Article Text

Abstract
Aims Sudden unexpected death in infancy (SUDI) investigation requires extensive ancillary investigations, the results of which, such as postmortem microbiology, can be difficult to interpret. Markers of an inflammatory response, including interleukin 6 (IL-6), c-reactive protein (CRP) and cellular adhesion molecules are elevated in infections, yet little attention has been paid to their assessment after death. This study investigates the role of inflammatory markers in SUDI autopsies for determining cause of death.
Methods Cases of SUDI over a 14 year period were identified from an autopsy database and 100 cases were selected for immunohistochemical staining of heart and liver for IL-6, CRP, P-selectin, VCAM-1 and ICAM-1 (CD54), with staining patterns compared between five groups, including infectious and unexplained SUDI.
Results There were significant differences between groups. Cases of histological infection demonstrated strongly positive hepatocyte CRP and ICAM-1 expression and increased myocardial staining for CRP. Half of trauma-related deaths demonstrated diffuse hepatic CRP expression but without myocardial CRP staining. Staining of unexplained SUDI cases were predominantly negative, apart from a subgroup in whom Escherichia Coli was identified, who had increased expression of hepatic IL-6.
Conclusions There were distinct patterns of organ-specific CRP and ICAM-1 expression in SUDI by cause of death. These markers of inflammation were rarely present in unexplained SUDI suggesting either a non-inflammatory cause of death or a failure to mount an effective acute phase response. Immunohistochemical staining offers potential to identify infection-related deaths and provides insight into SUDI mechanisms.
- SIDS
- ACUTE PHASE PROTEINS
- AUTOPSY PATHOLOGY
- IMMUNOHISTOCHEMISTRY
Statistics from Altmetric.com
Introduction
In cases of sudden infant death (sudden unexpected death in infancy (SUDI)), a medical cause of death is identified in around a third.1 Evidence suggests that clinically unrecognised infections may be associated with unexplained deaths, including a history of minor self-limiting illness/coryza in the preceding days2 and increased frequency of detection of potentially pathogenic bacteria from postmortem cultures.3
Investigation of SUDI requires autopsy examination,4 including microbiology, but interpretation of such findings is difficult in the absence of additional features.5 ,6 SUDI may be associated with a systemic inflammatory response, which in turn may represent a final common pathway to death, as suggested by the triple risk hypothesis,7–9 in which a predisposed infant is exposed to an exogenous stressor during a critical developmental period.
Innate immunity is rapid and non-specific with a wide repertoire against numerous organisms; the response includes cytokine and acute-phase protein production and upregulation of cellular adhesion molecules. Interleukin 6 (IL-6), is a multifunctional cytokine that stimulates immune and inflammatory responses as a consequence of macrophage exposure to pathogens. Increased macrophage numbers are reported in unexplained SUDI10 and raised cerebrospinal fluid IL-6 levels in infectious causes of infant death.11 Similarly, c-reactive protein (CRP) is a hepatic acute phase protein, elevated in acute inflammation with a role in host defence.12 ,13 Elevated levels are detectable within 4–6 h following the initial insult, due to gene transcription response to cytokines, including IL-1, IL6 and tumour necrosis factor.14 Levels peak within 24–48 h. Expression of cellular adhesion molecules by endothelial cells facilitate rolling, attachment and extravasation of neutrophils,15 and is associated with many infections in clinical practice.16
There are little data regarding blood CRP after death.17 An alternative approach is to assess liver CRP, which is routinely sampled in all SUDI autopsies. An adult study reported that diffuse CRP immunostaining was more frequently found in non-acute deaths or in those associated with extensive tissue injuries but neither infectious aetiologies nor SUDI were included.18
We suggest that activation of the host inflammatory cascade through pathogen exposure is associated with expression of inflammatory markers at their site of production, or circulating in myocardium. This study investigates the significance of such markers of infection in sudden infant death.
Methods
SUDIs were identified from an anonymised paediatric autopsy database (all performed at a single specialised centre over a 14 -year period). Infants 7–365 days who died suddenly and unexpectedly without a pre-existing medical cause were selected and categorised into the following groups:
-
Unexplained with inconclusive microbiology (mSUDI): Infants whose death despite a complete autopsy examination including ancillary investigations remained unexplained, however postmortem microbiological findings detected either Staphylococcus aureus (in lung and spleen only) or Escherichia coli (in at least one of site of blood, lung and/or spleen).
