Article Text

Abstract
Objective: To investigate the frequency of neonatal and later childhood morbidity in children exposed to antiepileptic drugs in utero.
Design: Retrospective population based study.
Setting: Population of the Grampian region of Scotland.
Participants: Mothers taking antiepileptic drugs in pregnancy between 1976 and 2000 were ascertained from hospital obstetric records and 149 (58% of those eligible) took part. They had 293 children whose health and neurodevelopment were assessed.
Main outcome measures: Frequencies of neonatal withdrawal, congenital malformations, childhood onset medical problems, developmental delay, and behaviour disorders.
Results: Neonatal withdrawal was seen in 20% of those exposed to antiepileptic drugs. Congenital malformations occurred in 14% of exposed pregnancies, compared with 5% of non-exposed sibs, and developmental delay in 24% of exposed children, compared with 11% of non-exposed sibs. After excluding cases with a family history of developmental delay, 19% of exposed children and 3% of non-exposed sibs had developmental delay, 31% of exposed children had either major malformations or developmental delay, 52% of exposed children had facial dysmorphism compared with 25% of those not exposed, 31% of exposed children had childhood medical problems (13% of non-exposed sibs), and 20% had behaviour disorders (5% of non-exposed).
Conclusion: Prenatal antiepileptic drug exposure in the setting of maternal epilepsy is associated with developmental delay and later childhood morbidity in addition to congenital malformation.
- epilepsy
- anticonvulsants
- malformation
- neurodevelopment
Statistics from Altmetric.com
A round 6.1 per 1000 pregnancies occur in women with epilepsy,1 making this the most common major neuro logical disorder in pregnancy requiring continuous treatment. Early reports suggested an increased prevalence of malformations in the offspring of epileptic mothers taking antiepileptic drugs (AEDs), such as phenytoin, carbamazepine, and sodium valproate.2,3 More recent prospective studies have shown that malformations occur in between 6 and 14% of exposed infants, compared with about 3% of children of epileptic mothers not taking drugs.4–7 Some malformations are more common following exposure to certain drugs. For example, spina bifida is associated with valproate or carbamazepine exposure,5,7,8 cleft lip and palate and microcephaly with phenytoin,3 hypoplastic nails with phenytoin and carbamazepine,9,10 and cardiac malformations can result from exposure to any of these AEDs.10–12 Other malformations requiring early intervention, such as inguinal hernias and joint dislocation, are not infrequently reported following valproate or carbamazepine exposure and, in later childhood, glue ear and myopia are prominent among those exposed to valproate in utero.13 There is also an increased frequency of minor anomalies, some of which may be associated with maternal epilepsy rather than its treatment.14 Specific combinations of major and minor anomalies, including characteristic facial findings, are often referred to as a fetal anticonvulsant syndrome. The facial features change with age. Some are associated with specific drugs while others, particularly in infancy, are common to all three major fetal anticonvulsant syndromes (the fetal valproate, carbamazepine, and phenytoin syndromes).13
The frequency of developmental delay following exposure to AEDs is controversial. In some studies, 20-30% of children exposed to carbamazepine or phenytoin had developmental delay or learning difficulties,10,15,16 while in others, usually,17 but not always,18 with shorter follow up periods, no increased risk was found. Specific cognitive dysfunction has been documented in otherwise normal offspring exposed to valproate, carbamazepine, phenytoin,18 and phenobarbitone.19 To assess the level of risk of adverse outcomes over a longer follow up period, we ascertained a cohort of mothers who took antiepileptic drugs in pregnancy and report the findings in their children.
