Article Text

Abstract
Since the 2010 publication in this journal of a review of the management of imported malaria for UK children, new evidence for the treatment of both severe and uncomplicated malaria has been published. This review discusses these new data and expands the scope of the previous review to include non-endemic countries outside of the UK. The results of the AQUAMAT trial in late 2010 and other studies have prompted the WHO to recommend that intravenous artesunate be used preferentially over quinine for the treatment of severe malaria caused by any Plasmodium species in both adults and children. Oral artemisinin-based combination therapies have also shown equivalent (if not better) efficacy in the treatment of uncomplicated malaria caused by all Plasmodium species (including chloroquine-resistant P vivax) in both adults and children, though there are issues regarding the availability of artemisinin-based combination therapies in many non-endemic countries. In these instances, conventional therapeutic regimens continue to be efficacious. Lastly, the use of primaquine for hypnozoite and gametocyte eradication is discussed.
- Infectious Diseases
- Tropical Inf Dis
- Tropical Paediatrics
- Pharmacology
- General Paediatrics
Statistics from Altmetric.com
Malaria in humans is caused by the transmission of the Plasmodium parasite via infected bites from female Anopheles mosquitoes. The main species known to infect humans are P falciparum, P vivax, P malariae, and P ovale. P knowlesi, first recognised as a primate infection in Southeast Asia, has increasingly been described in human infection, including children.1 Severe malaria is largely caused by P falciparum, though other species (particularly P vivax) may also cause serious illness.2–6
Approximately half of the global population lives in a malaria-endemic region. An estimated 216 million clinical cases and 655 000 malaria deaths occurred in 2010, predominantly in children aged <5 years in sub-Saharan Africa.7
In non-endemic countries, most patients presenting with malaria are returned travellers who have visited endemic regions. However, the recent increase in global migration has resulted in a growing proportion of patients who originate from endemic regions (ie, immigrants or refugees) and/or those visiting friends and relatives (VFRs) in these regions; this latter group, in particular, has low uptake of antimalarial chemoprophylaxis and other preventative measures.8 ,9
In the UK from 2005 to 2010, there were approximately 1600 cases of imported malaria each year, of which 10–15% of cases were in children.9 ,10 Of childhood cases, 90% were among African children who acquired their infection in Africa as VFRs. Most cases (∼80%) were falciparum malaria.9 ,10 The USA has a similar epidemiology—approximately 1500 cases annually, of which 15–20% are children and 70% are among VFRs.8 In Australia, the age profile is similar, but the number of cases of imported malaria halved from 800 in 2005 to 400 in 2011,11 in part due to improved pre-departure screening and management of malaria in humanitarian refugees.
An overview of the clinical presentation, diagnosis and management of imported malaria in children in the UK was recently published in this journal.10 Here we have updated the information on treatment of malaria in children, following the publication of key new evidence.
Severe malaria—the increasing use of intravenous artesunate
Refer to figure 1 for the definitions of severe and uncomplicated malaria.

Initial management of malaria.
The choice of therapy for both uncomplicated and severe malaria (figure 1) has evolved rapidly over the past decade with the introduction of artemisinin derivatives (table 1). Early research in the 1980s and early 1990s, using predominantly intramuscular artemether (or intramuscular artemotil (arteether)), showed no overall survival benefit over quinine in the treatment of severe falciparum malaria in children.10 Artemether in particular is known to have erratic and partial absorption especially in severely ill patients.14
More recent research using parenteral artesunate has shown it to be rapidly and reliably distributed,14 ,15 and highly efficacious for the treatment of severe malaria due to all Plasmodium species. The 2005 SEAQUAMAT study, a large well-designed study of 1461 Southeast Asian patients (including 202 children) with severe falciparum malaria, directly compared mortality outcomes in those treated with intravenous artesunate versus quinine.16 The trial was stopped prematurely due to the clear survival advantage of artesunate in adults (relative risk (RR), 0.69; 95% CI 0.54 to 0.83; risk reduction 34.7%). However the study was relatively underpowered for these findings to be generalised to the paediatric population.