-
Unexplained (uSUDI): Infants whose death despite a complete autopsy examination including ancillary investigations remained unexplained (including sterile postmortem microbiology and negative virology findings).
-
Non-infectious death (non-infectious): Infants whose sudden death was due to trauma who either died immediately or who did not receive intensive care for longer than 48 h prior to death and had no evidence of infection on either histology or microbiology results.
-
Microbiological infection (positive micro): Infants whose death remained unexplained following a complete autopsy including ancillary investigations with negative histological findings but with positive findings on postmortem microbiology which would indicate systemic sepsis if identified in life.
-
Histological infection (positive histo): Infants who demonstrated definite evidence of histological infection with positive microbiological findings, such as pneumonia and meningitis.
Twenty cases from each group were identified in which formalin-fixed paraffin-embedded heart and liver tissues were available and where consent for research was either available or exempt (existing holdings). Tissue microarrays of 4 mm were created and sections stained using; IL-6 (1:100, Novacastra, UK), intercellular adhesion molecule-1 (ICAM-1) (CD54, 1:25, Novacastra, UK), vascular cell adhesion molecule-1 (VCAM-1) (1:1, ABCam, UK), P-selectin (1:100, Novacastra, UK) and CRP (1:100, ABCam, UK). Immunohistochemical staining was performed using the Bond-Max system (Leica Microsystems) under identical conditions. Slides were scanned using a Hamamatsu NanoZoomer 2.0-HT slide scanner (Hamamatsu Photonics UK, Hertfordshire, UK) and analysed (non-blinded) using NanoZoomer Image Analysis Software for quantifiable differences.
