Article Text

Abstract
Background The International Quality Improvement Collaborative (IQIC) was formed to reduce mortality and morbidity from congenital heart disease (CHD) surgeries in low/middle-income countries.
Objectives We conducted this study to compare the postoperative outcomes of CHD surgeries at a centre in Pakistan before and after joining IQIC.
Methods The IQIC provides guidelines targeting key drivers responsible for morbidity and mortality in postoperativepatients with CHD. We focused primarily on nurse empowerment and improving the infection control strategies at our centre. Patients with CHD who underwent surgery at this site during the period 2011–2012 (pre-IQIC) were comparedwith those getting surgery in 2013–2014 (post-IQIC). Morbidity (major infections), mortality and factors associated with them were assessed.
Results There was a significant decrease in surgical site infections and bacterial sepsis in the post-IQIC versus pre-IQIC period (1% vs 30%, p=0.0001, respectively). A statistically insignificant decrease in the mortality rate was also noted in post-IQIC versus pre-IQIC period (6% vs 9%, p=0.17, respectively). Durations of ventilation and intensive care unit (ICU) and hospital stay were significantly reduced in the post-IQIC period. Age <1 year, malnutrition, low preoperative oxygen perfusion, Risk Adjustment for Congenital Heart Surgery score >3, major chromosomal anomalies, perfusion-related event, longer ventilation and ICU/hospital stay durations were associated with greater odds of morbidity and mortality.
Conclusion Enrolling in the IQIC programme was associated with an improvement in the postsurgical outcomes of the CHD surgeries at our centre.
- congenital heart disease
- surgical outcomes
- developing country
- quality improvement
Statistics from Altmetric.com
Introduction
Congenital heart diseases (CHDs) are the most common congenital anomalies, affecting 1% of births each year.1 Approximately 3/1000 children will require CHD surgeries within the first month of life.2 Congenital heart programmes are essential for access to life-saving surgeries. The success of these programmes is determined by quality of intervention and postoperative care provided to patients. Emerging programmes in low/middle-income countries, however, may lack the institutional framework and skilled multidisciplinary teams necessary to provide appropriate care.3 Limitations faced by low/middle-income countries include lack of financial resources, poor infrastructure, lack of equipment and a shortage of trained staff and specialists.4 5 Consequently, surgical mortality is 10 times higher in these countries than in industrialised nations.6
The International Quality Improvement Collaborative (IQIC) for congenital heart surgery was established in 2007 to address the lack of quality evaluation of surgical programmes in low/middle-income countries and to identify risk factors contributing to poor surgical outcomes. The collaboration aims to reduce surgical mortality and complications in low/middle-income countries and to benchmark programmes to track progress. Three ‘key drivers’ crucial to reducing mortality after CHD surgery were identified: safe perioperative practice, reduction of surgical site infections (SSIs) and bacterial sepsis, and team-based practice through nurse empowerment.3 Strategies to address each of these were developed, a data registry for all participating sites was created and a telecommunications platform for educating the multidisciplinary teams was launched.
Though previously published reports have described IQIC’s impact,3 7 their lack of a control (pre-IQIC) period prevents causality inference. These reports also lacked identification of site-specific risk factors contributing to postsurgical morbidity and mortality as well as details of the processes that led to nurse empowerment.
The objective of this paper is to assess the impact participating in the IQIC had on key outcomes after CHD surgery at our institution compared with a control (pre-IQIC) period. Additionally, we identify other risk factors contributing to those outcomes and provide a more detailed presentation of the implementation, including nurse empowerment, at this site.
Methods
Implementation of IQIC guidelines at the Aga Khan University Hospital
Aga Khan University Hospital (AKUH) joined the IQIC in January 2013 and implemented its guidelines to improve CHD surgery outcomes. AKUH is a 644-bed tertiary care teaching hospital in Karachi, Pakistan. A specialised paediatric cardiology department performs around 300 CHD surgeries each year.
