Article Text

Abstract
It is vital to involve children, young people and families in the design, delivery and improvement of their care. Their involvement can range from individuals giving feedback, such as patient stories, to collaborative work including patient groups and communities helping to develop and commission services. The methods for involving individuals and families include questionnaires and innovative ideas such as feedback Apps. Other methods include the 15 Steps Challenge which helps an organisation to view the care it delivers through a patients eyes and includes a ‘walk around’ involving a patient, carer, staff member and board member. The Experience Based Design approach is another method of reviewing a service and involves assessing how staff and patients feel when delivering and receiving care. Involving patient groups can be facilitated by working with schools and children's centres. The type of involvement will vary, but if carefully designed can allow meaningful participation and improvement of services.
- Quality Improvement
- Patient Involvement
- Patient Experience
- Feedback
Statistics from Altmetric.com
Introduction
Children, young people and families who access health services form an important quality improvement tool. Our use of their huge expertise varies significantly, but even short reflection on their unique window of experience tells us something profound, for example, feedback from an 11-year-old who described ‘I felt really scared’ at an experience of being surrounded by drunken adults in an emergency department. If we take up the mantra ‘No decision about me without me’1 then we must involve children, young people and families in the design, delivery and continuous improvement of their care.
This article, as part of the series on quality improvement in child health, will act as a guide for health professionals who provide care and design services for and with children and young people, allowing them to assess patient experience and embed the views of children, young people and families into everything that they do.
Children, young people and families must be involved in the design and delivery of their care. There must be real involvement of patients and the public in all that is done, and patients should be integrated into organisational structure at both provider and commissioner levels.2
The continuum of patient influence is least developed through patients complaining, but then develops through listening and responding, and then consulting and advising, but finally progresses to co-designing services with patients.3
Whether focussing on improvement in individual programmes of care, or whole system large-scale change, the gold standard for all patient experience and engagement work is experience-based co-design. It is necessary to acknowledge from the outset what the aims of the service improvement work are and how partnership with children, young people and families can be used to improve outcomes.
Who should be involved – individuals, groups or communities?
The level of patient involvement that is appropriate can range from working with a specific individual to whole communities as illustrated in figure 2. At the individual level, the emphasis should be on gathering specific feedback including patient stories, positive or negative, relating to their unique experience. This can then be themed for ongoing service improvement work. On a larger scale, collaborative work with expert patient groups may be appropriate for development and commissioning of services or recruitment of staff. At a still larger scale, engagement with communities may allow children and young people to be involved in, for example, reconfiguration of services, in schools or beyond.
Spending time exploring and planning patient involvement at the outset of a service improvement project will be time well spent. The methods of capturing experiences will vary depending on each situation, to ensure that rich feedback is effectively gathered to enhance the delivery of care and to achieve better outcomes for children, young people and their families.
Guidance on designing a project to assess and improve patient experience is available from the Royal College of Paediatrics and Child Health in the document ‘Not just a phase: A Guide to the Participation of Children and Young People in Health Services, 2010’. This document provides a useful framework for planning a participation project (box 1).
Box 1 Planning a participation project
There are a number of key steps in planning a participation project, and young people should be involved in this planning process.
-
Be clear about the aims and objectives and take into account what resources you have available.
-
Be clear about the degree of participation and how decision making will (or can) be shared with young people.
-
Be realistic about the extent to which change is possible.
-
Consider who you will invite to participate. Is your group representative of current or potential service users? Have you included children from marginalised groups, for example, looked after children, black and minority ethnic children and children with disabilities?
-
Which methods of participation would best suit the aims and objectives, resources and participants? It is preferable to employ a variety of methods and to involve young people in the methods to be used.
-
Draw up an ethical statement, clarifying issues around consent (by children/parents), confidentiality, anonymity and disclosure.
-
Consider developing a contract of participation. Will it include rewards for young people who participate?
-
Plan which staff you will be using as facilitators and ensure they have the necessary skills.
-
Consider the practicalities – what potential obstacles are there to completing the project?
There are various methods of assessing patient experience with varying levels of qualitative and quantitative information with varying levels of patient involvement required. Current or recent data, collected through a variety of methods to allow triangulation of data, are most useful. Qualitative and quantitative data are both important, including patient stories, with comparison of data before and after interventions and across different clinical settings.4
Resources and examples of patient experience and patient participation tools
There are many methods by which children, young people and families can be actively engaged in sharing their experiences to enhance services.
