Article Text

Abstract
Background Post-mortem (PM) microbiological investigations are recommended in cases of sudden unexpected death in infancy (SUDI), and infection is a recognised cause of such deaths, but no current evidence-based guidelines exist for the appropriate interpretation of results.
Aim To assess interpretive difficulties using a targeted cross-specialty questionnaire.
Methods 109 consultant specialists involved in infant death management were given a questionnaire providing information on five hypothetical standardised SUDI cases, which differed only in their PM microbiology findings. Participants classified each case into categories: definite bacterial infection, probable bacterial infection, bacterial growth of uncertain significance and PM contamination.
Results 63 (57%) specialists responded. There was no clinical scenario in which complete concordance in interpretation of PM microbiology results was established among participants. In cases with pure growth of Group 2 pathogens such as Group B β-haemolytic Streptococcus, 96% of respondents agreed upon probable or definite bacterial infection. With mixed growth of Group 2 pathogens, 83% reported probable or definite bacterial infection. Growth of organisms such as Staphylococcus aureus caused the most difficulty, with almost equal numbers of participants interpreting the finding as significant or non-significant. There were no consistent differences in interpretation between different specialist groups.
Conclusions While there is general agreement in interpretation of PM microbiology findings in some SUDI scenarios, no consensus was achieved for any clinical setting, and variation in the presumed significance between specialists was apparent. In the absence of appropriate evidence-based guidelines, this has practical implications for the management of such deaths in a multidisciplinary setting.
- Questionnaire
- infection
- blood cultures
- infant death
- autopsy
Statistics from Altmetric.com
Introduction
Sudden unexpected death in infancy (SUDI) represents the most common presentation of postneonatal death in the UK.1 Such cases are investigated by paediatric pathologists on behalf of HM Coroner, including complete post-mortem examination (autopsy) with performance of ancillary investigations, such as histological and microbiological (including bacteriological and virological) sampling, as recommended by the Royal College of Pathology and the Royal College of Paediatrics and Child Health.2 In a recent study of >1500 paediatric deaths, infection was the most common cause of ‘explained’ SUDI, and it has been hypothesised that infection, often subclinical or unrecognised, may also explain a proportion of ‘unexplained’ SUDI; in that study, the majority of infection-related deaths demonstrated histological evidence of an infectious process (such as meningitis or pneumonia).3 Further studies have reported that potentially pathogenic organisms are more commonly found in cases of unexplained SUDI than controls.4 5 These data suggest that there may be an underlying infection-related systemic process in a proportion of cases, despite the absence of histological evidence of infection.
However, while post-mortem microbiological sampling remains an important component of current investigation of SUDI deaths, appropriate interpretation of the significance of such post-mortem microbiology results remains a difficult but important and controversial topic, with no evidence-based published guidelines regarding what constitutes a ‘significant’ result. Interpretation is therefore usually based on clinical acumen derived from results in living patients, but there is a lack of published information on the interpretation of data derived from autopsy sampling. Confounding factors in this setting include differences in sampling sites and techniques, use of perimortem antibiotics during resuscitation, post-mortem translocation and sample contamination.6 7
A recent literature review examined published autopsy bacteriology findings from all ages and concluded that most blood and cerebrospinal fluid results (if taken carefully) should be negative, and that a substantial proportion of positive results would be a result of genuine infection.7 However, data from recent series of SUDI cases do not support this interpretation, since most SUDI samples are associated with some organism growth.4 The clinical importance of correct post-mortem microbiological result interpretation is further highlighted by medicolegal cases, which have passed to the court of appeal or resulted in acquittal, based on such findings alone.8
The aim of this study was to investigate opinions and assess interpretive differences and difficulties in interpretation of autopsy microbiology findings in SUDI using a cross-specialty questionnaire.
Methods
In total, 109 consultant specialists were contacted by email, including specialists routinely involved in infant death management, or specialists who come into contact with such cases as part of their service work, including paediatric pathologists, general histopathologists, microbiologists, and paediatricians (including paediatric infectious-disease specialists and specialists in child protection). Non-responders in the first round were recontacted after 2 weeks with a further request to participate.