Interleukin 6 staining was performed only on liver. The remaining antibodies were performed on heart and liver and a grading system used for scoring (table 1, figures 1 and 2).
Grading system for immunohistochemical staining
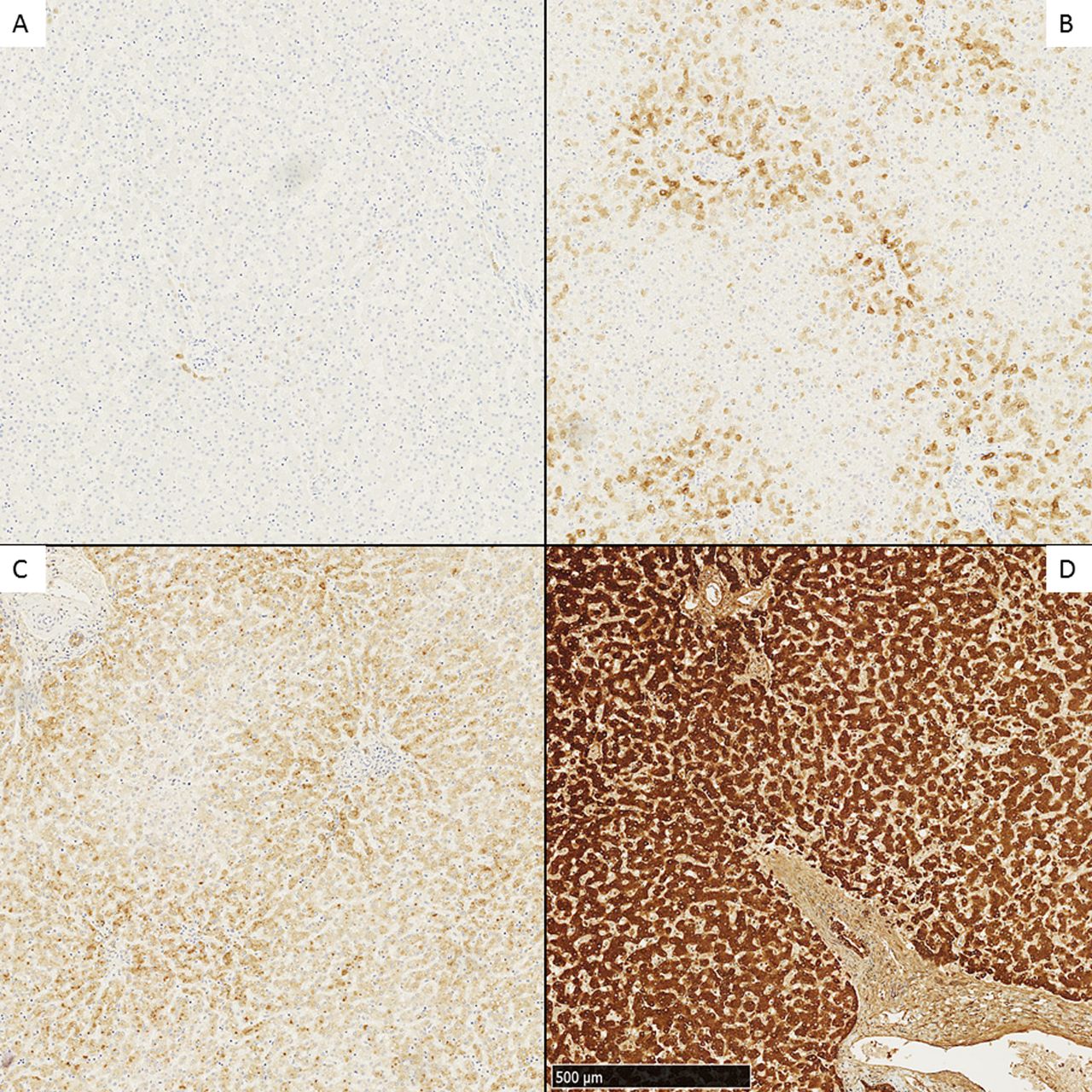
Examples of grading for c-reactive protein staining of hepatocytes, identifying four distinct patterns, including no staining (A), Periportal with negative intervening hepatocytes (B), Strong periportal with intervening staining (C) and strong diffuse (D).

Immunohistochemical c-reactive protein staining patterns of myocytes, identifying different patterns including strong perivascular/zonal staining (A) and strong diffuse staining (B).
Results were compared between groups using Mann-Whitney U test and Kruskal-Wallis statistical test with SPSS V.21.0 (IBM). The Clopper-Pearson method was used to calculate 95% CIs. The study was approved by the local research ethics committee (London Bloomsbury REC).
Results
Hundred patients were selected, including 20 from each group, age range 9–345 days, 41 girls and 59 boys. The postmortem interval was median 2 (range 0–8) days. There were no statistically significant differences regarding age, gender or postmortem interval (p=0.118; p=0.508; p=0.623, respectively).
CRP expression
Statistically significant differences were identified between groups for CRP expression in liver (p<0.0001) and heart (p<0.0001 (figures 3 and 4). All cases of histologically proven infection demonstrated strongly positive hepatocyte CRP expression, with either low or absent expression in SUDI groups (p<0.0001 for mSUDI and uSUDI), microbiological infection groups (p<0.0001) and non-infective groups (p=0.029).