The subsequent AQUAMAT trial in 2010 confirmed these (Asian) adult findings in a trial of African children; 5425 children from nine African countries were enrolled. There was a 22.5% reduction in mortality in patients receiving intravenous artesunate compared with quinine for severe falciparum malaria (OR, 0.75; 95% CI 0.63 to 0.90), together with a significant reduction in clinical complications (development of coma, convulsions and deterioration of coma score).17
The first WHO Guidelines for the Treatment of Malaria (2006) recommended either parenteral artesunate or quinine as acceptable therapies for severe falciparum malaria in both adults and children.13 SEAQUAMAT, AQUAMAT and other similar clinical trials (recently summarised in a Cochrane review18) have led to a change in the WHO guidelines such that intravenous artesunate be used preferentially over quinine as the drug of choice in both adults and children with severe falciparum malaria13 (figure 1 and table 2).
While P falciparum is the most important species causing severe malaria, other Plasmodium species can also cause severe disease. Recent literature has highlighted severe P vivax malaria in both adults and children. Previously considered relatively benign compared with P falciparum, infections with P vivax are associated with severe anaemia, acute respiratory distress syndrome and higher mortality than realised previously.2–5 Interestingly, the predilection of P vivax to infect young red blood cells (reticulocytes) severely limits its reproductive capacity; levels of P vivax parasitaemia rarely exceeds 2% and high parasitic burdens are not characteristic of severe disease.2 ,4 ,5 Rather, the severity of P vivax infection is thought to result from proinflammatory cytokines.2 ,5 Much less is known about the pathophysiology of severe P knowlesi infection; it causes a similar clinical spectrum to P falciparum, but without coma.1 ,6
There are no studies that directly compare the efficacy of intravenous artesunate to quinine for severe malaria caused by non-falciparum species.3 ,4 However, artemisinins have demonstrated higher activity against P vivax than P falciparum, and faster parasitic clearance times against P vivax than chloroquine or quinine.23 The clinical success of artesunate has been also well-documented in multiple case-series of severe vivax3 ,4 and knowlesi6 malaria in both children and adults. Given this evidence and its proven superiority in falciparum malaria, parenteral artesunate is now recommended as the first-line treatment for all cases of severe malaria regardless of the causative species.13 Furthermore, intravenous artesunate should also be used whenever oral therapy is not tolerated (figure 1 and table 2).
The accessibility of intravenous artesunate in both resource-rich and resource-poor countries has been an issue, but the situation is improving. It remains unlicensed for the treatment of severe falciparum malaria in the UK, European Union, USA and Australia because the only commercially available product (Guilin Pharmaceutical Company, China) is not manufactured according to international Good Manufacturing Practice standards. However, intravenous artesunate from the Guilin company achieved WHO prequalification status in November 2010, which may facilitate its formal acceptance into standard drug formularies. In the UK, artesunate is accessed on a ‘named patient basis’ and is available via the two schools of tropical medicine (Liverpool and London).22 In the USA, the use of artesunate falls under an ‘investigational new drug’ protocol and it is only obtainable through the Centres for Disease Control and Prevention.19 In Australia, intravenous artesunate is widely available in hospitals through the national ‘Special Access Scheme’; a similar scheme has been established in Canada via the Canadian Malaria Network. The accessibility of intravenous artesunate in other countries varies widely.
Uncomplicated malaria
For the treatment of uncomplicated falciparum malaria, oral artemisinin-based combination therapies (ACTs) exhibit at least equal efficacy to non-artemisinin-based regimens for both adults and children,24 and have been the treatment of choice since the 2006 WHO treatment guidelines. Artemether plus lumefantrine (Coartem or Riamet) is the ACT most commonly used by global malaria eradication programmes and is widely distributed in under-resourced countries. However, Coartem/Riamet and other ACTs are not readily available in Canada, UK and parts of Europe, due to licensing and quality assurance issues similar to those encountered by intravenous artesunate. UK and Canadian national guidelines recommend atovaquone plus proguanil (Malarone) or quinine sulphate plus doxycycline/clindamycin as effective alternative treatment regimens21 ,22 (figure 1 and table 3).