Subjects were provided with a specialty specific questionnaire which contained information on five standardised SUDI cases, differing only in their post-mortem microbiology findings from blood, spleen and lung. The clinical history provided was that of a 2-month-old child found dead at home in bed, who had been previously well with an unremarkable antenatal and neonatal period. A full post-mortem examination was performed which was essentially unremarkable and did not reveal a cause of death. The weight, head circumference and length were on the 50th centile for age. Appropriate post-mortem samples had been taken for histology, virology, toxicology and metabolic screening. Blood, spleen and lung biopsies were taken for microbiology. Histological analysis was unremarkable. Toxicology and metabolic screening were negative. Virology results were negative.
Five microbiology scenarios were provided, and participants were asked to classify each case regarding the likely cause of death into one of four categories, including; definite bacterial infection, probable bacterial infection, bacterial growth of uncertain significance and post-mortem contamination. Findings were chosen to ideally represent the spectrum of infective and non-infective cases, as well as those cases which clinically appear more difficult to interpret (table 1).
Microbiology results from the clinical scenarios provided to respondents, listed by case
Results
The 109 specialists included 47 paediatric pathologists, 14 histopathologists, 11 microbiologists, nine infectious-disease specialists and 28 general paediatricians (figure 1A). Sixty-three (57%) responded (figure 1B), of which 50 fully completed the questionnaire; the remaining 13 responded but declined to answer the questions fully, as they felt the interpretation of such results was outside their area of expertise. All responses were recorded anonymously, being identified only by clinical specialty and study number. Five specialists offered more than one interpretation for some cases and these responses were therefore excluded.

Proportion of specialists (%) invited to participate by discipline (A) and with individual discipline response rate (B).
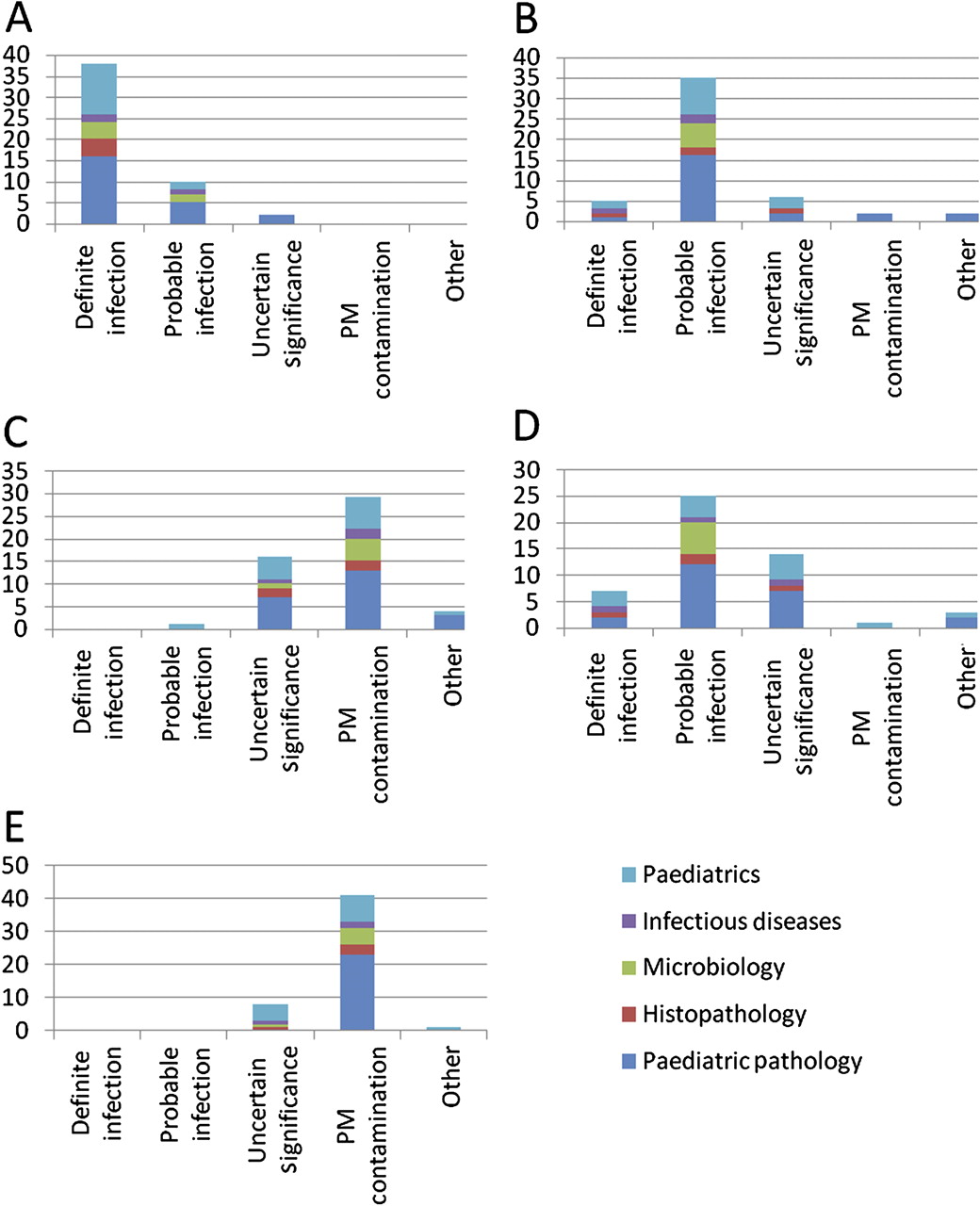
