Article Text

Abstract
Objectives Atrial fibrillation (AF) is associated with increased morbidity and mortality in patients with hypertrophic cardiomyopathy (HCM). The primary aim of this study (HCM Risk-AF) was to determine the predictors of AF in a large multicentre cohort of patients with HCM. Exploratory analyses were performed to investigate the association between AF and survival and the efficacy of antiarrhythmic therapy in maintaining sinus rhythm (SR).
Methods A retrospective, longitudinal cohort of patients recruited between 1986 and 2008 in seven centres was used to develop multivariable Cox regression models fitted with preselected predictors. HCM was defined as unexplained hypertrophy (maximum left ventricular wall thickness of ≥15 mm or in accordance with published criteria for the diagnosis of familial disease). 28% of patients (n=1171) had coexistent hypertension. The primary end point was paroxysmal, permanent or persistent AF detected on ECG, Holter monitoring or implantable device interrogation.
Results Of the 4248 patients with HCM without pre-existing AF, 740 (17.4%) reached the primary end point. Multivariable Cox regression revealed an association between AF and female sex, age, left atrial diameter, New York Heart Association (NYHA) class, hypertension and vascular disease. The proportion of patients with cardiovascular death at 10 years was 4.9% in the SR group and 10.9% in the AF group (difference in proportions=5.9%; 95% CI (4.1% to 7.8%)). The proportion of patients with non-cardiovascular death at 10 years was 3.2% in the SR group and 5.9% in the AF group (difference in proportions=2.8%; 95% CI (0.1% to 4.2%)). An intention-to-treat propensity score analysis demonstrated that β-blockers, calcium channel antagonists and disopyramide initially maintained SR during follow-up, but their protective effect diminished with time. Amiodarone therapy did not prevent AF during follow-up.
Conclusion This study shows that patients with HCM who are at risk of AF development can be identified using readily available clinical parameters. The development of AF is associated with a poor prognosis but there was no evidence that antiarrhythmic therapy prevents AF in the long term.
Statistics from Altmetric.com
Introduction
Hypertrophic cardiomyopathy (HCM) is a myocardial disorder characterised by left ventricular (LV) hypertrophy not explained solely by abnormal loading conditions.1 Atrial fibrillation (AF) is a common complication of the disease and a number of studies have suggested that it is associated with adverse clinical outcomes and reduced survival.2–5 In order to prevent AF and its sequelae, it is necessary to develop methods for stratifying patients into subgroups that will derive most benefit from targeted therapeutic strategies. In a recent multicentre study (HCM Risk-CVA) we demonstrated that patients at high risk of thromboembolic stroke can be identified using a small number of simple clinical parameters including a history of AF.6 The primary aim of this study was to determine predictors of new onset AF in the same cohort. Additional exploratory analyses were performed to investigate the effect of AF on mortality and the efficacy of antiarrhythmic therapy in the prevention of AF.
Methods
Study design and overview
This study uses data from a retrospective, multicentre longitudinal cohort (HCM Risk-CVA).6
The study conforms to the principles of the Declaration of Helsinki. The sponsors of this study did not have a role in study design, data collection, analysis and interpretation. OPG, MP, RZO and PME had access to all data and had final responsibility to submit the article. The authors from each participating centre guarantee the integrity of data from their institution. All investigators have agreed to the article as written.
Study population and participating centres
The study cohort has been described in detail in a previous manuscript on thromboembolism in HCM (HCM Risk-CVA).6 Subgroups of patients from this cohort have been reported in other recently published studies (see online supplementary table S1). The study cohort consisted of all consecutively evaluated patients with HCM, followed at seven participating European centres: (i) The Heart Hospital, University College London, London, UK, (ii) A Coruña University Hospital, A Coruña, Spain, (iii) Unit of Inherited Cardiovascular diseases, First Department of Cardiology, University of Athens, Greece, (iv) Institute of Cardiology, University of Bologna, Italy, (v) University Hospital Virgen de la Arrixaca, Murcia, Spain, (vi) Monaldi Hospital, Second University of Naples, Italy and (vii) Hospital Universitario Puerta del Hierro, Madrid, Spain.
supplementary tables
Only adult patients (≥16 years of age) were studied. HCM was defined as a maximum LV wall thickness of ≥15 mm unexplained solely by loading conditions7 or in accordance with published criteria for the diagnosis of disease in relatives of patients with unequivocal disease.8 Patients with known inherited metabolic diseases or syndromic causes of HCM were excluded from the study. For the study of AF predictors, patients with AF at first evaluation were excluded from the analysis.
Ethics approval
Ethics approval and written informed consent was obtained for each participating centre. Patients at A Coruña University Hospital (Spain), First Department of Cardiology, University of Athens (Greece), University Hospital Virgen de la Arrixaca (Spain) and Monaldi Hospital (Italy) provided written informed consent. The data collection at The Heart Hospital (UK), Universitario Puerta de Hierro (Spain) and at the Institute of Cardiology at the University of Bologna (Italy) has been approved by the appropriate local ethics committee.
Patient assessment and data collection
All patients underwent pedigree analysis, clinical assessment, physical examination, resting and ambulatory ECG and transthoracic echocardiography as previously described.6 Each participating centre collected data independently. Patients were reviewed every 6–12 months or earlier if there was a change in symptoms.