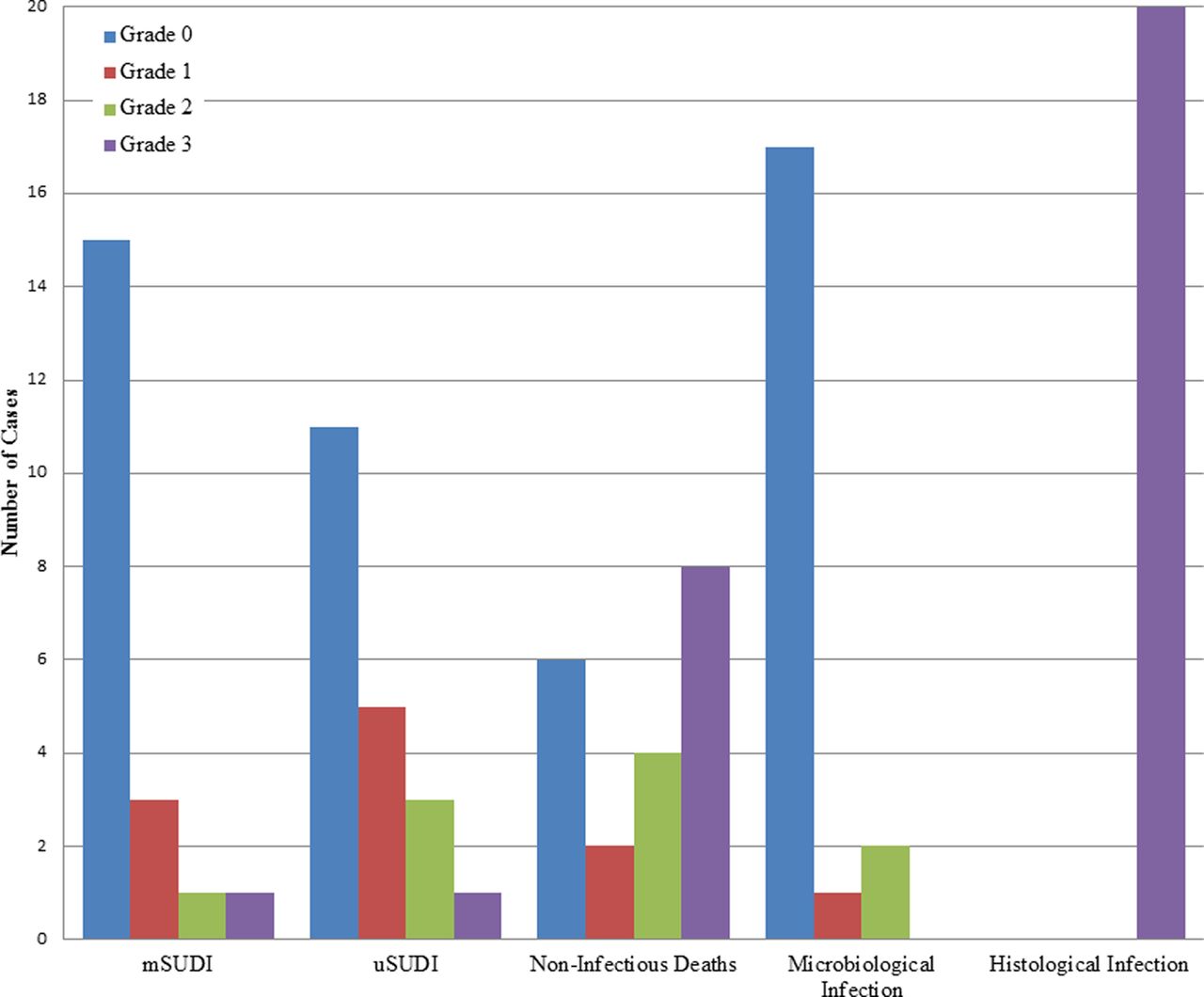
Bar chart demonstrating the variation of hepatocyte staining between cohorts, with cases of histologically confirmed infection showing consistent diffuse positivity for c-reactive protein .mSUDI; unexplained with inconclusive microbiology sudden unexpected death in infancy, uSUDI, unexplained sudden unexpected death in infancy.
Bar chart demonstrating the variation of myocytes staining between cohorts, with cases of histologically confirmed infection showing positivity for c-reactive protein in comparison with other groups. mSUDI; unexplained with inconclusive microbiology sudden unexpected death in infancy, uSUDI, unexplained sudden unexpected death in infancy.
The non-infective group showed variable hepatic CRP expression particularly when initially successfully resuscitated following trauma (table 2). The six CRP-negative cases were all sudden deaths, due to fire (two), head injuries (two), fall (one) and traumatic liver rupture (one).
Cases of non-infectious deaths with corresponding variable immunohistochemical results highlighting the cases of positive CRP staining of the liver and heart
Six cases showed grade 1 or grade 2 staining, with histories of trauma but who were resuscitated and died within 48 h. The remaining eight demonstrating grade 3 hepatic CRP staining included two falls with associated injuries, three head trauma and one asphyxia. The remaining two cases had findings of head injuries at autopsy with unclear histories and demonstrated diffuse staining.