Concordance rates varied by case, but even among this small group of highly selected specialists in whom management of infant death is part of their routine practice, there were no cases in which complete agreement was reached regarding either actual interpretation or clinical significance regarding the likely cause of death. In case 1 (all sites having pure growth of group B β-haemolytic Streptococcus); all specialists used the provided answers. Seventy-six per cent agreed on definite bacterial infection, and 20% responded as probable bacterial infection. Two (paediatric pathologists) would not have regarded these findings as suggestive of an infective death, selecting bacterial growth of uncertain significance (figure 2A).

Distribution of answers by discipline and by answer. (A) (Case 1): pure growth of group B β-haemolytic Streptococcus. (B) (Case 2): mixed growth of group (B) β-haemolytic Streptococcus. (C) (Case 3): negative blood cultures with coagulase negative staphylococcus. (D) (Case 4): Pure growth of S aureus in blood cultures. (E) (Case 5): mixed growth. PM, post-mortem.
In case 2, microbiology results demonstrated mixed growth of organisms, including growth of group B β-haemolytic Streptococcus from all sites. Seventy-three per cent agreed on probable bacterial infection, 10% responded with definite bacterial infection, but one in six specialists would not have regarded the findings as sufficient evidence of an infective cause of death. In total, of the 50 specialists, paediatric pathologists expressed the widest range of answers (figure 2B).
Case 3 showed negative blood cultures and coagulase-negative staphylococcus only from other sites. The majority (58%) responded as post-mortem overgrowth/contamination or bacterial growth of uncertain significance (32%). There was no answer of definite bacterial infection in this setting, but one respondent suggested probable bacterial infection (figure 2C).
Case 4 was designed to be the most difficult to interpret, and this proved correct. There was pure growth of Staphylococcus aureus in blood cultures and mixed growth including S aureus from other sites. More than half of respondents (64%) suggested probable or definite bacterial infection as the cause of death, while the remainder would not have given infection as the likely cause of death. Interestingly, all microbiologists responded as probable bacterial infection in this case compared with only 60% of paediatric pathologists (figure 2D).
Finally, case 5 showed mixed, predominantly non-pathogenic organisms. Eighty-four per cent agreed on post-mortem contamination, including all paediatric pathologists. There were no answers of definite or probable bacterial infection (figure 2E).