Treatment recommendations for non-falciparum malaria are changing rapidly with the patchy but increasing availability of ACTs, decreasing access to chloroquine, and most importantly, the increasing prevalence of chloroquine-resistant strains of P vivax worldwide. The 2010 WHO treatment guideline continues to recommend chloroquine as the primary treatment for all uncomplicated non-falciparum malaria (P vivax, P ovale, P malariae and P knowlesi) with the exception of vivax malaria from known chloroquine-resistant areas.13 However chloroquine-resistant P vivax (once thought to be limited to Indonesia, Timor-Leste and the Pacific Islands) is now widely distributed throughout Southeast Asia and has been increasingly reported in India, parts of Africa (Ethiopia, Eritrea, Madagascar), Turkey and South America, with chloroquine treatment failure rates reported to be over 10%.4 ,5 ,25 ,26 This significantly undermines the clinical utility of chloroquine; it is likely to be obsolete in a few years’ time.25
As a result, ACTs are increasingly used in all non-falciparum malaria, and are currently recommended by WHO as an alternative to chloroquine for chloroquine-sensitive species (figure 1 and table 3). In a Cochrane systematic review comparing the efficacy of ACTs versus chloroquine for chloroquine-sensitive vivax malaria in both children and adults, ACTs demonstrated lower rates of remaining parasitaemia at 24 h (3 trials, 1165 participants; RR, 0.39; 95% CI 0.31 to 0.48) and equivalent treatment efficacy as measured by recurrent parasitaemia before day 28 (4 trials, 1185 participants; RR, 1.0; 95% CI 0.8 to 3.39).27 In addition, ACTs with long half-lives (particularly dihydroartemisinin-piperaquine) were demonstrated as probably superior to chloroquine over 6–8 weeks follow-up, with significantly fewer recurrent episodes after day 28 (2 trials, 668 participants; RR, 0.47; 95% CI 0.29 to 0.76).27 Two other thorough literature reviews elaborate further on this evidence with an additional eight studies which had not been included in the systematic review.4 ,25 Lastly, one review examined specifically the efficacy of artemether-lumefantrine (the most widely available ACT) for vivax malaria,26 and summarised that lumefantrine's relatively short half-life translated to a lower day 28 parasitological cure rate compared with some other ACTs or chloroquine-primaquine when given alone, but had similar efficacy to chloroquine-primaquine when it was also given with primaquine.
In patients with likely chloroquine-resistant vivax malaria, ACTs are also the treatment of choice according to WHO treatment guidelines (figure 1 and table 3). However, atovaquone plus proguanil (Malarone) and mefloquine continue to have excellent efficacy,4 ,5 and are the recommended alternatives (along with quinine sulphate plus doxycycline/clindamycin) when ACTs are not available (figure 1 and table 3). Eventually, given their effectiveness against all Plasmodium species and for ease of protocol, ACTs are likely to become the universal treatment for uncomplicated malaria as the availability of ACTs in both resource-rich and under-resourced countries improves.25–27
Unfortunately, resistance of falciparum malaria to artemisinins has started to emerge in areas along both the Thai-Cambodian and Thai-Myanmar borders, as seen by increasing parasitic clearance times and rising treatment failure rates.28 ,29 Day 42 treatment efficacy rates are now estimated to have decreased from nearly 100% to 75–90% in western Thailand,29 and the prevalence of impaired artemisinin efficacy may be as high as 30–40% in western Cambodia.28 ,29 Despite the introduction of ACTs a decade ago in Cambodia, monotherapy artemisinin use is the most common.28 As artemisinins are still the most effective compounds available in these areas, they are still considered the treatment of choice if coupled with a partner drug, while containment measures that limit the spread of resistant strains continue to be implemented.
Primaquine therapy for liver hypnozoite and gametocyte eradication
In children infected with P vivax, P ovale, or an infection (including mixed infection with more than one species) where P vivax or P ovale cannot be reliably excluded, a 14-day course of primaquine is necessary to eliminate hypnozoite forms dormant in the liver13 ,20–22 to prevent relapse months to years later. Screening for glucose-6-phosphate dehydrogenase (G6PD) deficiency should be performed prior to the administration of primaquine and advice sought from paediatric infectious disease specialists should the patient be G6PD deficient. For those without G6PD deficiency, the antihypnozoite primaquine dose varies with species; a dose of 0.25 mg/kg daily is adequate for P ovale infections, whereas 0.5 mg/kg daily is recommended in P vivax infections (or infection with unknown species) due to the increasing resistance to primaquine primarily in Southeast Asia (table 4). Patients with a mild variant of G6PD deficiency (see footnote of table 4 for G6PD variant classification) may be treated with a less-intensive and prolonged course of primaquine under close supervision of a paediatric infectious disease specialist, using a dose of 0.75 mg/kg weekly for 8 weeks.13 ,19 ,21 ,22 ,30 The patient should be monitored closely, and if signs of haemolysis occur (eg, jaundice, darkened urine) the medication should be stopped.
