Article Text

Statistics from Altmetric.com
Unilateral and bilateral involvement of the temporomandibular joint (TMJ) and subsequent growth disturbance of the mandibula is a common feature in juvenile idiopathic arthritis (JIA).1 The prevalence varies between 17% and 87% depending on the subtype of JIA.2–6 No conclusive measures for local disease activity are found. Arthritis of the TMJ is usually not associated with pain, and clinical signals, such as deviation of the jaw, impaired opening of the mouth, absence of translation, crepitation, or clicking during palpation, are usually scarce, which explains the delay in diagnosis.7
The TMJ consists of fibrocartilage, hyaline cartilage, and synovial membrane like other joints. The growth centre of the mandible is located on the articular surface of the condylar caput instead of more distal to the joint,8 therefore the TMJ is more vulnerable to damage of the surface.
Arthritis may cause rapid condylar destruction as the following case history illustrates.
CASE REPORT
A 7 year old girl with arthritis in wrist, ankles, and some joints of hands and feet was diagnosed with rheumatoid factor negative polyarticular JIA. She was treated with non-steroidal anti-inflammatory drugs, sulfasalazine and methotrexate. The wrists and hands, especially, showed active arthritis with a gradual deterioration of function. Radiological evaluation disclosed no erosions.
At a routine check up the patient—then 11 years of age—complained of pain when she opened her mouth with impairment of biting, a clicking sound in her left TMJ, morning stiffness, impaired mastication, and decreased maximal opening which had been present for one month. Results of the immediate orthodontic evaluation were compared with those of the previous completely normal control two months earlier. The only observed changes were a limited translation and corresponding side deviation of the right jaw in rest and during maximal opening. The maximal opening of the mouth was not altered. The orthopantomogram, which was normal at the previous visit, showed severe destructive abnormalities of both condylar heads, disclosing TMJ destruction within two months (figs 1 and 2). Splint treatment was started to decompress the TMJ.

Orthopantomogram: detailed photo of the left condylar grade 0, normal.

{kind=link}
{kind=link}
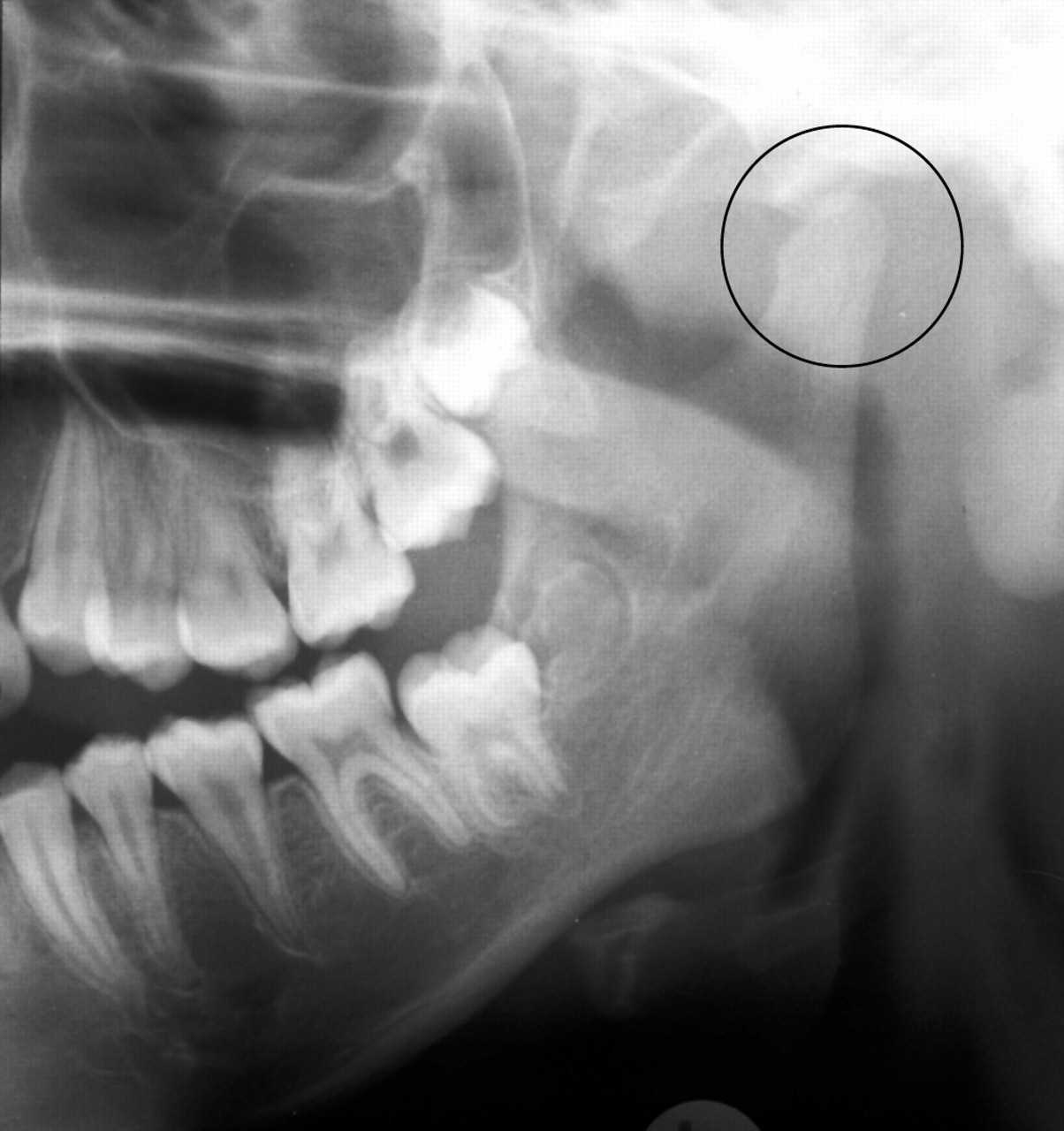
Orthopantomogram: detailed photo of the left condylar, grade 4, severe destructive abnormality, extensive erosions of the lateral and medial parts of the condyle and the temporal joint.
DISCUSSION
Sudden destruction of both condylar heads of the mandibula was seen in the patient only one month after she developed complaints. There is a striking discrepancy between the complaints and the clinical findings. The movements of the jaw compared with the previous measurements were exactly the same, except that the translation of the condylar head at the right side was limited but still present. This demonstrates that even discrete signs make thorough evaluation, including orthopantomography, necessary.
All studies on TMJ involvement agree that orthodontic evaluation is necessary and mandatory, but the frequency of orthodontic evaluation is not yet established.4,6,7,9,10 In our clinic all children with JIA have a routine orthodontic evaluation once a year. An extra evaluation can be arranged within a few days. Patients and parents should be informed of possible signs of TMJ involvement during the course of disease. The clinician has to be aware of the possibility of acute destruction of the condylar heads of the mandibula.
There is still no conclusive therapeutic regimen for TMJ involvement in JIA. Three possible therapeutic measurements have been reported: intra-articular corticosteroid injection, expanding antirheumatic drugs, or splint therapy. In our clinic splint therapy is the standard policy in condylar involvement in JIA.
The case illustrates the rapid and sudden destruction that can take place in a very limited period of time and emphasises the importance of awareness of clinical signals of TMJ destruction/involvement even when there are no objective abnormalities during evaluation. Treatment will be delayed if clinical signs are misinterpreted and the typical complaints are not attributed to possible involvement of the TMJ. Therefore regular evaluation of the TMJ by the paediatrician/rheumatologist and periodic evaluation by the orthodontist with orthopantomogram assessment is recommended.