Key factors the IQIC identified as having an impact on mortality and morbidity included duration of ventilation and intensive care unit (ICU) stay, rate of postoperative infections, variable adherence to safe perioperative practices and lack of a nurse-empowered, team-based practice. We worked with the following two main approaches to address these issues.
Nurse-empowered team-based approach
The IQIC framework promoted a change in the traditional hierarchical set-up, where nurses played a passive role, by encouraging proactive nurse involvement in patient care and safety. The senior cardiac intensive care unit (CICU) nurse formed and led an ‘IQIC team’ consisting of two paediatric cardiologists, a paediatric cardiothoracic surgeon, anaesthetists and nurses. The chief executive officer of the hospital signed an agreement to join the IQIC, which entailed data entry, regular audits and conducting webinars, thus involving the hospital management in the IQIC process. The nurse acted as a liaison between the hospital administration and the bedside clinical teams, and corresponded with other IQIC sites. She organised monthly educational and training webinars via the IQIC platform, hosted by a multidisciplinary team at Boston Children’s Hospital. She facilitated post-webinar team-based sessions in which participants who had attended the webinar taught those who had missed the session. The active participation of nurses in rounds, assertive communication and better training led to improvement in compliance with patient safety measures. These initiatives placed nurses at the forefront of the only international quality registry at our site, creating a nurse-empowered culture within our wards.
Preventing SSIs and bacterial sepsis
This collaboration stressed the importance of equipment disinfection and hand hygiene to reduce bacterial sepsis and SSI. Measures were taken to improve hand hygiene practices, especially in areas of critical care. Webinars on preventing healthcare-associated infections (HAI) educated healthcare professionals on creating a hand hygiene culture at the hospital. Purell hand sanitisers were installed at entrances to all intensive care areas and adjacent to patient beds. Targets achieved for hand hygiene were displayed prominently at notice boards. Standard barrier precautions including sterile glove and gown use, previously unobserved, were incorporated into echocardiogram procedures. Single-use gels for echocardiograms were distributed and a protocol directing the use of alcohol swabs on echo probes before each use was initiated. A central venous catheter (CVC) care bundle was introduced for drawing blood samples. Safer and more effective methods in the bagging and endotracheal tube suctioning of patients, such as using two people to suction patients, were introduced. Equipment and room disinfectant was changed from 1:30 sodium hypochlorite to 1:3 sodium hypochlorite. The adult and paediatric bays at CICU were separated, and traffic was controlled.
Data collection
All patients undergoing CHD surgeries at our centre between January 2011 and December 2014 were considered for this study. Patients with incomplete records, loss to follow-up within 30 days of surgery or transferred to other facilities postoperatively were excluded. Patient clinical characteristic data were collected preoperatively using standardised forms. Data collected intraoperatively included the surgery performed, its Risk Adjustment for Congenital Heart Surgery (RACHS-1) categorisation,8 and whether the chest remained open postsurgery. Postoperative data included perfusion events, SSIs, duration of ventilation, ICU and hospital stay, and 30-day mortality. Perfusion events encompassed low cardiac output syndrome, acute kidney injury and brain hypoperfusion. SSI was defined using Center for Disease Control definitions.9 Bacterial sepsis was defined as a positive growth of pathogenic bacteria from the blood stream, high-grade fever accompanying an increase or decrease in the white cell count, a rise in C reactive protein, or hypotension, tachypnoea or tachycardia, and if the patient responded favourably to antibiotics. Major infection was defined as either SSI or bacterial sepsis.
Data were primarily collected by the CICU nurse (the IQIC team leader). Two members of the IQIC team (BH and NA) randomly audited 70% of the collected data each month. The IQIC also performed audits. The study was divided into three periods. The period from 1 January 2011 to 31 December 2012 was designated as pre-IQIC, from 1 January 2013 to 31 May 2013 as the transition period and from 1 June 2013 to 31 December 2014 as post-IQIC.