In addition, it is useful to consider whether therapy against gametocytes (the sexual stage of the parasite transmitted to mosquitoes from infected patients) should be administered, especially in places with Anopheles mosquitoes but without endemic malaria, where imported cases may lead to local outbreaks. In the past decade there have been a handful of examples of imported cases leading to local transmission of either P falciparum or P vivax in France, Greece, Italy, Spain, the USA (Florida), Jamaica, the Bahamas, Singapore and Oman.7 These instances usually result in small outbreaks of less than 10 cases, although in one exceptional situation a wave of immigration to Jamaica between 2006 and 2009 resulted in 406 confirmed local cases of P falciparum malaria.7
Primaquine is the only antimalarial that is effective against all stages (including mature) gametocytes; artemisinins (and to a lesser extent sulfadoxine-pyrimethamine, amodiaquine and chloroquine) target only early-stage (but not mature) gametocytes.31 Therefore, although not suggested on a routine basis, for those patients living in areas at risk of ongoing malaria transmission, the administration of a single dose of primaquine (after checking G6PD status) should be considered for adults and children ≥1 year of age who are infected with P falciparum or P malariae (there is no evidence to date of human-to-human transmission of the zoonotic P knowlesi), in addition to the primary antimalarial therapy;13 ,31 primaquine therapy for liver hypnozoites will adequately treat gametocytes in those infected with P vivax, P ovale or an unknown species (see above).
Outpatient management
Previous guidelines for non-endemic countries suggest that all patients with falciparum malaria should be hospitalised for observation and initial treatment.20–22 However, routine admission may not always be necessary and most children in resource-poor countries are managed in the outpatient setting (often not even by a medical doctor). As stated previously, an increasing proportion of imported malaria cases are attributed to recent migrants/refugees and VFRs. These patients may have a degree of antimalarial immunity, conferring some protection from the more severe manifestations of disease. A recent systematic review summarises the results of five studies (four in adults, one in children) in which patients with uncomplicated falciparum malaria were successfully managed in an outpatient setting.32 Three studies involved only immigrant/refugee populations while two studies included travellers/expatriates with imported malaria. In all studies, approximately 40–75% (62% in the study involving children)33 of patients with falciparum malaria were successfully treated in the ambulatory setting. The selection criteria for outpatient management were similar: clinically well without clinical or laboratory features of severe malaria, low level of parasitaemia, and reliable follow-up and family support.