Some ideas as to how children and young people can engage and participate in health services
-
Provision of direct feedback via a compliment letter, complaint, survey, either in writing, online or via Apps
-
Engagement in expert patient programmes
-
Reviewing current healthcare services using programmes such as the Department of Health's You're Welcome Standards and the NHS Institute 15 Steps Programme
-
Recruitment and selection of staff
-
Informing and participating in research programmes
-
Participation in the governance of health services
-
Involvement in the commissioning of services
Tailoring each patient experience and engagement activity to the project is essential to ensure that it is appealing to children, young people and families, allowing meaningful feedback. Each method, from surveys and questionnaires to focus groups, has advantages and disadvantages which should be considered. It is also important that feedback is provided to children, young people and families, so that they know their input has been valued and that their feedback has made change possible.
The following resources and examples offer some inspiration that can be built on and developed locally.
Patient questionnaires for children seen in urgent and emergency care
Questionnaires are a convenient way to capture feedback and can be applied to any setting, such as outpatients and inpatient experiences. The Royal College of Paediatrics and Child Health developed a survey to measure patient-reported outcome measures for children seen in urgent and emergency care which can be used to capture the experiences of using ambulance, GP or emergency department/walk-in centre services. This questionnaire was based on literature review, then developed through focus groups with children and families, allowing incorporation of the views of children and families at an early stage. The questionnaire has different versions; for parents and carers, for 0–7-year-olds and for 8–16-year-olds. The capturing of feedback from children and young people in these settings has not been systematically gathered, but these questionnaires will allow themes to be identified to provide a focus for service improvement programmes.5
Using social media to obtain contemporary feedback regarding patient experiences
The growth of social media cannot be ignored in capturing patient experience.
Birmingham Children's Hospital has developed a feedback App as part of their commitment to providing open and transparent services. Children, young people and families can download the App, and all messages are published live on their website, providing a real-time view of their services as seen by patients and families. www.feedbackapp.nhslocal.nhs.uk
Some trusts now have age-appropriate websites, for example, Imperial Children's Hospital http://www.imperial.nhs.uk/cyp/index.html and University College London NHS Foundation Trust http://www.childrenandyoungpatients.uclh.nhs.uk/ and patient experience can be captured via this source.
Low-cost ideas
Resources are often limited, but easily implemented engagement mechanisms are available that do not require significant investment, such as those used by West Suffolk NHS Foundation Trust as shown in figure 1. Taking the learning from a local supermarket they gathered the tops of plastic milk cartons (too big for children to choke on!) and asked children to select which large plastic cereal box they put them in based on their experiences, the boxes have ‘happy’, ‘ok’ and ‘sad’ faces. An early warning sign is if there are a few in the sad box and immediate investigations and actions can begin (figure 1).

Feedback boxes at West Suffolk NHS Foundation Trust.
At University Hospital Southampton NHS Foundation Trust, the paediatric matron worked with play specialists to encourage children and young people to become ‘secret agents’, collecting evidence in their note books, providing insight and feedback into their experience. The play specialists also have access to digital cameras, and support children and young people to take pictures, while ensuring consent and confidentiality issues are addressed.
15 Steps Challenge
The 15 Steps Challenge was inspired by a quote from a parent: “I can tell what kind of care my daughter is going to get within 15 steps of walking on to a ward”. The challenge was developed by the NHS Institute and provides a tool for organisations to work with staff, patients and other stakeholders to view a clinical setting through a patient's eyes. An important stage in the challenge is a ‘walkaround’ by a team made up of a patient or carer, staff member and board member. The purpose of the ‘walkaround’ is to recognise what the patient sees and to make note of their first impression. The team then feeds back to senior leaders in the organisation, with a focus on good practice and areas for improvement. It is most useful if this is repeated at regular intervals to monitor whether improvements are being made.
A free toolkit is available at www.institute.nhs.uk/productives/15StepsChallenge and has been specifically developed for children and young people to participate in the challenge (figure 2).6

Graphic representation of the 15 Steps Challenge.