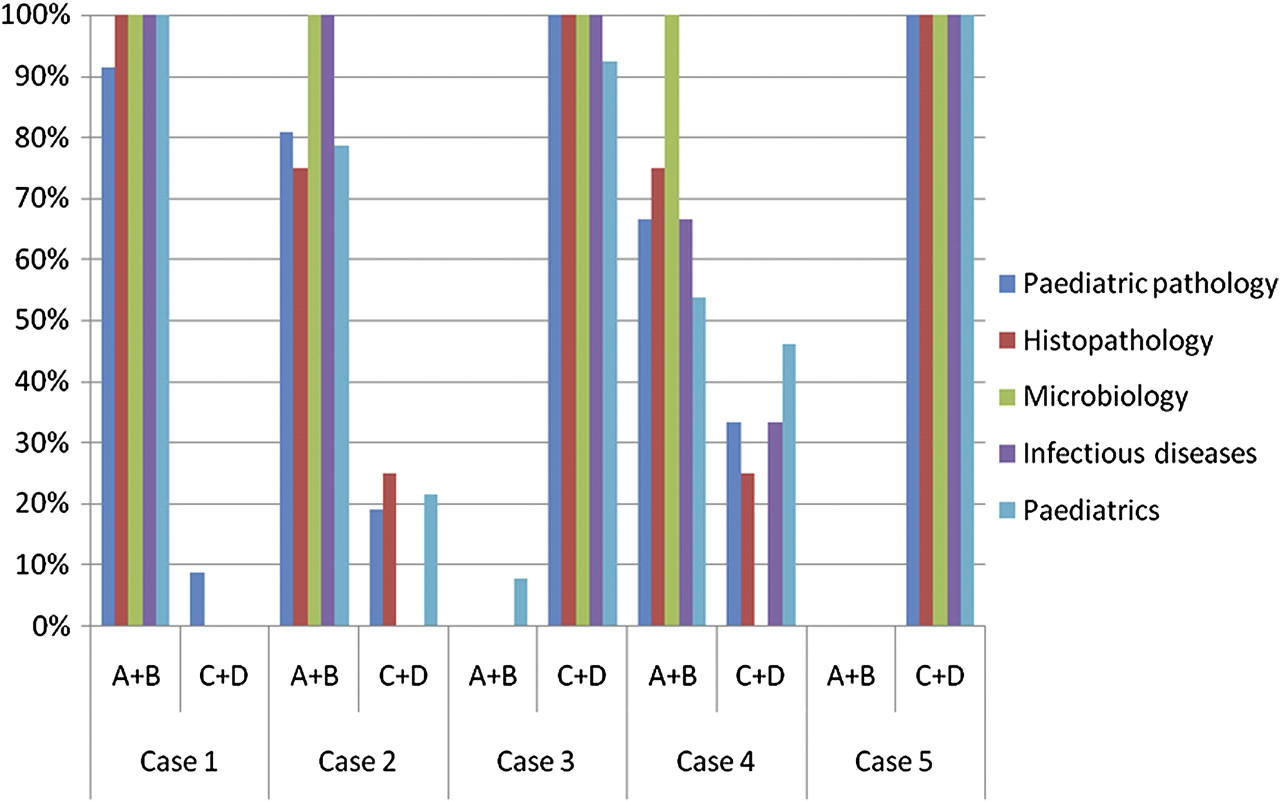
On review of answers by specialities, there was no general consensus within specialities. Overall, paediatric pathologists provided the widest range of opinions across the cases compared with other specialities. If the responses are categorised by clinical significance, summarising as either ‘at least probable bacterial infection’ or ‘uncertain significance or post-mortem contamination,’ microbiologists appeared most consistent in their evaluation, with paediatric pathologists offering the least concordance, only fully agreeing in one case (figure 3). It should be emphasised, however, that no ‘correct’ answer is possible for any of the cases, since no independent gold standard investigation is currently available to indicate unequivocally the significance of such post-mortem microbiological findings, the responses representing opinions, which may or may not be ‘correct.’
{kind=link}
{kind=link}
{kind=link}
Answers of definite/probable infection (A&B) verse infection of uncertain significance/post-mortem contamination (B&D) by specialty (%).
Discussion
The findings of this study have demonstrated that, even among those involved in infant death investigation, there is no overall consensus regarding the appropriate interpretation of post-mortem microbiological results in terms of their likely significance regarding the cause of death. While ‘general’ agreement was demonstrated in some scenarios, such as those highly likely or highly unlikely to represent an infection-related death, in other scenarios, such as the presence of S aureus in post-mortem cultures, there was essentially no agreement regarding its significance. In particular, there was no consensus opinion among paediatric pathologists, who are the specialists most likely to be involved in obtaining and interpreting the results of such microbiological investigations.
There is no current evidence that provides ‘gold-standard’ guidance for the correct interpretation of post-mortem microbiology results. There have been several studies reporting on post-mortem microbiology results.9–11 In most of these, S aureus was identified, but the significance thereof remains unclear. One early study investigated the concept of post-mortem ‘transmigration,’ using injection of ‘tracer organisms’ into bodies following death prior to autopsy,12 but the conclusion was that further investigations were required to answer the question of significance of organisms identified at autopsy. None of these reviews are specific to infant deaths.