Clinical outcomes
The primary outcome was paroxysmal, permanent or persistent AF detected on ECG, Holter monitoring or device interrogation. The secondary outcome was all-cause and cardiovascular mortality (defined as sudden cardiac death, heart failure-related death, stroke-related death and other cardiac death). Sudden cardiac death was defined as witnessed sudden death with or without documented ventricular fibrillation or death within 1 hour of new symptoms or nocturnal deaths with no antecedent history of worsening symptoms.9 Heart failure-related death was defined as death preceded by signs and symptoms of heart failure or cardiogenic shock. Stroke-related death was defined as any death preceded by stroke. Pulmonary embolism and myocardial infarction were included in other cardiovascular death. All other deaths were considered as non-cardiovascular.10
Selection of predictors and coding
Candidate predictor variables were selected following a review of the literature completed in September 2012.11 Clinical parameters were used as pre-specified predictor variables only when associated with AF in at least one published study. All parameters used in the final model were uniformly defined in all participating centres. In addition to these variables, predictors known to be associated with AF in the general population such as hypertension, diabetes mellitus and vascular disease were considered (table 1). All predictors were determined at baseline evaluation.
Definition of pre-specified predictor variables assessed at baseline evaluation
Sample size
Based on a regression analysis to examine the relationship between explanatory variables and AF, a minimum of 10 AF events are required per coefficient estimated by the model to ensure that the regression coefficients are estimated with adequate precision.15 The 740 AF end points observed in this cohort over a 10-year follow-up period allow the estimation of all 11 candidate regression coefficients (as shown in table 1) in a multivariable regression model and also adjust for possible centre effects.
General statistical methods
STATA (V.12) and R (V.3.0) were used for the statistical analyses. For descriptive results, variables are expressed as mean±SD, median and IQR or counts and percentages as appropriate. The follow-up time for each patient was calculated from the date of their first evaluation at participating centres to the date of the relevant end point or to the date of their most recent evaluation. The annual event rate was calculated by dividing the number of patients reaching the end point by the total follow-up period for that end point. The Kaplan-Meier method was used to estimate the cumulative probability for the occurrence of an outcome.
Missing data
The characteristics of patients with missing information were compared with those of patients with complete information to investigate bias due to missing data. Logistic regression was used to identify the predictors of missingness. Data were assumed to be missing at random and values for the missing predictors were imputed using multiple imputation techniques based on chained equations.16 The multiple imputation model included all predictors of missingness, the outcome, all pre-specified predictors of the risk model and the estimate of the cumulative hazard function.17 Rubin's rules were used to combine the estimates from 30 imputed datasets.18 We also carried out a complete case analysis, excluding patients with missing observations in any of the candidate predictor variables.
Survival analysis
Univariable and multivariable Cox regression models were fitted and tested for non-linearity of continuous predictors by inclusion of quadratic terms. The final Cox regression model for AF was developed using backward elimination and a 15% significance level was used to select the predictors.19 The proportional hazards assumption was investigated using Schoenfeld residuals.20 A sensitivity analysis was performed using a model stratified by centre. As part of the sensitivity analysis, a complete case analysis of patients with no missing data was also carried out.
Cardiovascular and non-cardiovascular mortality was compared in patients with AF and sinus rhythm (SR) at any time during the follow-up period of 10 years. Patients with AF at first evaluation were included for this analysis.
A propensity score analysis was used to investigate clinical outcomes in patients receiving β-adrenoreceptor blockers, non-dihydropyridine calcium channel antagonists, disopyramide and amiodarone. If a patient received treatment at any time prior to the event, it was assumed that the patient continued on this medication until the end point of the study was reached or the end of follow-up. The effect on development of AF was investigated. A sub-analysis was performed to assess the relationship between risk of AF and left atrial (LA) size.
Results
The initial study cohort comprised 5104 patients. Of these, 197 were only seen once at baseline evaluation and so were excluded from all subsequent analyses. The remaining cohort of 4907 patients was used to model the relation between AF and survival; 659 patients had AF prior to first evaluation and were excluded from the analysis of new AF events (table 2). Missing data per variable are presented in online supplementary table S2. Clinical characteristics of the patients with AF at baseline evaluation, who were excluded, are presented in online supplementary table S3.
Clinical characteristics of whole cohort (4907 patients) and in patients with and without AF (740 and 4167 patients, respectively)
Predictors of AF
AF events during follow-up
During a follow-up period of 22 743 patient-years (median 5.4 years), 740 out of 4248 patients (17.4%) who were in SR at baseline reached the primary end point within 10 years of first evaluation. Of the 732 patients with the type of AF recorded, 423 patients (57.8%) had paroxysmal AF and 309 patients (42.2%) had permanent/persistent AF. The 5-year and 10-year cumulative incidence rates of AF were 16.0% (95% CI 14.6% to 17.5%) and 33.3% (95% CI 30.7% to 36.1%), respectively. The clinical characteristics of patients with and patients without AF during the follow-up period are shown in table 2.
Univariable and multivariable analyses for primary end point
The models for predicting new onset AF were developed using the 740 events within the first 10 years of follow-up. Univariable analyses are shown in table 3. Maximal LV wall thickness and LA size had a non-linear association with AF and so a quadratic term was included in the multivariable analysis.