Experience-based design approach
The experience-based design (EBD) approach is a tool for surveying patient and staff emotions and feelings related to receiving and delivering care. Staff and patients look together at how to improve how care is delivered at each stage of the patient journey. This approach focuses more on a patient's experience of their journey, encouraging patients to tell their stories, and looking for ‘touchpoints’ where their experience is most powerfully affected. Patients and staff are then involved to shape systems and processes, with a focus on patient experience.7
Working with communities
Engagement with children, young people and families has identified that schools are an ideal location to capture feedback about experiences and ideas for improvement regarding health services.
The NHS Institute for Innovation and Improvement has coproduced emergency and urgent care lesson plans and suites of resources for 5–11-year-olds and 11–14-year-olds to support health and education in embedding information about health in schools. Structured resources, such as these, introduce children to language of healthcare, local services and mechanisms for providing feedback about their experiences, while within a familiar environment. Demonstrable benefits of close collaboration include the development of high-quality signposting information to children and families, in school diaries, which highlight the range of services available to families.8
Working with children's centres
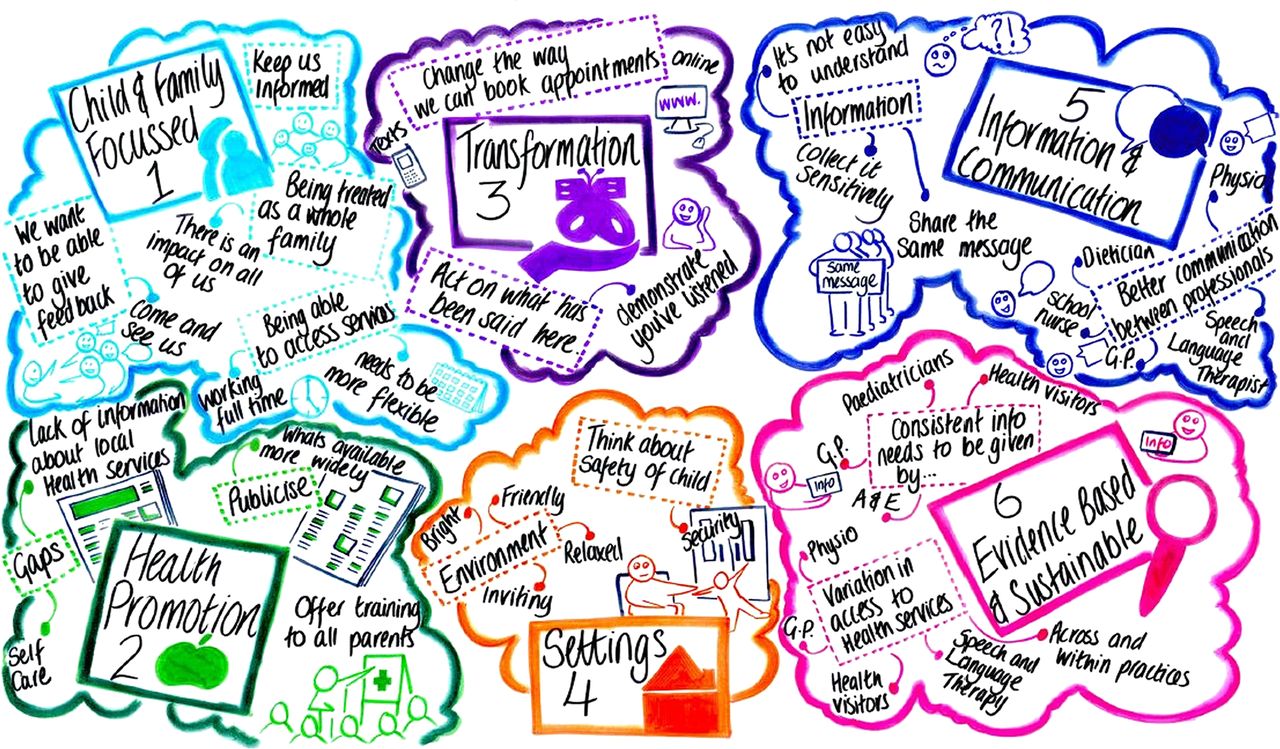
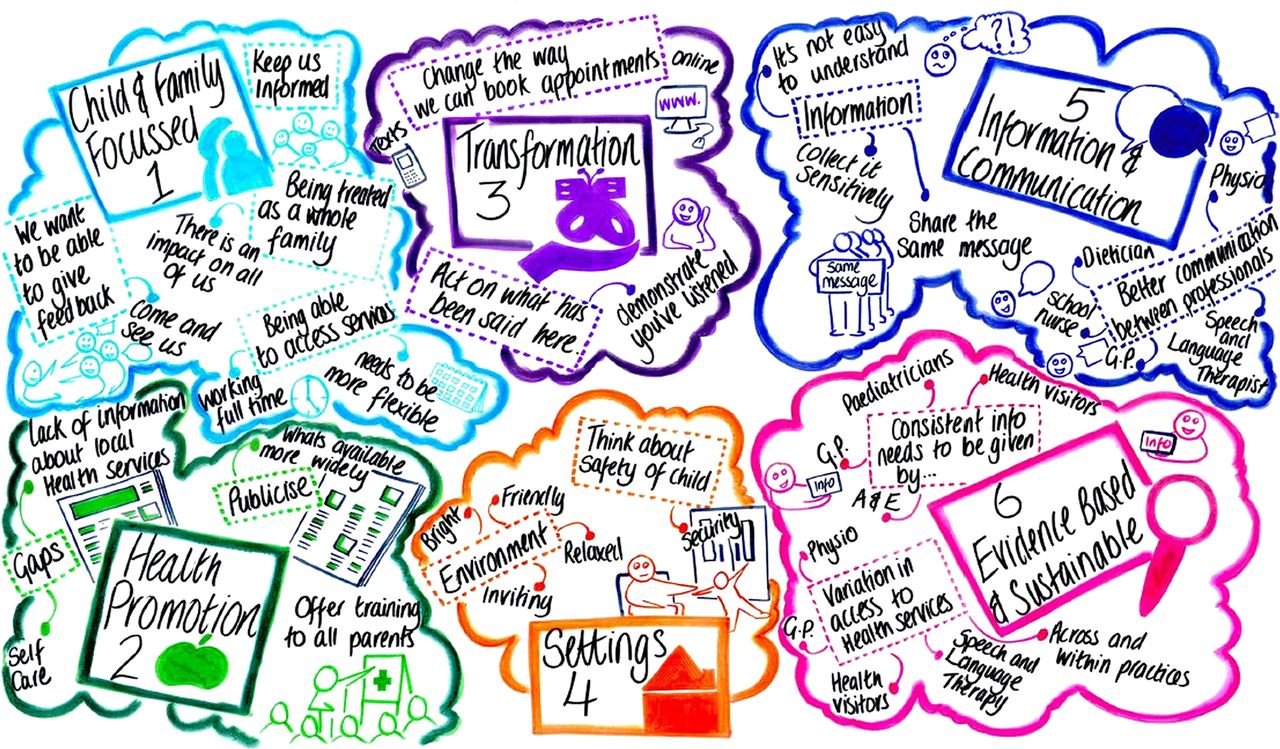
In East of England a multiprofessional team including patient and family representatives developed a vision and defined principles to help providers of healthcare for children and young people and commissioners to define what good care looks like. These principles give providers and