Of the microbiological infection group, 17 had negative liver CRP staining, including β-haemolytic Group B streptococcal sepsis (GBS) and Streptococcus pneumoniae sepsis. Three had periportal positive staining, including one with a grade 1 pattern (GBS cultured in blood and lung) and the other two with grade 2 (one case of GBS; cultured in blood, spleen and lung, and one S. aureus with toxic shock syndrome toxin-1 identified).
Of the 20 unexplained uSUDIs, one had grade 3 staining (with prominent macrosteatosis), three demonstrated patchy grade 2 staining, five showed grade 1 periportal staining and remaining 11 were negative. Of the 20 unexplained mSUDIs, 15 were negative, 4 had low grade staining (3 grade 1, 1 grade 2) and 1 had grade 3 staining.
There was significantly increased cardiomyocyte CRP staining in the histologically proven infectious deaths compared with all other groups (p<0.0001). Eighteen of 20 (90%) cases in this group with positive hepatic CRP expression also demonstrated myocyte positivity, compared with five non-infectious cases with positive myocyte CRP staining, all of whom had head trauma and positive hepatocyte CRP staining. There were no cases with positive myocyte staining but negative hepatocyte staining in any group. Only one case in the mSUDI group had CRP staining of the myocardium.
Adhesion molecules
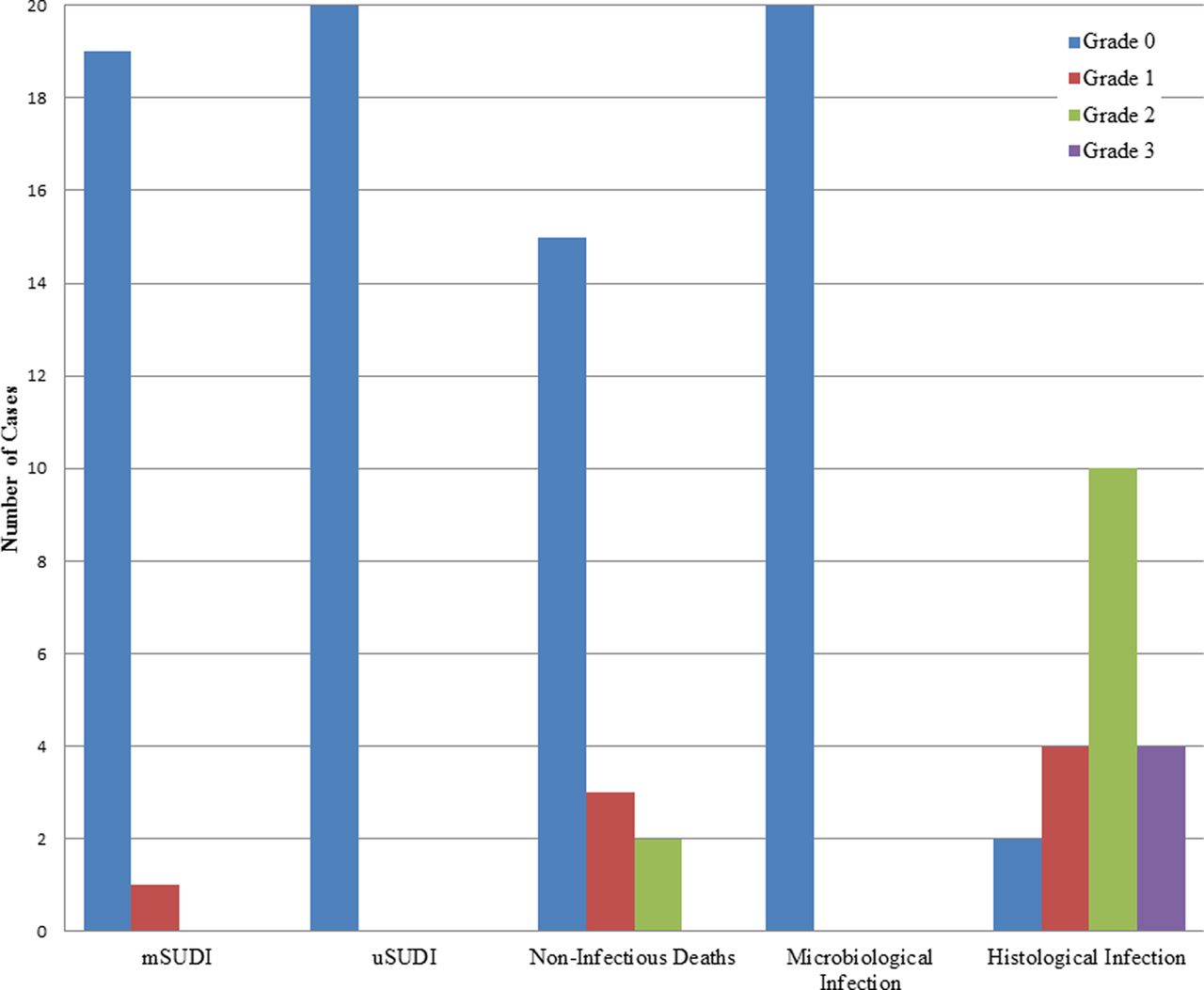
There were no statistically significant differences in P-selectin staining between groups, being diffusely positive for heart (p=0.593) and negative for liver (p=0.355). Immunohistochemical staining for ICAM-1 was positive in liver sinusoids and cardiac endothelium, with significantly increased expression in the histological infection group (heart, p<0.0001, liver, p<0.0001, respectively), compared with all other groups (figures 5 and 6). VCAM-1 staining in all cases was diffusely positive in the heart and liver making interpretation impossible.