Univariable analysis for predictors of atrial fibrillation in hypertrophic cardiomyopathy
Multivariable Cox regression showed an association between new onset AF and the following: female sex, age, LA diameter (and its quadratic term), New York Heart Association (NYHA) class II, NYHA class III/IV, hypertension and vascular disease as shown in table 4. A test based on Schoenfeld residuals did not indicate a violation of the proportional hazards assumption (global test p value >0.3 for the models in all of the imputed datasets).
Multivariable analysis for predictors of atrial fibrillation in hypertrophic cardiomyopathy
A model including centre was also considered. There was a significant centre effect on AF; however, the proportional hazards assumptions were violated for some of the imputed datasets (global p value <0.05). We therefore considered a Cox model stratified by centre as part of a sensitivity analysis, for which the proportional hazards assumption was satisfied for all of the imputed datasets (global p value >0.2). The results were very similar and are presented in the online supplementary tables (see online supplementary table S4). Clinical characteristics according to centre are displayed in online supplementary table S5.
Sensitivity analyses
As part of the sensitivity analysis, a complete case analysis of patients with no missing data (n=3831; 676 events) was also performed. This analysis showed an association between new onset AF and the same variables except for vascular disease and hypertension. This could be due to smaller sample of patients included in the analysis.
Relation of LA size to AF
Using the multivariable Cox regression model (table 4), we calculated the risk of AF for a range of values for LA size (the values of the other predictors in the model were fixed at their mean value). The predicted risks of AF were then plotted against the values for LA size (figure 1). There was a linear relationship between LA size and AF risk above a diameter of 40 mm.
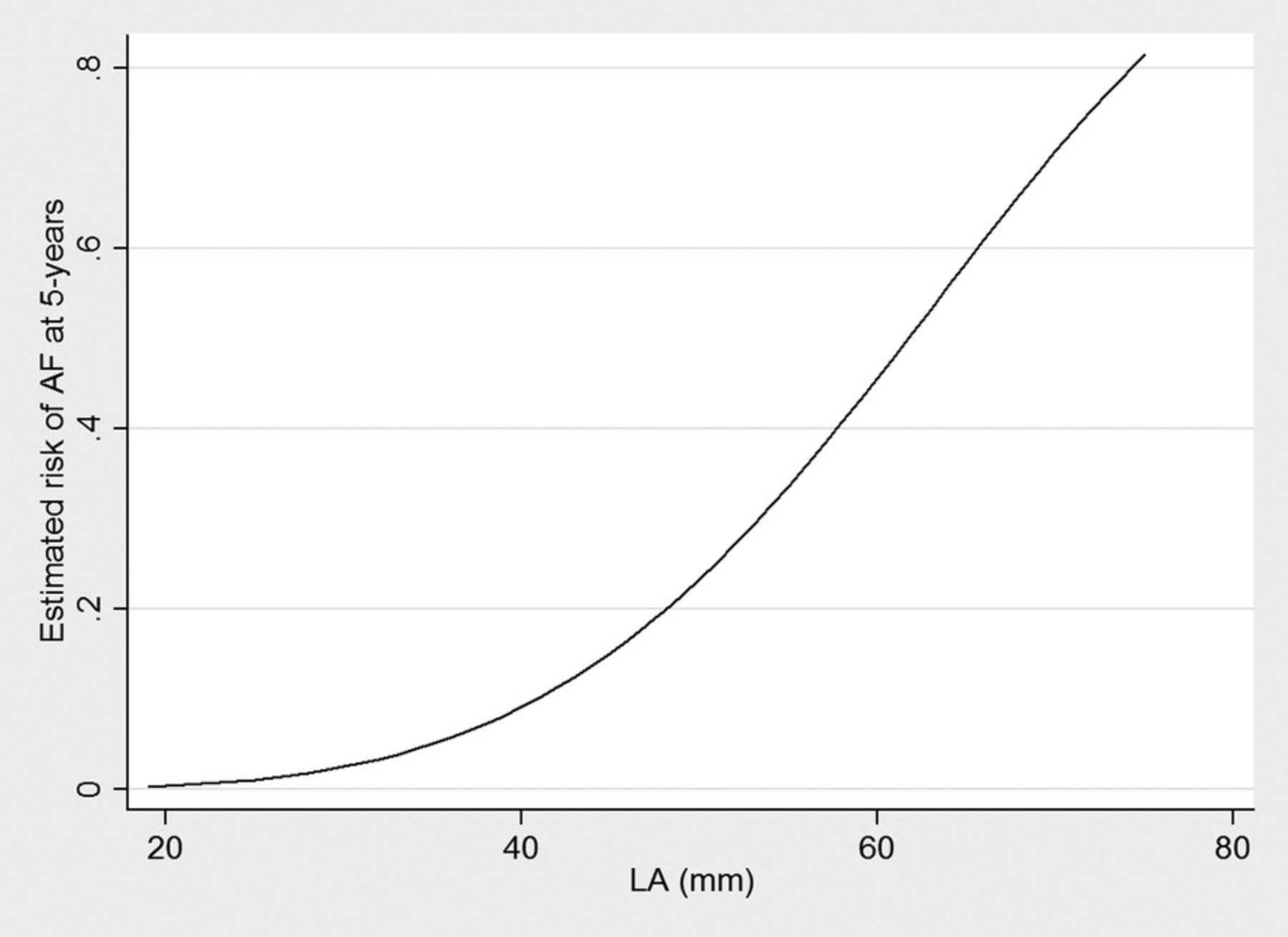
Graph showing the relationship of left atrial (LA) size with risk of atrial fibrillation (AF).