METHODS
Aberdeen Maternity Hospital is the referral centre for all women with medical complications of pregnancy in the Grampian region of Scotland (population 525 300). We identified a cohort of women who took antiepileptic drugs in pregnancy and delivered at Aberdeen Maternity Hospital between 1976 and 1996 through review of hospital records. Mothers delivering since 1997 were also recruited from the antenatal clinic and postnatal wards. Those ascertained by records review were approached by letter, through their primary care physicians. A structured interview including pregnancy histories and a standardised assessment of all available offspring was carried out by a trained research nurse, using questionnaires and examination schedules validated in a previous study.13,20
Clinical features in the offspring were classified into six categories, according to an assessment protocol described previously.20 These were (1) congenital malformations, (2) developmental delay, (3) behaviour disorders, (4) neonatal withdrawal, (5) childhood medical problems, and (6) facies. Congenital malformations were divided into two subgroups, major if they required medical intervention (surgery or other therapy) in the first year of life, and minor if they did not (for example, cleft uvula, nail hypoplasia, digit hypoplasia, arachnodactyly, overlapping toes, sacrococcygeal sinus). Developmental delay was classified as speech delay when local developmental child health services had recorded a need for speech therapy, motor delay if the child was not sitting by 10 months or not walking by 18 months, and global delay if both speech and motor delay were evident. Children with apparently normal preschool developmental history, but special educational needs were classified as having a school age learning disorder. As delayed speech development cannot be reliably diagnosed before 21 months, the age by which most children have acquired single words, only children older than this are included in the calculation of developmental delay frequencies. Tables 1 and 2 include data for all children. Information about behaviour disorders such as autism, autistic spectrum disorder, Asperger syndrome, or attention deficit hyperactivity disorder was taken from hospital records of diagnoses made by a developmental paediatrician or child psychiatrist following clinical referral. Features such as jitteriness, hypotonia, hypoglycaemia, apnoeic episodes, and seizures in the neonatal period were considered possible manifestations of withdrawal. Information on later childhood medical problems such as myopia, strabismus, otitis media with effusion, and joint laxity, which were observed in our previous study of affected children,13 was specifically sought and recorded. Joint laxity was assessed using the Beighton score21 and was considered to be present if the score was 4/9 or greater. Clinical photographs taken by the research nurse were assessed for facial features of the fetal anticonvulsant syndromes by three of the authors independently (JD, SJM, PDT). Each author scored the features on a five point scale (“definitely present”, “probably present”, “uncertain”, “probably not”, “definitely not”). A characteristic face was considered to be present if at least two of the authors considered the features to be definitely or probably present.
Summary of outcomes of pregnancies
Adverse outcomes according to anti-epileptic drug exposure
The relationship between reported drug dosage and clinical outcome for children exposed to monotherapy was assessed using Student's t test (two tailed). Analysis of frequencies of features present at birth (neonatal withdrawal, malformations, and facial features) in relation to drug exposure was by χ2, or by Fisher's exact test (two tailed) if numbers were small. Because each drug exposure group had a different age structure, the Cox proportional hazards model was used for those characteristics whose diagnosis is age dependent (childhood medical problems, developmental delay, and behaviour disorders). In each analysis, comparison was made with frequencies in the non-exposed group, which was regarded as a control group. In order to include pregnancies terminated because of major malformation, the data for major congenital malformations include all pregnancies surviving into the second trimester, whereas frequencies for other features were based on livebirths only.
Families where exposed offspring had malformations, learning difficulties, or behaviour problems were offered medical assessment at the genetic clinic. Hospital and developmental records were reviewed with permission. This study was approved by the local research ethics committee.
RESULTS
Study population
Records were available for 411 mothers who delivered between 1976 and 2000 and who took an AED during pregnancy. Of these, eight had died before the study started and 102 had moved away. Contact was not appropriate in seven further cases because the child had been adopted or fostered and in one case because of neonatal death. The general practitioner refused permission to contact the mother in a further 35 cases, in one because of parental disability, and in one because of disability in the child. Of the remaining 258 mothers, 149 (58%) participated in this study.
Maternal and pregnancy histories
One hundred and forty-four mothers had epilepsy. The condition was idiopathic in 117 cases, but in 27 an underlying cause was identified. Twelve cases were attributed to head injury, four to brain tumours, three to perinatal factors, three to viral encephalitis, and five to miscellaneous individual causes. Three mothers took AEDs for bipolar affective disorder (two carbamazepine, one valproate), one was prescribed an AED for symptoms later diagnosed as migraine, and one was given phenobarbitone as a sedative.
Two hundred and sixty-one pregnancies were exposed to AEDs and continued beyond the first trimester. These resulted in 255 liveborn infants and six fetal losses. Three pregnancies were terminated because of congenital malformation (two neural tube defects and one exomphalos) and three pregnancies ended in fetal death associated with obstetric complications. Two hundred and ten pregnancies were exposed to monotherapy with one of seven drugs (table 2) and 51 were exposed to polytherapy. This was most commonly phenytoin and phenobarbitone (18 cases), but also carbamazepine and valproate (7), carbamazepine and phenytoin (6), carbamazepine and phenobarbitone (6), valproate and phenobarbitone (3), and various combinations, including the newer drugs, lamotrigine, gabapentin, vigabatrin, and topiramate (11). The mothers also had 38 liveborn infants while not taking AEDs. The mean maternal age at delivery was 27 years (17-43 years). At the time of study, the children ranged in age from 2 days to 39 years (mean 9 years) (some sibs of index cases were born before 1976). The outcomes are summarised in table 1.
Congenital malformations
Those exposed to polytherapy (table 2) had a significantly higher frequency of major malformations than the non-exposed group (p=0.012), although overall the frequency of malformations in the exposed children was not significantly different from the non-exposed (table 1). The most frequent major congenital malformation was inguinal hernia, most commonly occurring following exposure to carbamazepine either alone or in combination (table 3). Carbamazepine was also associated with hip dislocation, genital abnormality, congenital heart disease, and submucous cleft palate (a further case with cleft uvula was classified as a minor malformation). Valproate tended to be associated with talipes, other limb abnormalities, and genital abnormalities, such as hypospadias, hydrocele, and undescended testis. The pattern of abnormalities for other drugs is less clear, probably owing to the smaller number of cases in each group. Some children had more than one malformation. Minor malformations, such as fingernail hypoplasia, overlapping digits, clinodactyly, or plagiocephaly, were significantly more common in all the exposure groups.