commissioners a tool by which to assess care and look at ways to improve care. The principles can be used in any setting where children and young people are seen from GP surgeries to hospitals or even minor injury units. As part of the work, the team also visited children's centres, primary and secondary schools and listened to stories of families’ experiences of local health services. Children, young people and families offered plenty of ideas about how we could enhance services. The use of graphic facilitation captured ideas in real time, demonstrating that all contributions were valued. The result was a postcard that children, young people and families can use to hold their local health services to account (figure 3).
{kind=link}
{kind=link}
{kind=link}
A graphic representation developed in East of England to illustrate what children, young people and families want from health services.
Conclusion
Children and young people are key stakeholders in health and healthcare, rather than beneficiaries or passive recipients of services. If health services are to deliver high-quality holistic care, then the experiences of children and young people need to be harvested, valued and acted on. As health professionals, it is our responsibility to create the mechanisms to facilitate effective engagement of children and young people who are current and future consumers of healthcare, to cultivate true participation and coproduction. Children and young people's engagement and involvement will result in much richer perspectives that will assist in improved health outcomes and enhanced services.
Footnotes
-
Contributors SR and KP had the idea for the article. SR performed the literature search. SR wrote the article with contributions from KP and KE. SR is the guarantor.
-
Competing interests None.
-
Provenance and peer review Commissioned; internally peer reviewed.