Bar chart demonstrating the variation of ICAM-1 staining of hepatocytes between cohorts, with cases of histologically confirmed infection showing statistically significant positivity compared with other groups. mSUDI; unexplained with inconclusive microbiology sudden unexpected death in infancy, uSUDI, unexplained sudden unexpected death in infancy.

Bar chart demonstrating the variation of ICAM-1 staining of cardiomyocytes between cohorts, with cases of histologically confirmed infection showing statistically significant positivity compared with other groups. mSUDI; unexplained with inconclusive microbiology sudden unexpected death in infancy, uSUDI, unexplained sudden unexpected death in infancy.
Interleukin 6
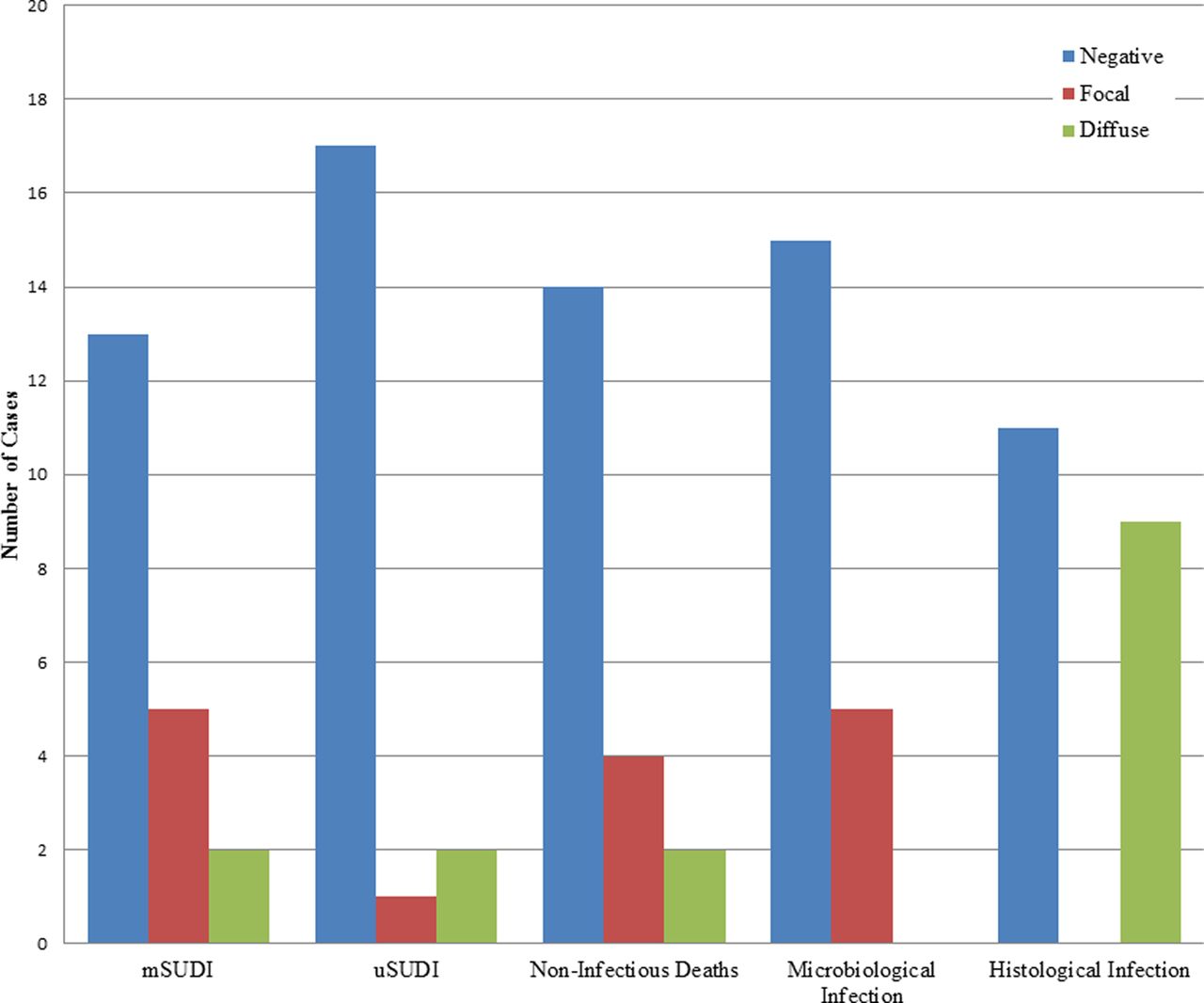
There were no statistically significant differences in IL-6 expression between groups (p=0.138), however nine (45%) of the histological infection group showed diffuse IL-6 staining (figure 7). Within the mSUDI group, cases with microbiological evidence of E. coli had significantly increased IL-6 hepatocyte staining compared with those with S. aureus (p=0.035) or sterile microbiology (p=0.037).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bar chart demonstrating the distribution of cases within cohorts with interleukin 6 staining. mSUDI; unexplained with inconclusive microbiology sudden unexpected death in infancy, uSUDI, unexplained sudden unexpected death in infancy.
Sensitivity and specificity for identification of infection