Major malformations and drug exposure
Neurodevelopment
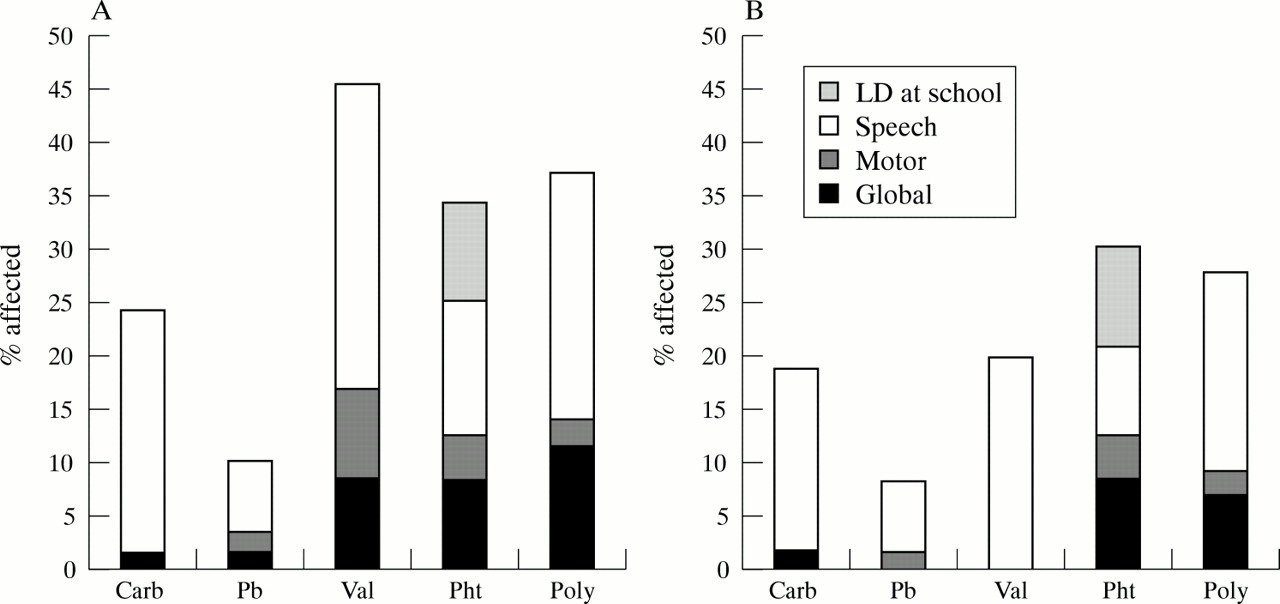
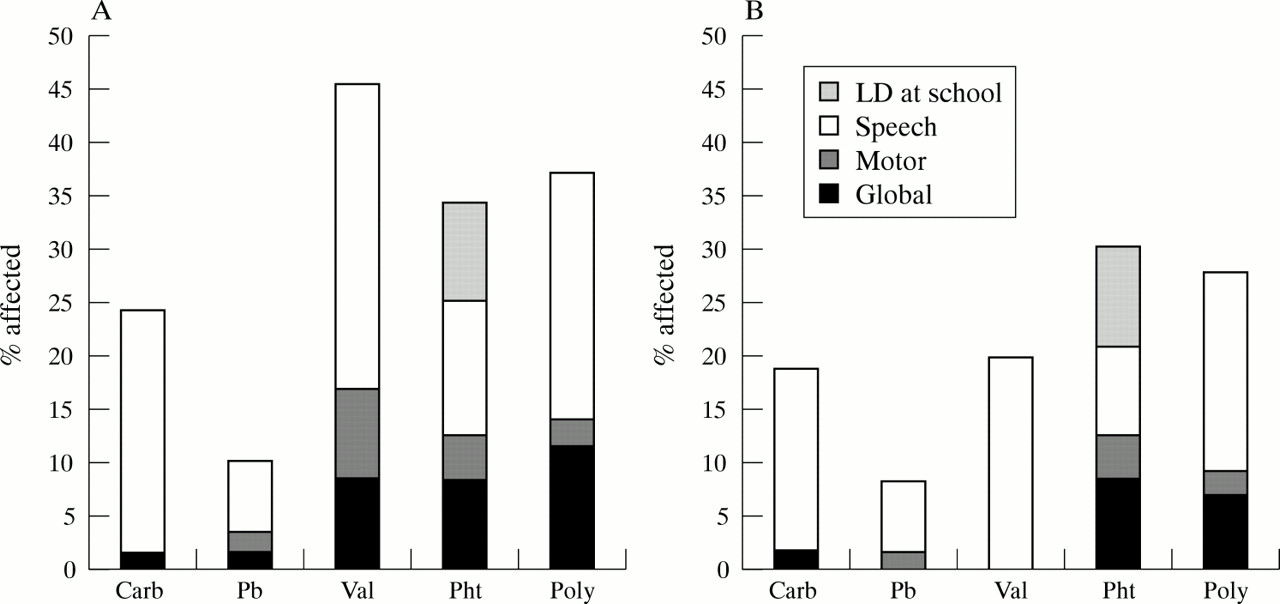
Developmental delay was significantly more common in those exposed to an AED than in children of epileptic mothers on no treatment (table 1). Analysis of the different drug exposure groups (table 2) showed that carbamazepine monotherapy (p<0.001), valproate monotherapy (p<0.001), phenytoin monotherapy (p<0.008), and polytherapy (p<0.001) were associated with significantly more developmental delay, whereas phenobarbitone monotherapy was not (p=0.55). Speech delay was common following exposure to valproate (29%) or carbamazepine (22%) monotherapy and to polytherapy (23%) (fig 1A). Most cases in the polytherapy group were exposed to combinations including either valproate or carbamazepine or both (8/11). Speech delay was much less common following phenobarbitone (6.7%) or phenytoin (12.5%) exposure. The frequency of motor delay alone was low in all exposure groups. The higher frequency of global delay in the polytherapy group results from children exposed to valproate or phenytoin in various combinations in 5/6 cases.
{kind=link}
Pattern of developmental delay. (A) Exposed group. (B) Exposed group after excluding cases with a family history of developmental delay. Carb = carbamazepine, Pb = phenobarbitone, Val = sodium valproate, Pht = phenytoin, LD = learning difficulties.
Family histories were reviewed to assess the influence of genetic factors on the occurrence of developmental delay. Thirteen families where an exposed child had developmental delay or learning difficulties reported a family history of developmental delay or learning difficulties. In four cases, a parent and sometimes other relatives were affected, suggesting a possible monogenic cause (karyotypes and fragile X mutation testing were normal). In nine families, more distant relatives were affected, suggesting a multifactorial aetiology. When the affected children with a family history of developmental delay were excluded, valproate was associated only with speech delay (fig 1B). The frequency of developmental delay in those exposed to phenobarbitone alone remained not significantly different from those exposed to no AEDs, while the frequencies for those exposed to carbamazepine (p=0.003), valproate (p<0.001), phenytoin (p=0.006), and polytherapy (p=0.005) were still significantly higher.