Mortality in patients with AF and SR
Patients with unknown date (n=47) or cause of death (n=25) were excluded from this analysis. The proportion of patients with cardiovascular death was 8.4% over the whole follow-up period (95% CI 7.6% to 9.2%) (405 out of 4835 patients). The proportion over a 10-year follow-up was 6.7% (95% CI 5.9% to 7.3%) (317 out of 4835 patients). The proportion of patients with non-cardiovascular death was 4.9% over the whole follow-up period, (95% CI 4.2% to 5.4%) (234 out of 4835 patients). The proportion over a 10-year follow-up was 3.91% (95% CI 3.4% to 4.5%) (189 out of 4835 patients).
Patients in AF at any time were more likely to experience cardiovascular death (10.9% in the AF group vs 4.9% in the SR group (difference in proportions=5.9%; 95% CI (4.1% to 7.8%)) and non-cardiovascular death (5.9% in the AF group vs 3.2% in the SR group (difference in proportions=2.8%; 95% CI (0.1% to 4.2%)) than patients in SR over the 10-year follow-up. There was an increased mortality in patients with permanent and persistent AF compared with paroxysmal AF (difference in proportions=8.1%; 95% CI (4.5% to 11.7%)).
Effect of antiarrhythmic drugs on clinical outcomes
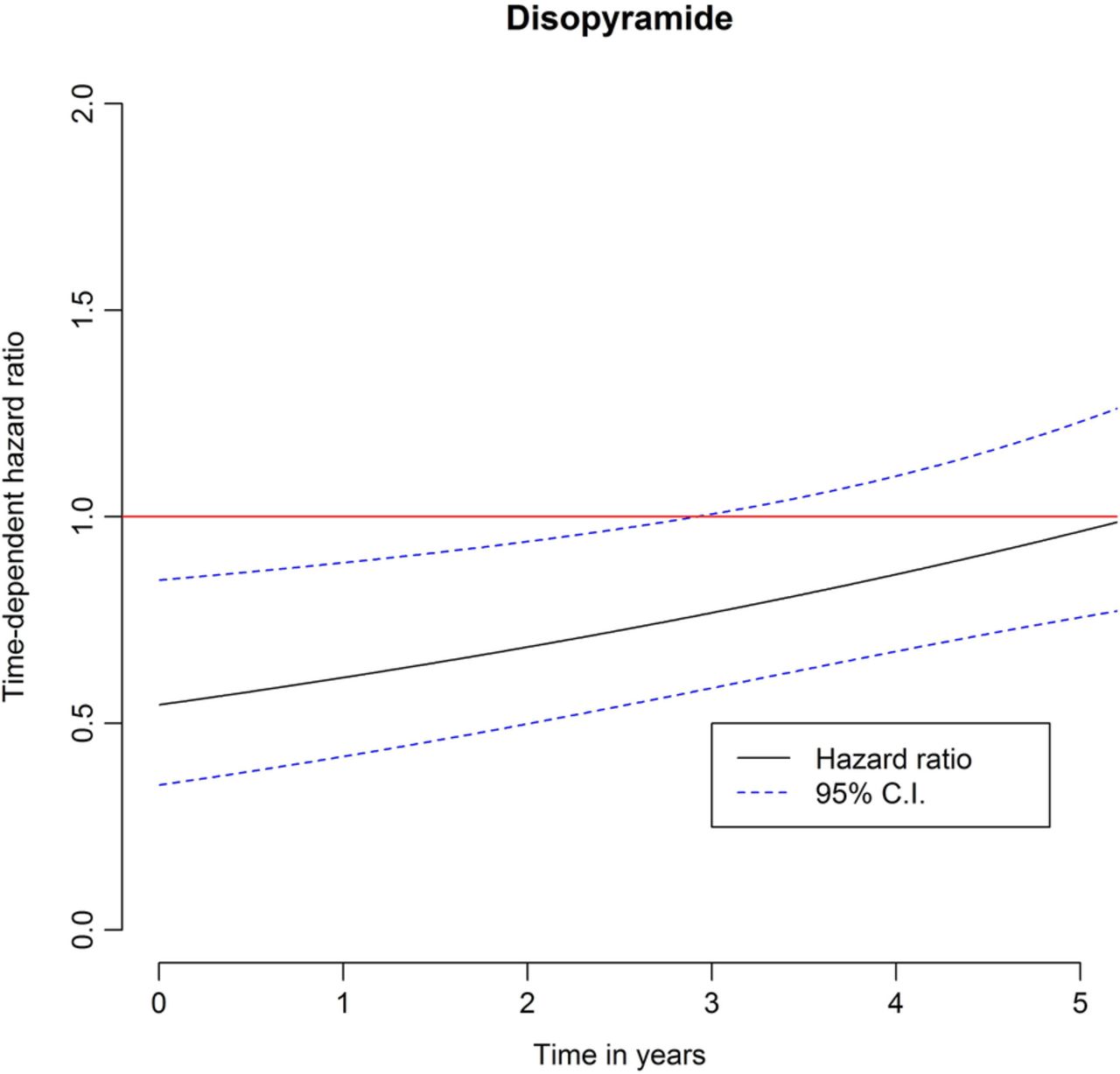
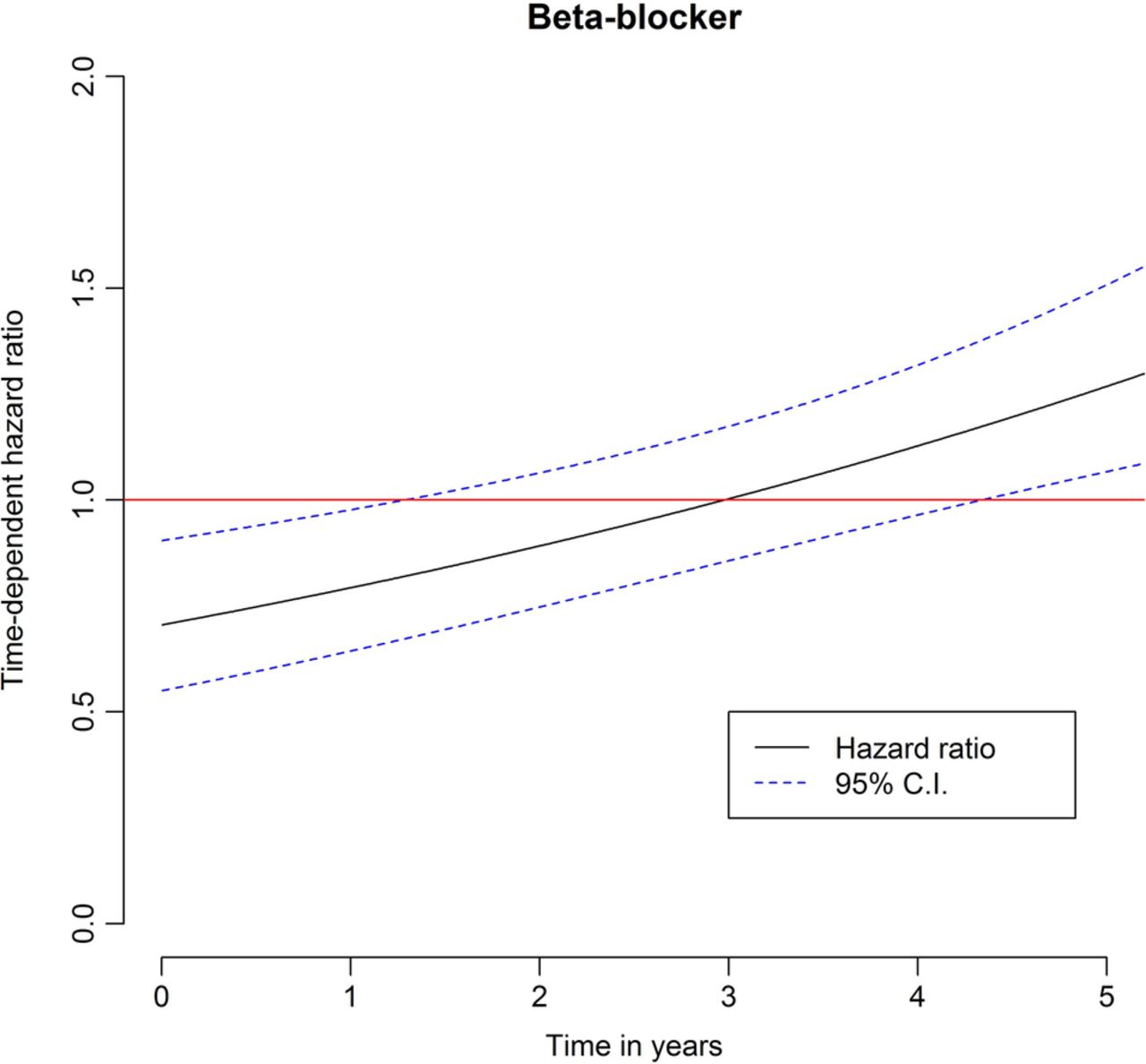
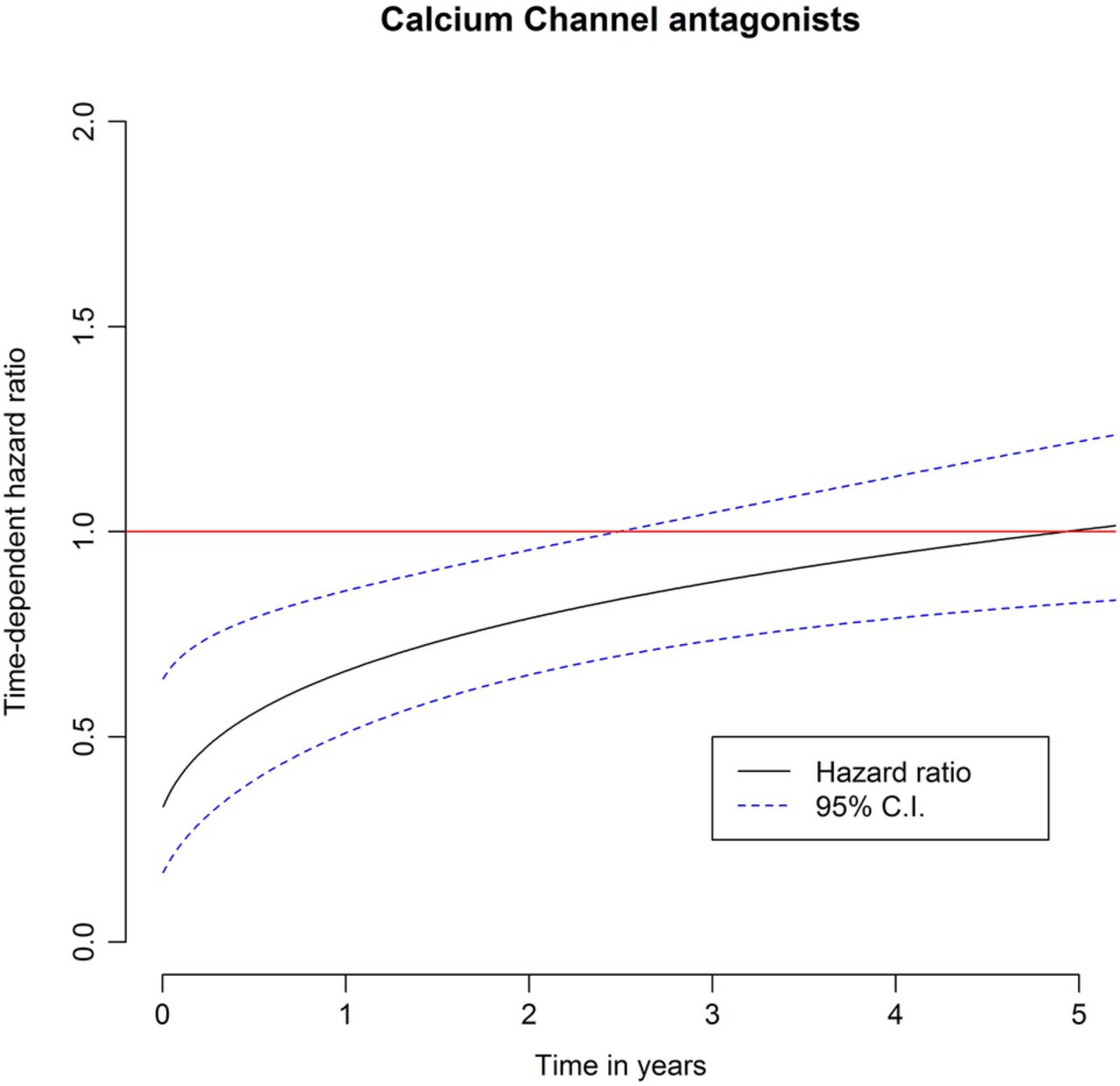
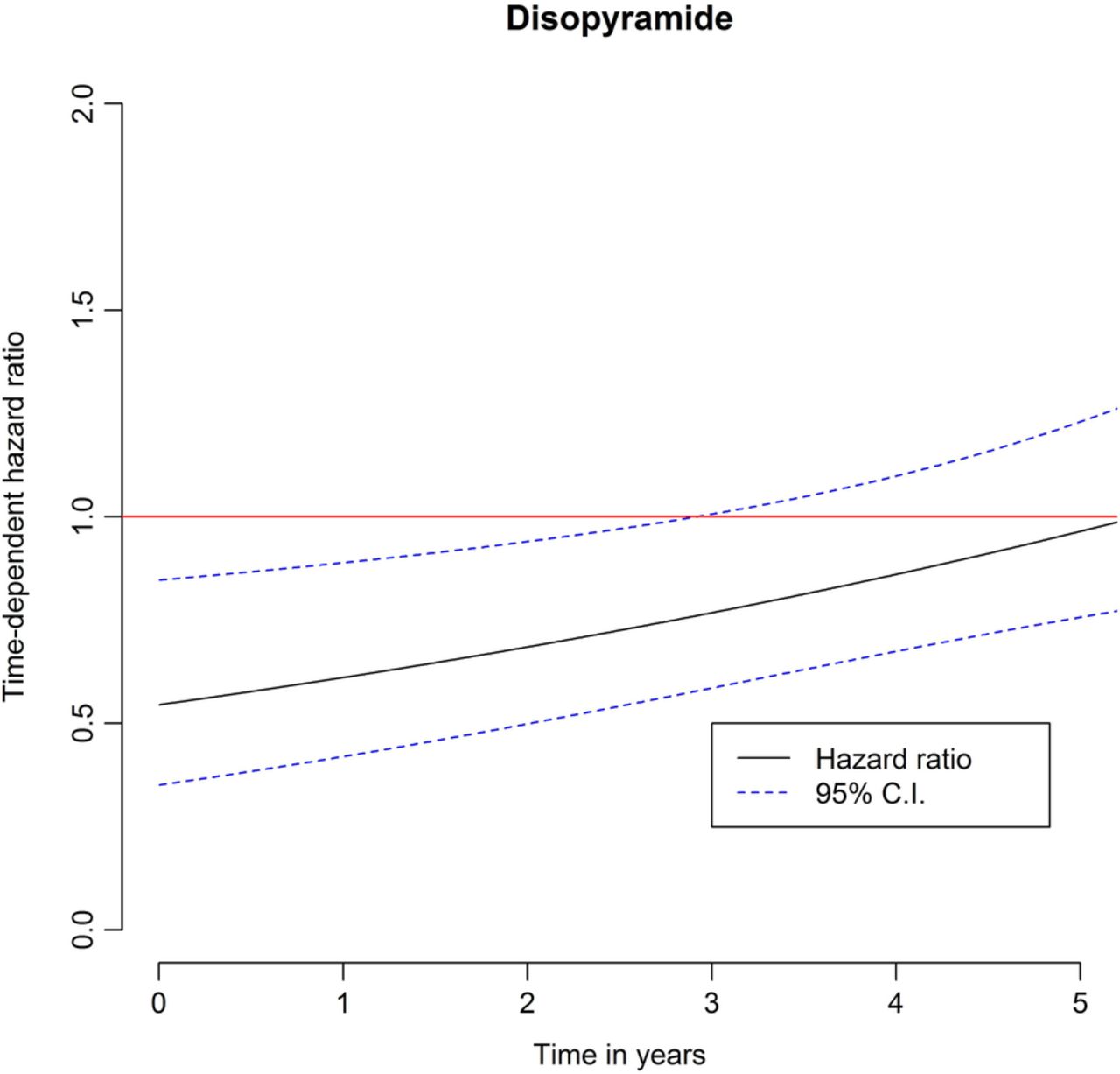
For each therapy, a Cox regression model for the time to AF adjusting for therapy and the propensity score was considered.21 For disopyramide, β-blocker and calcium channel antagonists, the proportional hazards assumption was not satisfied, meaning that the effect of treatment on AF varies with time. To account for this effect we analysed the effect of therapy over time. Plots