All 20 with histological infection had positive staining for either IL6, CRP or ICAM-1. Twenty seven cases had triple negative staining; including nine (45%) mSUDI, seven (35%) uSUDI, four (20%) non-infectious and seven (35%) microbiological infections. Thirteen cases were positive for IL-6 but negative for CRP; five mSUDI, two uSUDI, two non-infectious (both burns) and four microbiological infection group (two group B haemolytic Streptococcus and two S. pneumoniae).
Comparing histologically proven infection versus all other deaths, diffuse hepatic CRP staining sensitivity was 100%, specificity 87.5% (table 3).
Grouping of antibodies into positive and negative staining with separation of categories as shown
In reality, since a history of trauma would be available, the specificity in clinical practice would be even higher (table 4). Cardiac CRP staining provides further supporting evidence but since all cases also demonstrated diffuse liver expression, the sensitivity is not increased.
Grouping of antibodies into positive and negative staining with separation of categories as shown, excluding cases of non-infectious deaths
Discussion
This study demonstrates statistically significant differences in immunoexpression patterns of inflammatory markers by cause of death in SUDI. Using current protocols, most SUDI deaths remain unexplained post autopsy, and interpretation of ancillary investigations such as postmortem microbiology is difficult in individual cases.5 While extensive immunostaining and molecular techniques are routinely used in other settings such as paediatric tumours,19 ,20 histological investigation in SUDI remains limited. There is therefore a need to develop novel approaches, which may provide additional information, in order to progress understanding of these paediatric deaths.