Behaviour
Autism and related disorders were observed in 11 cases. Two had a formal diagnosis of autism (one exposed to valproate and phenobarbitone and one to carbamazepine) and nine were said to fall in the autistic spectrum (three exposed to valproate alone, three to carbamazepine alone, two to valproate and carbamazepine, and one to carbamazepine, phenytoin, and lamotrigine). Five children with normal preschool developmental milestones had behaviour problems requiring medical or clinical psychology intervention or special schooling. Two of these were diagnosed as in the autistic spectrum while three had attention deficit hyperactivity disorder. Overall, behaviour disorders were not significantly more common in the exposed children (table 1), but analysis of specific drug exposure groups shows significantly more behaviour problems in the carbamazepine monotherapy (p<0.001), valproate monotherapy (p<0.001), and polytherapy groups (p=0.006).
Neonatal withdrawal
Clinical features compatible with neonatal withdrawal were more common in the exposed children than in the non-exposed (table 1). One case in the non-exposed group was scored positive because of neonatal hypoglycaemia associated with low birth weight. Phenobarbitone monotherapy was least likely to be associated with neonatal withdrawal (13%) while polytherapy was most likely (30%) (table 2). Neonatal withdrawal was significantly more frequent in those exposed to valproate monotherapy (p=0.006), phenytoin monotherapy (p=0.018), and polytherapy (p=0.001) than in the non-exposed group (χ2 analysis). Major malformations were significantly more frequent in those who suffered neonatal withdrawal than in those who did not (χ2 test, p=0.033), but other clinical features were not significantly more frequent (by χ2, minor malformations p=0.568, facial features p=0.115, and by Cox's proportional hazards, childhood medical problems p=0.053, developmental delay p=0.794, or behaviour problems p=0.657).