Statistical analysis
Continuous variables were presented as median (25th, 75th percentiles), and categorical variables as count (per cent). Differences in patient characteristics and outcomes between the pre-IQIC and post-IQIC time periods were evaluated using the Mann-Whitney U test and Fisher’s exact test; summaries were included for the transition period for descriptive purposes. Logistic regression analysis was used to further examine factors associated with the outcomes major infection and 30-day mortality. Results were reported as the OR with 95% CIs. Multivariable analysis of baseline patient factors significantly associated with outcomes at the 0.20 level of significance, excluding time period, was performed using forward selection; p values <0.05 were required for retention in the final models. Time period was then introduced into these models to evaluate risk-adjusted relationships with outcomes. C statistics were calculated to assess the discrimination of each multivariable model, and the Hosmer-Lemeshow test was used to evaluate goodness of fit. Associations between major infection, 30-day mortality and additional patient outcomes such as extended ICU length of stay were assessed using Fisher’s exact test. Statistical analyses were performed using SPSS V. 15 and SAS V. 9.4.
Results
A total of 721 patients were included in this study. There was a significant decrease in rates of major infections in the post-IQIC period when compared with pre-IQIC (1% vs 30%, p<0.001) (figure 1) and a trend towards decrease in mortality (figure 2). The duration of ventilation (median 5 hours, IQR 0–19 vs 8 hours, 3–24, p=0.002), ICU stay (48 hours 24–84 vs 52 hours 30–98, p=0.001) and the total duration of hospital stay (5 days, 4–8 vs 6 days, 5–9, p=0.004) were significantly lower in the post-IQIC period compared with pre-IQIC, respectively. This was despite higher rates of open chest postsurgery (5% vs 1%, p=0.004) and patients with major medical illness (5% vs 1%, p<0.001) in the post-IQIC period compared with pre-IQIC (table 1).
Patient characteristics and outcomes across time periods—values shown are median (IQR) or number (per cent)

Interval plots representing six monthly infection rates. The circles represent point estimates and the ends depict 95% CIs. SSI, surgical site infection.

Interval plots representing annual 30-day mortality rate. The circles represent point estimates and the ends depict 95% CIs.
Factors associated with major infections
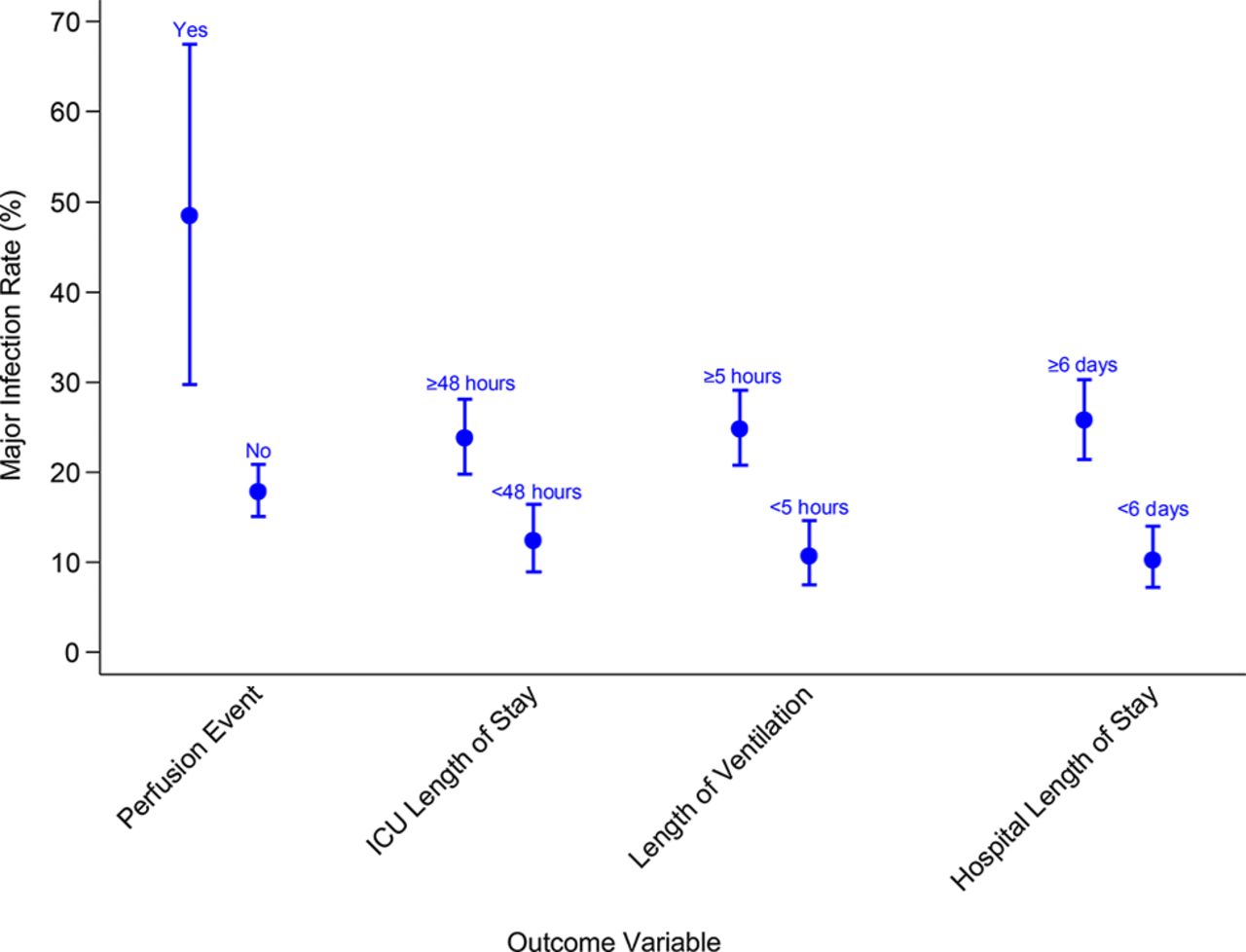
Neonates and infants (OR 3.1, 95% CI (1.6 to 6.2) and OR 2.1, 95% CI (1.4 to 3.2)) had a higher odds of developing major infections postsurgery when compared with patients>1 year of age (p<0.001 for both). Similarly, patients who were malnourished/emaciated (OR 1.6, 95% CI (1.1 to 2.4), p=0.01), with preoperative oxygen saturations of <85% (OR 2.1, 95% CI (1.4 to 3.2), p<0.001) and RACHS risk category of 3–4 (OR 2.4, 95% CI (1.3 to 4.5), p=0.008), had higher odds of developing major infections postsurgery (table 2). Younger age (OR 2.9, 95% CI (1.6 to 6.2), p=0.01 and OR 2.0, 95% CI (1.2 to 3.2), p=0.006 for neonates and infants, respectively) and oxygen saturation <85% remained significantly associated with occurrence of a major infection in multivariable analysis. A higher rate of infection was also seen in patients who had perfusion-related events, ICU stay of ≥48 hours, ventilation of ≥5 hours and hospital stay of ≥6 days (figure 3).