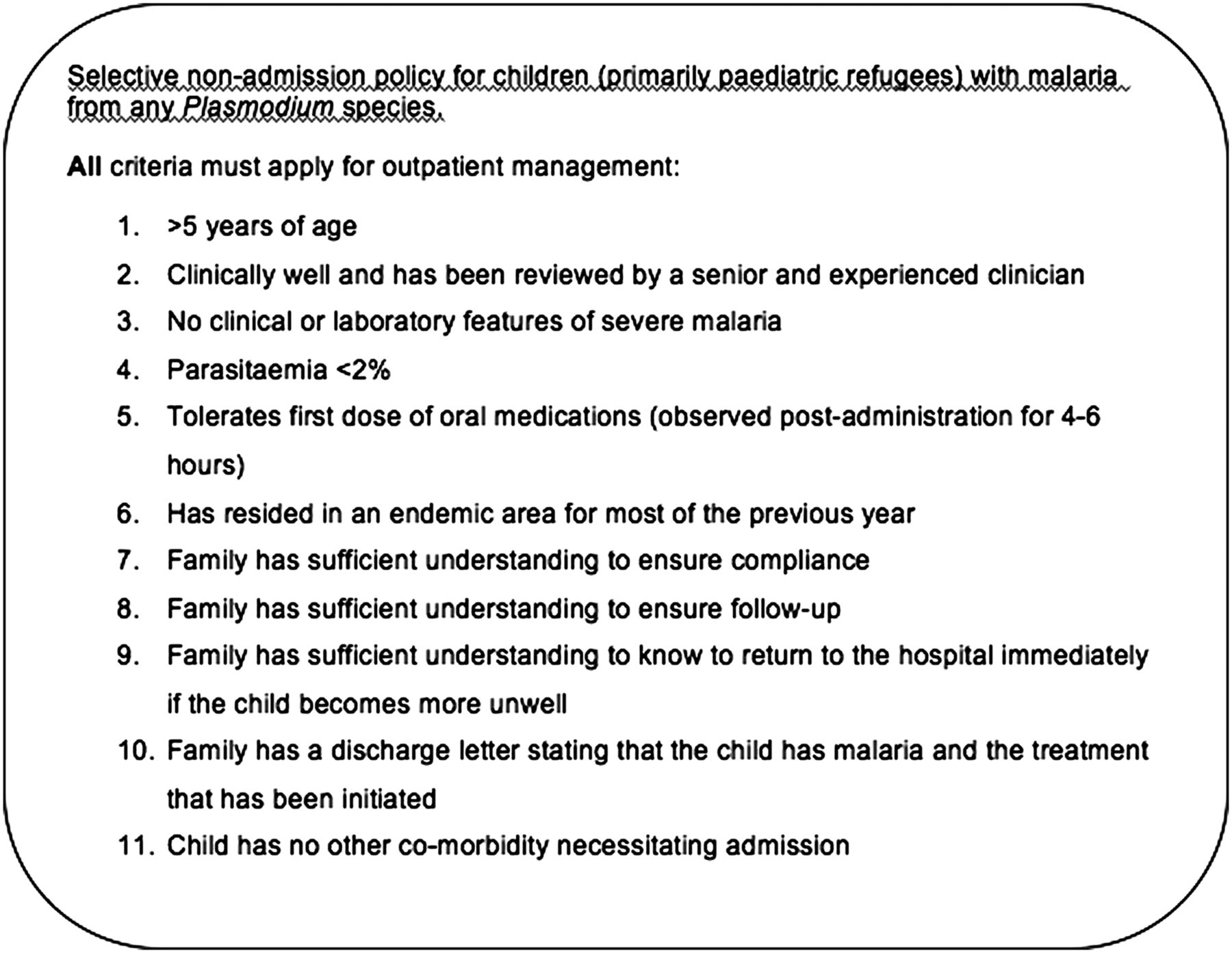
In children, Cherian and Burgner33 demonstrated that, by applying criteria similar to those listed in figure 2 to a group of 90 paediatric refugees with newly-diagnosed falciparum malaria, hospitalisation could be avoided in over 60% of cases. By extension, these criteria could probably be applied safely to children with non-falciparum malaria as well, although data are lacking.
{kind=link}
{kind=link}
Selective non-admission policy for paediatric refugees with Plasmodium falciparum malaria. Adapted from Cherian and Burgner.33
Although it is clinically well-known (and rightly feared) that young children, especially those <5 years of age, are at increased risk of rapid deterioration and death, this study provides some evidence that an increasing number of selected children, who are likely to have some antimalarial immunity, may be managed safely at home. Alternatively, these children may be managed by ‘hospital in the home’ programmes, if available. The decision to manage a child with malaria without hospital admission should be made by clinicians experienced in management of malaria, with consideration of likely antimalarial immunity and ‘safety net’ provisions should the child's condition deteriorate. If there is concern that patient safety will be compromised by outpatient treatment, the child should be admitted to hospital.
In summary, the recommendations in this update reflect the current WHO malaria treatment guidelines and are tailored to the treatment of imported malaria in children in non-endemic countries. This update also reflects the divergence of treatment options between these countries, based on availability of ACTs. In light of the recent high-quality evidence around the effectiveness of artemisinins in children, the inclusion of intravenous artesunate and oral ACTs into the national protocols of non-endemic countries and their improved availability should be encouraged.
Acknowledgments
Many thanks to Drs. Ric Price and Nick Anstey (Menzies School of Health Research, Global and Tropical Health Division, Darwin, Australia) for generously volunteering their knowledge and advice for this review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors PB, DS, SL, AS, and DB provided intellectual input into the manuscript, and reviewed and approved the final draft.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.