Childhood medical problems
Table 4 shows the frequency of eye abnormalities, joint laxity, otitis media with effusion, and other miscellaneous conditions in this category. In the present cohort, diagnosed refractive errors and other visual problems were not more frequent in the exposed children than in the non-exposed. There was an overall trend for myopia to be more common, and hypermetropia less common. Joint laxity was more common in those exposed to carbamazepine monotherapy (p=0.002), valproate monotherapy (p<0.001), and polytherapy (p=0.013). Childhood medical problems as a whole were more common in those exposed to carbamazepine (p<0.001), valproate (p<0.001), or polytherapy (p<0.001) (table 2), but not in those exposed to phenobarbitone (p=0.323) or phenytoin (p=0.061).
Pattern of childhood medical problems by drug exposure
Facial features
There was no statistically significant difference between the frequency of recognised fetal anticonvulsant syndrome facial features in the whole exposed group compared with the non-exposed children (table 1). Considering individual treatment groups, facial features were more commonly recognised following carbamazepine monotherapy (p=0.029), valproate monotherapy (p=0.005), and polytherapy (p=0.025) (table 2).
Influence of maternal drug dosage
In those exposed to monotherapy, there was no significant difference in maternal drug dosage between pregnancies with an adverse and a normal outcome for any clinical outcome category, with one exception. Children exposed to carbamazepine who had developmental delay were exposed to higher reported doses than children with normal development (mean daily dose 683 mg, compared with 462 mg, p=0.032). In addition, the difference in drug doses for those with and without facial features in the carbamazepine group almost reached statistical significance (p=0.055).
Non-exposed cohort
Thirty-eight sibs of exposed cases were not exposed to AEDs in utero (table 2). In 16 cases, the mother had epilepsy but took no treatment (seizures occurred during four pregnancies) and in 22 the child was born before epilepsy developed. Thirty-three children were normal and two had malformations. One had undescended testes and a family history of undescended testes. The other had contractures and learning difficulties and a family history of learning difficulties, involving an exposed sib and non-exposed cousins. Three had developmental delay without malformation. In one case (aged 14.6 years) developmental delay was attributed to meningitis at 9 weeks of age. Her two exposed sibs had no malformation or developmental delay. The other two were sibs and had similarly affected cousins.
Recurrence risk
Major malformation or developmental delay affected children in 68 of the 149 families. Counting the first affected child as the proband in each family, the probands had 65 sibs of whom 19 also had a major malformation or developmental delay. This gives a crude recurrence risk of 29%. Excluding those with a family history of developmental delay reduces the risk slightly to 14/54 or 26%. As many families had only one child, and therefore do not contribute to the crude recurrence risk estimate, we used Weinberg's proband method22 to allow for multiple incomplete ascertainment. This gives a recurrence risk of 43%, falling to 39% after excluding cases with a positive family history.
DISCUSSION
Although there have been many previous studies of pregnancy outcome in epileptic mothers taking AEDs, these have mainly focused on malformation rates in the first few months of life.4,6,7 The available data on long term consequences of exposure are based on small studies and are controversial.10 14 15 18 23 24 Our study set out to assess the long term consequences of intrauterine drug exposure on a population basis, by evaluation of children identified through their mother's maternity records.
We sought to ascertain all mothers who had taken antiepileptic drugs during pregnancy and delivered in Aberdeen since 1976. Because of the long interval since the earlier deliveries, some mothers could not be traced. In addition, some were not approached on the advice of their general practitioner, and some declined to take part, and these factors may have introduced bias. Nevertheless, the malformation rate in the exposed children in our study (13.8%) is comparable with that found in several prospective studies,1,4,6,7 suggesting that this bias may not be extreme.
Congenital malformation
Previous studies which involved review of birth records, assessment in the neonatal period, or assessment at 3 months found malformation rates overall of between 5% and 9.1%.1,4,6,7 In a 1973 records linkage study, 13.8% of exposed infants had malformations requiring intervention in the first year of life, although only 7.8% had malformations recognised at birth.25 Congenital heart disease, hernias, and pyloric stenosis accounted for the majority of the additional cases. In our study group, the sole major malformation was hernia in 10 cases, pyloric stenosis in three, and one case had Brown syndrome, an oculomotor malformation (table 3). One case with cleft soft palate was diagnosed at the age of 1 year 8 months. Excluding these cases would reduce the apparent malformation rate to 8%. Our relatively high malformation rate may therefore have resulted from the inclusion of more cases diagnosed after the neonatal period, rather than from a substantial effect of recruitment bias. The other malformations seen are similar to those documented in previous studies of fetal anticonvulsant syndromes. For example, there are three neural tube defects, one associated with carbamazepine alone, one with valproate and carbamazepine, and one with phenobarbitone alone. These findings are in keeping with previous reports suggesting that between 1% and 2% of pregnancies exposed to valproate7,26 or carbamezepine8 will have a neural tube defect. Some investigators have suggested that the increased malformation rate is a consequence of maternal epilepsy rather than drug exposure.2 Studies showing a correlation between malformation rate and drug dosage4,27 or polypharmacy,4,28 drug specific malformation rates,4,6 and the existence of animal models29 are more indicative of a teratogenic role for antiepileptic drugs. In keeping with this, polytherapy was associated with a significantly higher rate of malformation (p<0.012) in our study (table 2) while the various monotherapies were not. Although not statistically significant, our data suggest that phenytoin has a higher malformation risk than other monotherapies, and we found a higher rate with phenobarbitone than has usually been seen previously.4,6 The malformation rate in the non-exposed sibs of our cases (5.3%) is much lower than in the exposed cases overall, although numbers are small, and the difference is not statistically significant.