Associations of patient characteristics with major infection and univariate logistic regression models for major infection
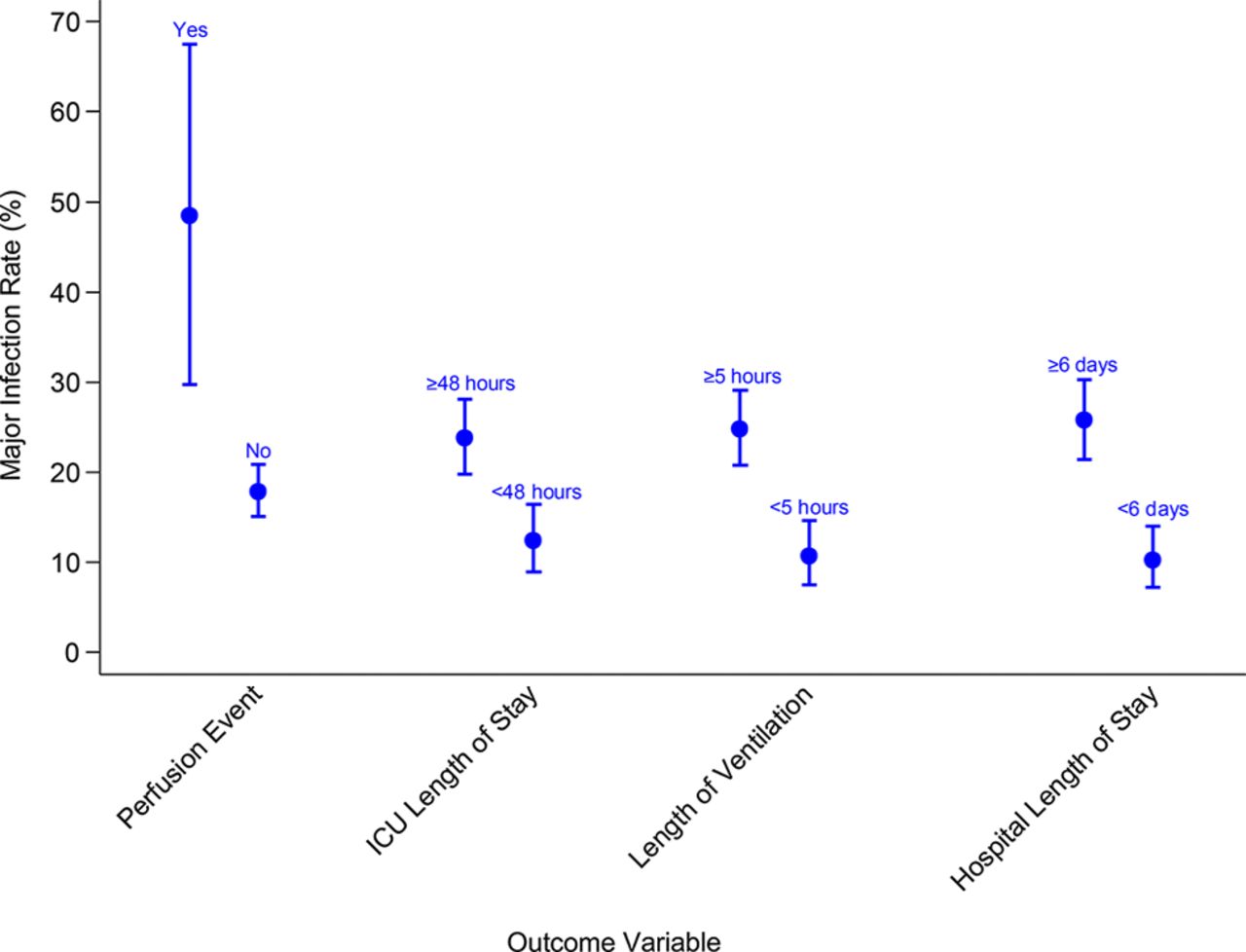
Interval plots representing associations of outcome variables with any major infection. The circles represent point estimates and the ends depict 95% CIs.
The post-IQIC period was associated with lower odds of infection when compared with the pre-IQIC period. This association persisted even after adjusting for baseline patient risk (OR 0.03 95% CI (0.01 to 0.08), p<0.001).
Factors associated with 30-day mortality
Younger age (neonates and infants) at surgery (OR 19.4, 95% CI (8.1 to 46.1) and OR 5.8, 95% CI (2.8 to 11.9), p<0.001 for both), malnourished or emaciated patients (OR 2.2, 95% CI (1.2 to 4.0), p=0.007), patients with major chromosomal anomalies (OR 4.5, 95% CI (1.7 to 11.9), p=0.002) or preoperative oxygen saturations <85% (OR 2.8, 95% CI (1.6 to 5.0), p<0.001) and a RACHS-1 risk category of 3–4 (OR 6.8, 95% CI (3.8 to 12.2), p<0.001) were associated with a higher odds of mortality (table 3). Younger age (OR 11.5, 95% CI (4.4 to 30.1) and OR 4.2, 95% CI (2.0 to 9.0) for neonates and infants, respectively, with p<0.001 for both), nutritional status malnourished or emaciated (OR 2.9, 95% CI (1.5 to 5.7), p=0.003) and risk category 3–4 (OR 5.4, 95% CI (2.8 to 10.4), p<0.001) remained significantly associated with occurrence of 30-day mortality in multivariable analysis (table 4).