for the Schoenfeld residuals20 revealed a decreasing effect of therapy with time (for all three therapies). According to Schoenfeld plots, a decreasing linear trend of the effect of therapy with time appeared plausible for disopyramide and β-blockers. A linear trend could not be assumed for calcium channel antagonists and hence a log transformation for time was used.
Disopyramide, β-blocker and calcium-channel antagonists initially had a protective effect (HR <1) but this effect seems to be attenuated with time (figures 2⇓–4). This could be explained by disease progression. A further reason could be the fact that the propensity score accounts for the probability of patients receiving therapy given their characteristics at baseline but does not account for the probability of receiving therapy for patients whose characteristics changed during follow-up and the patients received therapy or switched from one therapy to another after baseline.

Propensity score analysis for development of atrial fibrillation over 5-year follow-up period in treatment and non-treatment groups (time-varying effect of β-blocker).

Propensity score analysis for development of atrial fibrillation over 5-year follow-up period in treatment and non-treatment groups (time-varying effect of calcium channel antagonist).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Propensity score analysis for development of atrial fibrillation over 5-year follow-up period in treatment and non-treatment groups (time-varying effect of disopyramide).
The effect of amiodarone was not statistically significant (HR=1.12; 95% CI (0.89 to 1.36)) and did not appear to vary over time. In light of these findings, we examined the number of patients on amiodarone in the absence of a diagnosis of AF at first evaluation. Out of 311 patients receiving amiodarone at first evaluation, only 23 had a prior diagnosis of AF.