Neurodevelopment
In our study, 24% of the exposed group (26% of those over 21 months of age) had a developmental disorder compared with 10.5% of the non-exposed sibs (10.8% of those over 21 months). The relative risk of developmental disorder shows wide confidence intervals, despite the statistically significant association with AED exposure by Cox proportional hazards regression. This is likely to be because of the age dependent nature of the diagnosis of developmental delay, which is taken into account by Cox analysis, but not in the relative risk calculation. Nevertheless, the relative risks for this and other outcome measures are included in table 1, as they may be useful for counselling purposes. The rate of developmental delay following exposure to carbamazepine, valproate, or phenytoin alone and to polytherapy is significantly higher than in the non-exposed (table 2), while those exposed to phenobarbitone alone are not significantly different from the non-exposed sibs. In the carbamazepine exposed group, but not in the others, developmentally delayed children were exposed to significantly higher doses of AED during fetal life. A dose response effect on development in man has not been previously documented. No such effect was detected in the valproate and phenytoin groups, possibly because these drugs have a lower threshold for adverse developmental effects, or possibly because there were fewer children in these groups.
Three small prospective studies of between 25 and 41 children evaluating the frequency of developmental delay following fetal carbamazepine exposure previously found rates of between 8% and 20%.10,15,24 In a similar study of fetal phenytoin exposure, 20% had a global IQ score >1 SD below the mean.15 Recently, a large postal survey of epileptic women showed that 16% of 224 children who had been exposed to AEDs prenatally had additional educational needs compared with 11% of 176 exposed to no drugs (odds ratio 1.49, 95% CI 0.83-2.67).16 In that study, 30% of those exposed to valproate and 20% of those exposed to polytherapy including valproate had additional educational needs. An earlier study of school age children in Finland exposed to phenytoin, carbamazepine, barbiturates, or polytherapy found no increased risk of developmental delay, although subtle cognitive impairment including reduced auditory phonemic skills was detected.18
Among those over 21 months of age in our study group exposed to single drug therapy, the rate of developmental delay following valproate exposure was particularly high at 37% (table 5). Early reports of fetal valproate syndrome suggested a high frequency of developmental disorder associated with this drug30 and recent reports have tended to confirm this.13,16,31 In our cohort, exposure to valproate alone or carbamazepine alone was frequently associated with speech and language delay (fig 1). This is in keeping with previous reports of autism and communication disorder in fetal valproate syndrome.13,32,33 although communication disorders may be a more general effect of AED exposure in pregnancy, in the light of the findings in our carbamazepine exposed group and in the Finnish study.18 In addition, although our phenobarbitone exposed cases had the lowest rate of developmental delay, a previous study of 114 adult men found a modest reduction (equivalent to 0.5 SD) in verbal IQ compared with controls.19 It is likely that our study would not have detected such a subtle effect, as we did not undertake formal IQ testing. Eleven cases in our exposed group had autism or autistic spectrum disorders, mostly associated with valproate or carbamazepine. A high proportion of those exposed to phenytoin (33%) and to polytherapy (38%) also have a developmental disorder, although two of the eight affected children in the phenytoin group had only schooling difficulties with otherwise normal developmental milestones.
Influence of family history on proportion with developmental delay and/or congenital malformation
AED exposure is not the only possible cause for the developmental disorder. To evaluate a possible genetic aetiology, we undertook a family history review. When cases with a family history of developmental disorder were excluded, the frequency of developmental disorder only fell from 26% to 19% (table 5). Maternal epilepsy could be a risk factor for developmental disorder in the child through being a pleiotropic manifestation of a hereditary disorder of brain development, but if this is so, some of these cases should have been excluded by the family history review. It seems unlikely that seizures in themselves are usually the cause, as mothers had no seizures during 35/61 pregnancies in which the child subsequently had developmental delay, and only absence seizures in a further two. Maternal epilepsy or its treatment may affect the mother's ability to care for her child and stimulate his or her development, but this could not be assessed directly in isolation from other factors in this study. However, those families where parental learning disability may have influenced the child's development in a non-genetic fashion would also have been excluded by the family history review. When the familial cases are excluded, 20% of those exposed to valproate monotherapy are delayed and all have speech and language disorder. This may be seen in the context of a general population frequency of language impairment in 3-5 year olds of between 3% and 7.4%.34,35 The proportion of children with motor or global delay in the phenytoin and polytherapy groups is not changed by the exclusion of familial cases, perhaps reflecting a different pattern of neurotoxicity. Speech delay accounts for 8.3% and 19% of these groups respectively, which also have the highest overall rates of developmental delay (29% and 28%) in the absence of family history (table 5). Interpretation of the phenytoin group is difficult because of small numbers (only eight delayed children), although the high rate in the polytherapy group is probably a dose response effect. The qualitative and quantitative differences in patterns of development in the various exposure groups following exclusion of familial cases and the dosage effect in the carbamezepine group support the hypothesis of direct drug toxicity on the developing infant's nervous system. The developmental disorder is therefore likely to be multifactorial in origin, with genetic, teratogenic, and social effects all contributing. It should be noted that the group of children with major malformations, and the group with developmental delay do not fully coincide. The risk of either major malformation or developmental delay is therefore higher than the risk of either alone (tables 1 and 5).