Associations of patient characteristics with 30-day mortality and univariate logistic regression models for 30-day mortality
Multivariable models for major infection and 30-day mortality
Patients with an open chest postsurgery, perfusion-related events, ventilation ≥5 hours, ICU stay ≥48 hours and those who acquired a major infection had a higher rate of mortality (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Interval plots representing associations of outcome variables with 30-day mortality. The circles represent point estimates and the ends depict 95% CIs.
Adjusting for baseline patient risk, the time period was not significantly associated with mortality. However, the odds of death in the post-IQIC period were lower than in the pre-IQIC period (OR 0.8, 95% CI (0.4 to 1.7), p=0.63).
Again adjusting for baseline patient risk, major infections did not significantly increase the risk of death. However, the OR was greater than 1 (OR 1.6, 95% CI (0.8 to 3.0), p=0.20) and inclusion of major infection did increase the model discrimination slightly (c statistic from 0.844 to 0.854).
Discussion
By adopting clinical practice measures via the IQIC platform, we demonstrated a significant decrease in morbidity and a statistically insignificant decrease in mortality. There was also a substantial decrease in duration of ventilation and length of ICU and hospital stay in the post-IQIC period. Similar benefits have been demonstrated by other IQIC centres.7 We identified patients who were younger than 1 year of age at surgery, malnourished or emaciated, who had preoperative oxygen perfusion <85%, perfusion-related events, RACHS-1 3 or 4, open chest after operation and increased durations of ventilation, ICU and hospital stays as being at a higher risk of both morbidity (major infections) and mortality post-CHD surgery.
The IQIC identified team-based practice through nurse empowerment as a strategy for reducing morbidity and mortality.3 Our use of the term empowerment is informed by Kanter’s theory of empowerment, which has widely been applied to the practice of professional nursing. This theory asserts that empowerment is promoted in work environments that provide employees with access to information, resources, support and opportunities for professional growth.10 11 Empowered nurses have better job satisfaction, are more accountable for their work and more committed to the organisation. Studies have identified workplace empowerment as a strong predictor of job satisfaction.11 Improved job satisfaction reduces turnover rates, which have been associated with poor patient care quality and outcomes. Empowering nurses through IQIC puts them in a position to have an impact on healthcare policies within the hospital and produces better infection control practices. This was illustrated in instances of compromised sterility when nurses were encouraged to speak up and promote hand hygiene. Low/middle-income countries face educational and cultural barriers that preclude nurses from communicating effectively. Such barriers include a lack of nurse involvement in patient management, inadequate communication training and hierarchy within the medical team discouraging expression of concern or opinions.12 Giving the CICU nurse a lead position and making her the liaison between the clinical team and this hospital’s leadership was pivotal in achieving empowerment at our institution. A dedicated IQIC team, led by her, improved communication and effectively implemented quality measures.
Morbidity (postoperative infections)
Measures effective in reducing postoperative infections (SSI and bacterial sepsis) include the use of CVC bundles and good hand hygiene practice.13 14 The spread of infections by hands from health workers is the most common iatrogenic factor causing HAI in neonates.15 However, poor compliance rates in low-resource settings lead to a burden of HAI that is substantially higher than in developed countries.16 This disparity may also be attributed to contamination of catheter insertion sites, resulting in central line-associated bloodstream infections (CLABSI). Employing CVC bundles have shown to significantly reduce CLABSI rates.17 The introduction of a hand hygiene policy and a CVC care bundle in our centre contributed to a 71% decrease in postoperative infections during the IQIC period. Monthly internal infection control audits reported that hand hygiene compliance throughout all critical care areas at our centre increased from 45% to 75% (p=0.02) (see online supplementary figure S1). According to the 2014 IQIC report, a yearly benchmarking report tracking the progress of all institutions participating in the IQIC, the infection rate at our centre was well below the aggregate average.