Immunohistochemical staining for inflammatory markers is possible on routinely obtained formalin-fixed paraffin-embedded autopsy tissue and there are differential patterns of expression between infective and non-infective deaths. Specifically, histologically proven infections show diffuse hepatocyte CRP staining, traumatic deaths show variable expression consistent with a systemic inflammatory response, but less marked than infection and with reduced myocyte CRP staining.18 ,21 The unexplained deaths with postmortem microbiological findings consistent with sepsis if identified in life show predominantly negative liver CRP expression, suggesting that either death is rapid, without time for CRP response (<4 h) or that death occurs through a non-systemic-inflammatory mechanism, that such deaths affect patients who genetically cannot mount a normal CRP response,22 or that these are non-infective deaths with incidental microbiological findings.
IL-1, IL-6 and TNF stimulate CRP production23 and are under genetic control, with polymorphisms influencing protein levels or function.24 ,25 The inability to mount an effective acute response through such polymorphisms has been suggested as a possible predisposing factor for some SUDIs.26 In this study we did not examine cytokine polymorphisms and further work is required to explore this hypothesis.
Half of those with hepatocyte CRP expression also demonstrated myocyte CRP staining, all of whom were associated with strong diffuse hepatocyte staining. Furthermore, of those with diffuse hepatocyte staining and histological infection, 80% showed myocyte staining. The mechanism of myocyte immunostaining in these cases is unclear but is likely to represent binding of circulating CRP, possibly associated with tissue damage following ischaemia prior to death.27 ,28 The majority of unexplained SUDI (regardless of microbiological findings), showed no significant hepatic or cardiac CRP staining, suggesting that systemic inflammation or significant infection was not contributory to death.
SUDI typically occurs at night, with an uncertain time of death, and consequent delay in obtaining samples for chemical pathology, such as CRP from serum. Serum CRP correlates with liver CRP, as assessed by homogenisation of liver tissue,29 but data on postmortem CRP are limited. A study on CRP and prealbumin30 found only four SUDIs with a minimal increase in CRP, while seven patients had significant infection (four of which had prominent CRP elevation). There are little available data on immunoexpression of CRP within liver or heart. One study described similar patterns of CRP distribution (diffuse, periportal, focal and negative)18 in 314 autopsy cases (0–92 years of age). Histological findings were related to serum CRP levels at autopsy but the focus was on injury groups, with no discussion of infective patterns; diffuse staining was more frequently found in non-acute deaths. Hepatocyte CRP expression has also been described in viral hepatitis31 with an association between hepatocellular damage and CRP staining.
In summary, these data indicate that immunostaining can be reliably performed on routinely obtained SUDI tissue samples and that increased expression of IL-6, CRP and ICAM-1 are associated with infection-related death. Immunostaining for hepatocyte and myocyte CRP expression as an ancillary investigation in SUDI autopsies may allow accurate identification and timing of infection/inflammation associated deaths and may provide additional information in possible trauma-related deaths.
Take home messages
-
Immunohistochemical markers of infectious death can be reliably identified at autopsy in sudden unexpected death in infancy (SUDI).
-
C-reactive protein and intercellular adhesion molecule-1 (ICAM-1) (CD54) expression is markedly increased in infectious SUDI deaths.
-
Hepatic c-reactive protein expression may also be increased in association with the inflammatory response to severe head injury but shows a different pattern to infectious death.
-
The majority of non-infectious SUDI deaths are not associated with inflammatory marker upregulation regardless of postmortem microbiological findings.
Acknowledgments
The authors thank Malika Benatti for her assistance with performing the immunohistochemistry.
References
Footnotes
-
Contributors NJK and NJS conceived of and coordinated the study. JWP, NJK and NJS participated in its design. JWP, ARB, MTA, NJK and NJS participated in acquisition/interpretation of data. JWP performed the statistical analysis. All authors helped to draft the manuscript. All authors read and approved the final manuscript.
-
Funding JWP is part supported by the NIHR GOSH BRC and SPARKS charity. ARB is supported by a grant from the Lullaby Trust. NJS is part supported by GOSHCC and the NIHR GOSH BRC. This article presents independent research funded by SPARKS charity.
-
Competing interests None.
-
Ethics approval London (Bloomsbury) National Research Ethics Service Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.