Neonatal withdrawal
Infants exposed to antiepileptic drugs prenatally often present in the neonatal period with jitteriness, seizures, apnoeic episodes, feeding difficulties, and hypoglycaemia which may be attributable to drug withdrawal.23 Neonatal hypoglycaemia is common following valproate exposure and may be asymptomatic.36 Although it can cause cerebral damage and adverse neurodevelopmental outcome in other circumstances,37 it is not known whether this is important in the context of fetal antiepileptic drug exposure. In our cohort, neonatal withdrawal was documented at a similar frequency with each antiepileptic treatment regimen, and there was no relationship with reported drug dosage; maternal serum drugs levels were not routinely measured. We found no evidence of any effect of neonatal withdrawal on the subsequent frequency of developmental delay. This could reflect the active management of withdrawal, or may indicate that the developmental delay is not the result of perinatal factors. The statistical association of major malformation with neonatal withdrawal in our cohort may reflect the association of malformation with polytherapy. The frequency of neonatal withdrawal was highest in the polytherapy group, although this finding itself did not reach statistical significance.
Childhood medical problems
Later childhood medical problems were common in exposed children. Refractive errors and other ocular disorders were not as common as in our previous study of fetal valproate syndrome cases,38 although 34% of the polytherapy group were affected. The children exposed to valproate alone were on average younger than children in the other groups; 25% are less than 18 months old, compared with 14% in the polytherapy group. This may have reduced the likelihood of detecting a refractive error, although the lack of formal ophthalmic evaluation in this study may also be a factor. Interestingly, Cox regression analysis suggests that myopia is associated with carbamazepine monotherapy (p=0.009) and polytherapy (p=0.001), although no other specific ocular findings show statistical significance. Determination of the true frequency of eye abnormalities in this patient group awaits future research. In contrast, this study did confirm the high frequency of joint laxity and other connective tissue weakness in children exposed to valproate, or to polytherapy, and to a lesser extent to carbamazepine. This is reflected in the high frequency of hernias documented elsewhere. Otitis media with effusion was also common in the valproate group, but not particularly so following exposure to other drugs. Valproate does seem to be associated with a particular physical phenotype in preschool and school age children, including joint laxity, hernias, otitis media with effusion, and minor malformations particularly of the digits. This may aid recognition of fetal valproate syndrome in older children with a history of exposure and speech and language difficulties. Similarly, carbamazepine is associated with joint laxity, and autistic spectrum or attention deficit behaviour disorders, as is polytherapy. The association with polytherapy may reflect the fact that 19/50 of these children were exposed to combination therapy including valproate or carbamazepine or both.
Facies
Although we did not score the frequency of specific facial characteristics in our cohort, we used a check list of previously described facial features when reviewing the photographs. Facial features of fetal valproate syndrome include epicanthic folds, infraorbital groove, medial deficiency of the eyebrows, shallow nasal bridge, a short nose with anteverted nares and flattened tip, trigonocephaly, and a high forehead,39 while in fetal carbamazepine syndrome epicanthic folds, upward slanting palpebral fissures, and hypoplastic alae nasi occur. Hypertelorism and a broad nasal bridge are part of fetal phenytoin (hydantoin) syndrome. In infancy, a shallow philtrum, thin upper lip, and short nose with anteverted nares are common to these three fetal anticonvulsant syndromes.13 A typical face associated with prenatal exposure to phenobarbitone has not previously been described. In our study 3/12 photographed cases with no AED exposure were thought to have some of the facial characteristics of a fetal anticonvulsant syndrome. Although numbers are small, this finding is compatible with a previous study in which some facial features such as high forehead, frontal bossing, malar hypoplasia, epicanthic folds, and micrognathia were associated with maternal epilepsy, rather than with fetal AED exposure.14 A similar proportion of those exposed to phenobarbitone (21%) were thought to have facial features, suggesting that phenobarbitone may not have effects additional to those associated with maternal epilepsy, or that the features are not as recognisable as those described for other AEDs. Fetal anticonvulsant syndrome facies were seen in 52-70% of those exposed to carbamazepine, valproate, phenytoin, or polytherapy (the finding for phenytoin (p=0.12) was not statistically significant, probably owing to small numbers). This suggests that these drug regimens have much more easily recognised effects on facial development, and that these effects are more common than more clinically serious outcomes such as major malformation and developmental delay (32% of those exposed have at least one of these).
