating secondary to the child’s cerebral palsy, thus events such as congenital dislocation, traumatic disruption of the hip, and those few hips of children with cerebral palsy which dislocate in the first few months of life are excluded.7 In this study three hips (in two children) had congenital dislocation and no other hip has dislocated by 18 months, although one right and four left hips had a migration greater than 50% at that age.
MEASURING SUBLUXATION/DISLOCATION
For children with cerebral palsy the most commonly used measure for subluxation is the migration percentage—that is, the percentage of the bony width of the femoral capital epiphysis which falls lateral to a line drawn vertically from the bony lateral margin of the acetabulum, usually called Perkins’ line, on an A/P pelvic radiograph (fig1).4 8 9 The migration percentages for a normal population have been published and the original data from that study have been made available to us.10 Abstracting data for the age group 15 months to 5 years, the maximum recorded migration was 23%, the 98th centile was 19% (left) and 17% (right), and the median 0%. For this normal population the mean migration for girls was slightly higher than for boys. A hip is usually considered to be subluxed if the migration is equal to or greater than 33%.
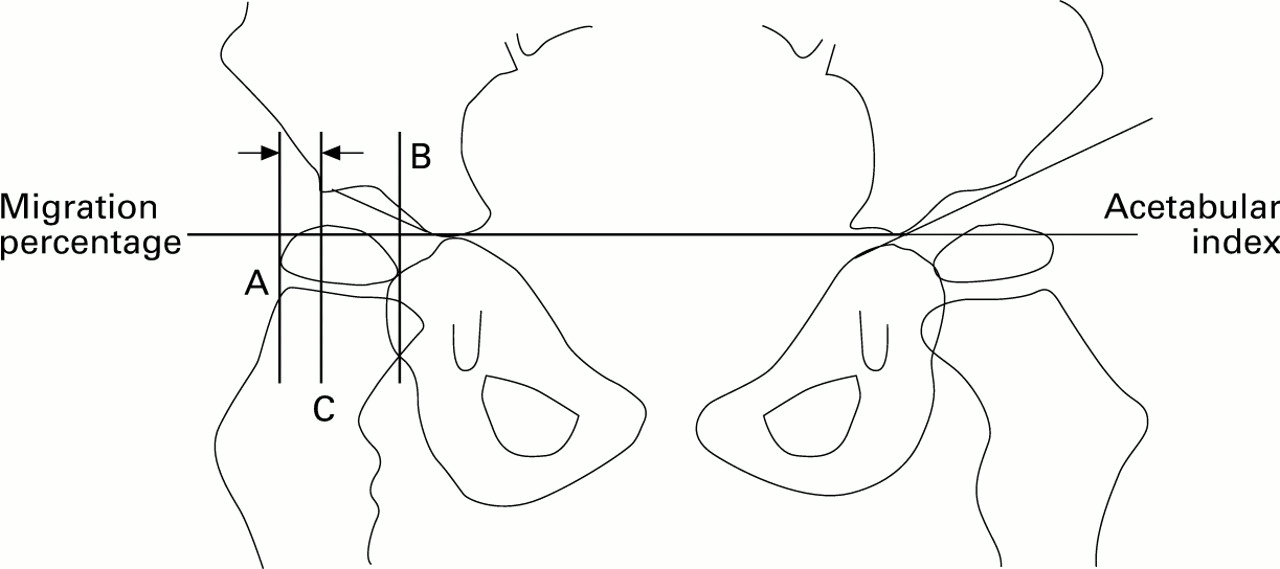
Measurement of migration percentage and acetabular index. Migration percentage = (AC × 100)/AB. The acetabular index is measured in degrees.
MEASURING DYSPLASIA
The development of the acetabulum is separate from, but intimately associated with, the position of the femoral head within it. There are a number of methods of measurement, some of which were developed for monitoring congenital dislocation, but the method most commonly in use for cerebral palsy is the acetabular index (fig 1). Although this measure may have great relevance for the orthopaedic management of these hips, up to the age of at least 30 months it appears from our data to have a poor correlation with hip state at 4–5 years of age. In spite of this it can be a useful prognostic guide at the extremes of the range, as discussed later.
Before entry to the study all the children were examined, usually in their home, and informed parental consent was obtained. Radiographs were obtained (A/P pelvis to show hips in a standardised position; fig2) at 18, 24, 30, 48, and 60 months corrected for gestational age. To avoid repetition throughout this paper, all ages are corrected for gestational age. Every six months from 18 months to 5 years questionnaires were sent to the child’s physiotherapist; it is from these that the locomotor data were obtained (see later).

Position of the children when the radiographs were taken. Note that the aim is to have the legs near parallel to each other in neutral (for abduction/adduction). If there is fixed or hypertonic flexion of the hips, the pelvis should be correctly positioned by allowing sufficient hip flexion.
Twelve of the 178 registered children born in 1989–90 have died and 156 of the surviving 166 children have been radiographed. Their 745 hip radiographs have been measured and the hip migration percentages and acetabular indices recorded.