S.aureus has been identified in several studies examining infant deaths and, in particular, SUDI.4 13 This includes the identification of enterotoxigenic bacteria in Sudden Infant Death Syndrome (SIDS) and healthy infant controls; 11% of cases had S aureus identified in blood cultures at post-mortem examination compared with no blood cultures of healthy infants, but putative post-mortem translocation remains a major confounding factor. There has been much speculation over the significance of the presence of S aureus in the nasopharynx of infants.14 15 S aureus was identified in the nasopharynx of 39% of healthy infants during the first 3 months of life,16 and S aureus was the predominant isolate in nasopharyngeal swabs in both healthy infants and SIDS cases.15 A recent large study examining the prevalence of organisms from SUDI post-mortem cultures has further highlighted the increased frequency of S aureus in ‘unexplained’ infant deaths compared with those dying of known non-infectious causes.4
The main issue in clinical practice therefore remains the appropriate interpretation of autopsy microbiology results. The significance of such results is usually based on the assessment of culture findings with regards to sample site, the organism's pathogenic potential, the child's age and the site's usual bacterial flora, together with usage of significance criteria based on infection in living children. Organisms with a high pathogenic capacity (eg, group B β-haemolytic Streptococcus) and/or obtained from sites that would usually be considered sterile, such as cerebrospinal fluid results, are presumed to be of more significance.17 Isolates from post-mortem blood cultures which might be considered pathogenic in a living patient may be considered to represent possible post-mortem translocation, or may be considered potentially pathogenic if found in multiple sites with the same antibiotic sensitivity pattern.18 In cases of SUDI, there are obviously limited clinical details regarding objective findings such as preceding temperature, respiratory rate or heart rate, or ante-mortem full-blood-count differentials; which would be standard investigations as part of a clinical investigation of possible sepsis. In the post-mortem setting, the detection of a pathogenic organism does not necessarily indicate clinical significance with regard to the cause of death.7 17 18
In one study of SUDI deaths during an 8-year period,19 10 were diagnosed as infective based solely on the microbiological findings, (with associated negative or minimal macroscopic/histological findings), but the rationale for selecting these organisms was not stated; isolates, however, included those previously referred to as group 2 pathogens,4 such as Streptococcus pneumoniae, Neisseria meningitides, group B β-haemolytic Streptococcus and Haemophilus influenza.
As mentioned, numerous hypotheses have been suggested regarding the cause of SIDS/SUDI, in particular, it is suggested that a proportion may be related to infection.7 20–22 More potentially pathogenic organisms (including S. aureus and Escherichia coli), are isolated from infants whose death is sudden and unexpected compared with non-infective deaths.4 5 In a previous study of post-mortem investigations in 546 SUDI performed at a single centre, the cause of death was explained in 17% based on histological investigations, and in 7% primarily based on post-mortem microbiological findings.3 In particular, where a cause of death was identified, the majority of infection-related diagnoses demonstrated histological abnormalities, with or without positive specific microbiological investigations.
Current guidelines advise that the investigation of SUDI deaths should include discussion of post-mortem findings by the SUDI paediatrician and the pathologist.2 Subsequently, a discussion meeting may be held, chaired by a paediatrician with a special interest in SUDI. However, little published evidence is available regarding the effectiveness of a multidisciplinary approach to interpretation of the significance of post-mortem findings, and as demonstrated by the findings of this study, there is little agreement between specialists regarding the significance of microbiological findings.
In summary, the interpretation of microbiological findings in SUDI deaths at present remains challenging. These findings emphasise that the interpretation of such microbiology results varies among specialists and is based on opinion rather than objective criteria. The data support previous suggestions that further research into the development of novel diagnostic methods is required and that alternative diagnostic markers of significant infections need to be found to aid the interpretation of post-mortem microbiology.
Take-home messages
There is a paucity of information to assist in the interpretation of post-mortem microbiology results. There is no consensus among specialists in interpreting such results, and multidisciplinary team meetings are advised to discuss such findings in cases of SUDI. A ‘gold-standard’ objective test is required to determine the clinical significance of post-mortem microbiological findings in SUDI.
Acknowledgments
Thanks must go to the respondents who took time to complete the questionnaire and provide their thoughts on the different scenarios.
References
Footnotes
Funding JWP is funded by a grant awarded by SPARKS charity. SPARKS had no involvement in the collection, analysis or interpretation of data, in the writing of this paper, or in the decision to submit the paper for publication.
Competing interests None.
Provenence and peer review Not commissioned; externally peer reviewed.