Teratogenic mechanisms
It has been suggested that some of the facial effects of phenytoin may be caused by relative vitamin K deficiency, resulting in maxillofacial hypoplasia.40 If this were the major mechanism, similar facial features might be expected following phenobarbitone exposure, but not following valproate exposure, whereas our study and other published reports suggest that the opposite is true. This is not to undervalue the essential role of prophylactic vitamin K therapy in preventing neonatal haemorrhage in infants who may be vitamin K deficient following exposure to phenobarbitone, phenytoin, carbamazepine, ethosuximide, primidone, or diazepam in utero.11 A number of mechanisms have been proposed for the wider teratogenic effects of antiepileptic drugs. Phenobarbitone, phenytoin, and carbamazepine reduce maternal folic acid levels, possibly through altered hepatic metabolism (all induce hepatic cytochrome P450).41 Valproate also alters folic acid metabolism in animal models.42,43 Abnormalities of maternal folic acid metabolism are associated with fetal malformations, particularly neural tube defects44 and possibly cleft palate45 in the non-epileptic population. Maternal folic acid status may also influence the risk of some forms of congenital heart disease.46 The possible role of folate metabolism in AED teratogenesis is supported by our previous finding of an association between maternal methylene tetrahydrofolate reductase (MTHFR) genotype and fetal anticonvulsant syndromes.47 Periconceptional folic acid supplementation has therefore been recommended for mothers with epilepsy,11 although no evidence of protection by low dose (0.4 mg) folic acid supplementation was found in one recent small case-control study.48 Alternatively, some AEDs or their metabolites may have a direct toxic effect on fetal tissues. In mouse models, valproate has been shown to accumulate in the neuroepithelium49 and to alter intracellular pH in the limb bud,50 findings which might support such a direct effect. Reduced activity of epoxide hydrolase, an enzyme involved in the elimination of phenytoin metabolites, increases the risk of fetal phenytoin syndrome, 51 suggesting that metabolites may be important in some cases. Recent studies have shown changes in gene expression in animal models following phenytoin52 or valproate exposure,53,54 indicating that these drugs may interfere with developmental pathways directly. Disentanglement of this complex area awaits further research.
Recurrence risk
In our previous study of a cohort of children with fetal anticonvulsant syndromes, we found a sib recurrence risk of 55%.13 In this study, we have not classified children as having specific syndromes but rather have evaluated the risk of a serious adverse outcome (major malformation or developmental delay) in sibs of affected children. The calculated recurrence risk is slightly lower at 43%, and is reduced to 39% when those cases with a family history of developmental delay are excluded. This compares with the risk of occurrence of major malformation or developmental delay of 26% (table 5), after exclusion of the positive family history cases. This supports the concept of an underlying genetic susceptibility to adverse fetal outcome in pregnancies of epileptic mothers which is independent of other family history. Although some of the genetic susceptibility factors may have already been identified,47,51 much work remains to be done in characterising these factors, as they may allow better targeting of maternal antiepileptic therapy to minimise the risk to the fetus in the future.
CONCLUSION
This study highlights the high frequency of later childhood complications associated with maternal epilepsy and its treatment, and emphasises the need for appropriate counselling and support of epileptic mothers. Joint laxity and behaviour disorders are associated with valproate and carbamazepine exposure. For a mother considering pregnancy, AED therapy with the drug regimens observed in this study is associated with a two to three fold increased risk of major malformation or developmental delay (relative risk 2.38, 95% CI 1.03-5.51). The developmental disorder is likely to have a multifactorial aetiology, but single drug therapy with valproate, phenytoin, or carbamazepine and polytherapy are all associated with a substantial risk of developmental delay, even when possible genetic factors are excluded, and a dose response effect for carbamazepine and developmental delay has been shown. The influence of an impaired mother-child interaction in the early years because of maternal epilepsy or its treatment requires further study. As discontinuation of epilepsy treatment in pregnancy because of the teratogenic risk is not usually an option, the importance of further research into susceptibility factors, the development of safer drugs, and the appropriate counselling and management of epileptic women cannot be overemphasised.
Acknowledgments
We are grateful for the assistance of Dr Doris Campbell in ascertaining mothers from the Aberdeen Maternity and Neonatal Database, and for support from the Aberdeen Special Nursery Trust, and the Chief Scientist's Office of the Scottish Health Department.