Discussion
This study confirms the high prevalence of AF in HCM and reveals an association between AF and atrial size, NYHA class and age.3 ,4 ,11 For the first time in a HCM population, we demonstrate an association between AF and several other patient characteristics including sex, hypertension and vascular disease.
Prevalence, incidence of AF and mortality
The prevalence and incidence of AF and mortality are in line with previous cohort studies in patients with HCM.4 ,5 ,11 ,22 Evidence for the detrimental effect of AF on survival is limited in HCM,4 ,11 but in this study we show a significant association with cardiovascular mortality reflecting a higher proportion of heart failure and stroke-related death in the AF group. It is possible that, in patients who die of heart failure, the onset of AF accelerates disease progression. Alternatively, AF may simply be a marker that identifies patients with advanced disease who are already on an accelerated trajectory to ventricular failure. The trend towards increased non-cardiovascular mortality in the AF group is likely to represent a complex interplay between some miscoding of deaths and the adverse consequences of cardiac disease and therapy on general health.
Effect of antiarrhythmic therapy on AF development
There are no prospective randomised trials of medical therapy for AF in HCM and only a very small number of observational studies assessing the effect of antiarrhythmic therapy on the maintenance of SR.5 ,23 In this study a propensity score analysis demonstrated that β-blockers, calcium channel antagonists