Summary of findings
In this context a ‘hip problem’ is defined as: (a) an orthopaedic surgeon has operated on that hip; (b) an orthopaedic surgeon has prescribed an abduction orthosis to reduce subluxation or to prevent likely dislocation; or (c) the hip has migrated >32% (subluxed) between 4 and 5 years of age.
PREVALENCE OF HIP SUBLUXATION/DISLOCATION
By 5 years the current prevalence of hip problems in this population was 31% of hips in 40% of children (fig3).

{kind=link}
{kind=link}
{kind=link}
Outcome at age 5 years for the hips using radiographs of the surviving 166 children. *HASO = H ip A nd S pine O rthosis, prescribed by some orthopaedic surgeons to control hip abduction/adduction (and to give trunk support).
PROGNOSIS FROM 30 MONTH DATA
Data collected at 30 months correlated much better with the four year hip state (r = 0.72) than those at 18 and 24 months (r = 0.58). Table 1 shows the risks of a hip problem by 5 years related to the data collected at 30 months, from which it is apparent that any migration over 15% at 30 months needs careful watching, especially in boys. These children have not yet been followed beyond 5 years. There are separate risk figures for laterality and sex. The figures given show what happened in this cohort; it is not known how general these data are to other groups of children with bilateral cerebral palsy.
Percentage risk of a hip having a problem between the ages of 4 and 5 years when the migration percentage at 30 months (corrected for gestational age) is in the range shown in the left hand column. Risks are shown separately for side and sex
WALKING
By 30 months, 21% of the children could walk 10 steps unaided, with below knee orthoses if needed, none of whom has had a hip problem, which may be why children with uncomplicated congenital hemiplegia do not have hip instability as they all walk by this age. Between 31 and 60 months, 17% of the children walked (as defined above), of whom 20% had a unilateral hip problem, no child being affected bilaterally. By the age of 5 years, 62% of the children had not walked. Fifty eight per cent of these children had a hip problem (44% bilateral and 14% unilateral).
ACETABULAR INDEX
The acetabular index at 30 months does not correlate well with the migration percentage at 4–5 years. Using first order partial correlations controlling for the migration percentage, the acetabular index at 30 months correlated poorly with the ipsilateral migration percentage at 4 and 5 years (r < 0.25 for all). However, all hips with an acetabular index of 30° or greater at 30 months had a hip problem by 5 years.
LATERALITY
The right and left hips at each study age have been statistically similar populations for both migration percentage and acetabular index, although the rate of certain developmental changes appears to differ.
SEX
From 18 to 30 months girls have slightly higher acetabular indices (a mean difference of only 2°), but significantly higher migration percentages than boys. By 4 years of age these differences have disappeared.11
‘SECURE’ HIPS
So far at 30 months for either sex no right hip with an acetabular index <17° or migration <7%, and no left hip with <12° acetabular index or <6% migration has been at risk by 5 years of age.
Suggested surveillance programme
(1) Clinical examination for hip state is insufficient; all children with bilateral cerebral palsy require a radiograph.
(2) It is possible to radiograph the hips too early as the radiograph may not yet show the signs of the problem to come. This may act as a false reassurance that there will be no problem.
(3) Provided there is no earlier clinical sign of a hip problem, a hip radiograph may be delayed until around 30 months of age.
(4) Should the migration or acetabular index be excessive, a radiograph at 30 months allows ample time to refer the child for an orthopaedic opinion before acetabular dysplasia is well established.
(5) Radiographs should be taken in a standardised position (fig 2). There are two reasons for this. (a) The measure of migration percentage is influenced by abduction/adduction of the femur and so only comparably positioned radiographs can show change over time9 12; also, the risk figures in table 1 relate only to the femoral shafts being within approximately 10° either side of neutral abduction/adduction. (b) The measures taken from the radiograph are influenced by pelvic position13 14—both by pelvic lordosis or kyphosis and by rotation about a vertical axis. Provided the radiographer understands what is wanted, correct positioning is not difficult; indeed a physical difficulty positioning the child (as opposed to behavioural) may be taken as pathognomonic of the need for orthopaedic referral.
(6) Intervals between repeat radiographs for hips at risk. The aim of this surveillance is to allow early referral to an orthopaedic surgeon experienced in the management of these hips. Therefore surveillance cannot solely be a paediatric decision and the whole surveillance procedure needs discussion with the orthopaedic department. Our experience, however, indicates that changes can develop rapidly at this age and, if a hip is causing concern, it would be unwise to defer a follow up radiograph much beyond 6 months as migration increases rapidly once above 50%.
Conclusions
The need for such guidelines is based on the known morbidity of progressive hip subluxation and the need for postural management and/or surgery. The assumption that earlier detection would reduce the need for the more extensive surgical procedures is implicit, but, of course, this assumption has not yet been tested. Consequently, it is important to emphasise that such guidelines cannot be regarded as a legal requirement of managing children with cerebral palsy.
The management of hip problems in cerebral palsy is a highly specialised area of orthopaedics which may not be available in every district, but which should be part of the complex disability service in a health region.
Acknowledgments
This study is supported by SCOPE and Mencap City Foundation.