![[SP1.jpg]](https://heart.bmj.com/content/heartjnl/103/21/1680/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
As identified by others,18 19 age <1 year at surgery, low preoperative oxygen saturations, high RACHS-1 score, perfusion-related events and long duration of ventilation, CICU and hospital stay were found to be risk factors for postoperative infections at our centre. In low/middle-income countries, identification of patients with such risk factors can lead to improved and more efficient resource allocation (eg, isolated rooms and one-to-one nursing).
Mortality
A decreasing trend in mortality during the post-IQIC period was observed at our centre. Developing a postoperative infection increased odds of mortality in our cohort. Postoperative infection is an established risk factor for mortality.20 21 Reduced infections may have contributed to the decreasing trend in mortality. However, mortality at our centre remained higher than the IQIC standardised institutional mortality rate. As demonstrated by other studies,22 23 risk factors like infant age at surgery, a higher RACHS-1 risk score, presence of major chromosomal anomalies, lower preoperative saturations, perfusion-related events, an open chest postsurgery and longer duration of ventilation and ICU stay were also associated with higher mortality in our patients. Measures to address some of these factors (eg, development of surgical expertise, improvement of infection control in high-risk patients) may help further decrease the mortality at our centre.
Malnutrition was identified as a risk factor for mortality in our cohort. Since 95% of the world’s malnourished live in low/middle-income countries,24 congenital heart programmes in resource-limited settings must recognise the impact malnutrition can have on the programme’s outcomes. Optimisation of nutritional intervention before and after surgical correction and standardisation of feeding protocols is vital to achieve the best postoperative care.25 Nurses empowered through the IQIC programme have initiated a nutritional intervention quality improvement initiative following the identification of this risk factor. Such interventions may help further improve the outcomes of CHD surgical programmes in low/middle-income countries.
Limitations
During the first quarter of the postintervention period, a steep learning curve for nurses and other CICU staff may have prevented adequate implementation of IQIC policies. The transition period served to address this issue. Variables were collected using standardised IQIC forms. Thus, other patient confounders may not have been accounted for. As a single centre study, the generalisability of our results is limited to our locale and similar resource-limited settings. Since our centre primarily employed one cardiothoracic surgeon, his expertise and experience with the surgeries increased with time, which may have favourably impacted the results of this study.
Conclusion
Participation in the IQIC coincided with a substantial decrease in bacterial sepsis and SSIs and a trend towards decrease in mortality. Results suggest that the IQIC model of nurse empowered/led, team-based practice along with basic infection control practices inculcated through continuous education reduced bacterial sepsis and SSIs. This improves outcomes of congenital heart surgeries in low/middle-income countries.
Key messages
What is already known on this subject?
The International Quality Improvement Collaborative (IQIC) uses a registry and quality improvement strategies to reduce mortality and morbidity associated with congenital heart disease surgeries in low/middle-income countries.
What might this study add?
Using a control period (pre-IQIC), we demonstrate a decrease in the postoperative infection rates from 30% to 1% and mortality from 9% to 6% after joining IQIC. We also identify additional important risk factors of surgical mortality, that is, malnutrition and describe process measures that led to nurse empowerment.
How might this impact on clinical practice?
Low/middle-income countries should implement IQIC protocols and use the IQIC framework to identify site-specific risk factors for poor surgical outcomes. Empowering nurses with leadership responsibilities and a team-based practice encourages nurse-led quality improvement initiatives for site-specific risk factors.
References
Footnotes
Contributors AK, BH and AA have contributed equally to the study concept, designing, data collection, analysis and manuscript writing. HA contributed to the data collection, analysis, manuscript writing and revision. KG, AR and SB contributed to the data analysis and manuscript writing. KJJ contributed to the study concept, design, analysis and manuscript writing. MA, AH and FM contributed to the conception, study design, patient selection, manuscript editing and final approval of the study. NA contributed to the data entry, data validation, concept, patient selection and manuscript editing.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.