and disopyramide at baseline initially prevented AF for the first 2–3 years of follow-up, but their protective effect then diminished. The retrospective nature of the analysis and the intention-to-treat analysis means that these findings should be interpreted cautiously, but it is likely that this loss of a therapeutic effect reflects the inexorable progression of disease. Contrary to expectations, amiodarone therapy did not have a protective effect on the development of AF. However, a large proportion of patients on amiodarone did not have a history of AF at first evaluation and we speculate that the apparently neutral effect of the drug might be explained by its historical use to prevent sudden cardiac death in patients with non-sustained ventricular tachycardia as this group of patients may have more myocardial fibrosis and advanced disease and thus be less likely to respond.24 ,25
Clinical implications
This study confirms the importance of AF in the natural history of HCM.1 The findings in this and our previous study on stroke in HCM6 suggest that patients with risk factors for AF should undergo frequent ambulatory ECG monitoring to detect atrial arrhythmia and could be considered for early prophylactic anticoagulation. The identification of associations with common cardiovascular risk factors such as vascular disease and hypertension is not by itself that surprising but shows that management of these risk factors should be given equal priority to other disease-specific complications. In spite of its limitations, the propensity score analysis for antiarrhythmic therapy suggests that rhythm control strategies for patients with AF and HCM are suboptimal and require revaluation in prospective randomised trials.
Limitations
The predictors identified in this study may not apply to patients with different characteristics. In particular, the study excludes paediatric patients (<16 years) and patients with metabolic or syndromic disorders in whom other disease characteristics may influence the risk of AF development.
Changes in imaging technology, rhythm monitoring and device therapy may be relevant over the long follow-up period.
The significant centre effect can be explained by the difference in some of the characteristics of the participating cohorts including follow-up time and prevalence of AF during the follow-up period. Further work is necessary to understand this, but it might reflect systematic differences in referral patterns.
Conclusions
Readily available clinical parameters can be used to identify patients at high risk of AF who require more frequent monitoring and early anticoagulation. Some of these variables have previously been described and reflect disease progression. In the exploratory analyses, AF was associated with increased cardiovascular and non-cardiovascular mortality. Although β-blockers and calcium antagonists may be useful for rate control in patients with persistent and permanent AF, there was no evidence for a sustained beneficial effect of antiarrhythmic therapy on the development of atrial arrhythmia.
Key messages
What is already known on this subject?
Atrial fibrillation (AF) is a common complication of hypertrophic cardiomyopathy (HCM) and a number of studies have suggested that it is associated with adverse clinical outcomes and reduced survival.
What might this study add?
In this study, 17.4% of patients developed AF during the follow-up period. Multivariable Cox regression revealed an association between the occurrence of new onset AF and the following: female sex, age, left atrial diameter, New York Heart Association (NYHA) class, hypertension and vascular disease. Patients with AF had more than twofold increased risk of cardiovascular death at 10 years. An intention-to-treat analysis using propensity score suggested that β-blockers, calcium channel antagonists and disopyramide initially maintained sinus rhythm, but their protective effect diminished with time. Amiodarone therapy did not prevent AF during follow-up.
How might this impact on clinical practice?
This study confirms the importance of AF in the natural history of HCM. Patients with risk factors for AF should undergo frequent ambulatory ECG monitoring to detect atrial arrhythmia and could be considered for early prophylactic anticoagulation. Common cardiovascular risk factors such as vascular disease and hypertension should be given equal priority to other disease-specific complications.
References
Footnotes
Collaborators Additional Hypertrophic Cardiomyopathy Outcomes investigators. Maite Tomé-Esteban1, Antonis Pantazis1, Shaughan Dickie1, Xusto Fernandez2, Angela Lopez2, Vasiliki Vlagkouli3, Antonio Romero4, Andrea Buono5, Giuseppe Pacileo5, Maria Gallego-Delgado6 and Marta Cobo-Marcos6: (1) The Inherited Cardiac Diseases Unit, The Heart Hospital/University College London, 16-18 Westmoreland St, London W1G8PH, UK; (2) Cardiology Department and Research Unit, A Coruña University Hospital, Galician Health Service, Spain; (3) Unit of Inherited Cardiovascular Diseases, First Department of Cardiology, University of Athens, 99 Michalakopoulou St, Athens 11527, Greece; (4) Cardiac Department, University Hospital Virgen Arrixaca, Murcia-Cartagena s/n. El Palmar, Murcia, 30120, Spain; (5) Monaldi Hospital, Second University of Naples, Via Leonardo Bianchi 1, Naples 80131, Italy; (6) Heart Failure and Inherited Cardiac Diseases Unit, Hospital Universitario Puerta del Hierro Majadahonda, Manuel de Falla, 1, 28222, Madrid, Spain.
Contributors OPG designed the study, collected and interpreted the data, carried out the descriptive statistical analysis and wrote the article. PME designed the study, interpreted the data and wrote the article. RZO was involved in study design, led the statistical aspects of the risk modelling and wrote the article. MP was involved in the study design and carried out the statistical analysis. COM, LM, AA, EB, JRG, GL, PG-P and CR collected and interpreted the data and critically reviewed the manuscript. WJM was involved in the drafting of the article and revised it critically for important intellectual content. Antonis Pantazis, Maite Tome-Esteban, Shaughan Dickie, Xusto Fernandez, Angela Lopez, Vasiliki Vlagkouli, Antonio Romero, Andrea Buono and Maria Gallego-Delgado and Marta Cobo-Marcos were involved in data collection and interpretation.
Funding This study was funded by the British Heart Foundation and by the National Institute for Health Research University College London Hospitals Biomedical Research Centre. It was also partially supported by the Red Investigación Cardiovascular from the Instituto de Salud Carlos III, Spanish Ministry of Health (grants RD12/0042/0049, RD12/0042/0066 and RD12/0042/0069) and Project No. PI11/02604, integrated in the National Plan for Scientific Research, Development and Technological Innovation 2008–2011 and funded by the ISCIII-General Subdirection of Assessment and Promotion of the Research—European Regional Development Fund ‘A way of making Europe’. OPG received research support from the British Heart Foundation (FS/12/86/29841) and the National Institute for Health Research University College London Hospitals Biomedical Research Centre.
Competing interests None declared.
Ethics approval West of Scotland Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.