Article Text

Abstract
Background Clinical decision rules (CDRs) for paediatric head injury (HI) exist to identify children at risk of traumatic brain injury. Those of the highest quality are the Canadian assessment of tomography for childhood head injury (CATCH), Children's head injury algorithm for the prediction of important clinical events (CHALICE) and Pediatric Emergency Care Applied Research Network (PECARN) CDRs. They target different cohorts of children with HI and have not been compared in the same setting. We set out to quantify the proportion of children with HI to which each CDR was applicable.
Methods Consecutive children presenting to an Australian paediatric Emergency Department with HIs were enrolled. Published inclusion/exclusion criteria and predictor variables from the CDRs were collected prospectively. Using these we determined the frequency with which each CDR was applicable.
Results 1012 patients (69.9%) were enrolled with 949 available for analysis. Mean age was 6.8 years (21% <2 years). 95% had initial Glasgow Coma Scale 15. CT rate was 12.8% and neurosurgery rate was 0.7%. No CDR was applicable to all patients. CHALICE was applicable to the most (97%, 95% CI 96% to 98%) and CATCH to the fewest (26%, 95% CI 24% to 29%). PECARN was applicable to 76% (95% CI 70% to 82%) aged <2 years, and 74% (95% CI 71% to 77%) aged 2–<18 years.
Conclusions Each CDR is applicable to a different proportion of children with HI. This makes a direct comparison of the CDRs difficult. Prior to selection of any for implementation they should undergo validation outside the derivation setting coupled with an analysis of their performance accuracy, usability and cost effectiveness.
- paediatric emergency med
- diagnosis
- Trauma, head
- imaging, CT/MRI
- paediatric injury
Statistics from Altmetric.com
Background
In developed countries, head injury (HI) is a significant cause of childhood death and neurological disability.1 ,2 The annual incidence of HI is estimated at 1850/100 000 for 0–4 year olds, 1100/100 000 for 5–9 year olds and 1170/100 000 for 10–14 year olds,3 and is therefore a very common reason for presentation to the Emergency Department (ED). While the majority (80%–90%) of HIs in childhood are mild,4–7 a proportion of these children are at risk of avoidable poor outcome.2 ,6 ,8–11
Cranial CT is currently the reference standard investigation for intracranial injury. It provides rapid identification and guides management, with early diagnostic imaging linked to improved outcomes and reduced admission rates.12 However, cranial CT scans have risks associated with ionising radiation-induced malignancies, and with sedation in young and uncooperative patients.13–17 Despite this, cranial CT rates for paediatric HI have increased markedly over the last 2 decades.10 ,18 ,19
Clinical decision rules (CDRs) help clinicians make medical decisions and are based on original research. They use elements of patient history, physical examination or simple tests to provide a clinical tool.20–22 To optimise the balance between identifying significant intracranial injury and minimising the risks associated with cranial CT, several CDRs for paediatric HI have been derived.2 ,8–10 ,12 ,23 ,24
While many CDRs for HI appear superficially similar, they differ significantly in their details, employing different predictor variables and suggesting different courses of action.12 ,24 They have been derived using different outcomes, age limits, inclusion and exclusion criteria, and have focused on different severities of HI. None have been prospectively validated other than in their derivation population, and no prospective comparison of their performance has yet been undertaken.12 ,24
There are many reasons why a CDR for paediatric HI should be widely implemented in EDs: it is a common ED presentation, there is potential for avoidable poor outcome, there is large variability in practice and cranial CT rates have been increasing.2 ,8 ,18 ,24 The potential impact of implementation can be estimated by assessing predictive validity and clinical sensibility, and by measuring the potential to improve decision making.22 At present, uncertainty exists as to which would be the most appropriate CDR to implement.
It is now essential that external validation and comparison be undertaken as many EDs are poised to introduce one or more of these CDRs into practice.24 ,25 This should include assessment of their performance accuracy and impact in order to guide clinicians as to which to implement. As a first step prior to multicentre validation we assessed their theoretical applicability in the same setting. The goal of this investigation was to describe how many patients in the same population each CDR was applicable to when interpreted strictly using the published inclusion and exclusion criteria (such as time of presentation post-HI, Glasgow Coma Scale (GCS) limits or presence of specified medical conditions).
Methods
Study setting
We conducted a prospective observational study in the ED of the Royal Children's Hospital, Melbourne (RCHM), Australia, with an annual census of 69 000. This is a tertiary paediatric ED which serves the children of metropolitan Melbourne and is the sole paediatric trauma centre for the state of Victoria. Patients were enrolled from 11 April 2011 to 17 October 2011.
Inclusion and exclusion criteria
We aimed to assess the applicability of the CDRs in children younger than 18 years of age presenting with HI of any severity. Patients were excluded if they had already received neuro-imaging at another institution. Patients who did not undergo neuro-imaging and did not have a telephone follow-up completed were excluded from the analysis.
Standardised patient assessment
Clinicians and research assistants underwent a standardised training process and collected data on specifically designed clinical report forms. On an ED form, clinicians recorded the clinical predictor variables of each CDR prospectively at the time of initial assessment before neuro-imaging was performed. On separate forms, completed following ED management, research assistants recorded non-clinical variables and outcomes including follow-up information.
CDR selection
We aimed to assess the applicability of the CDRs which are most likely to be incorporated into clinical practice. Previous work 10 ,12 ,24 has demonstrated that those derived with the best methodology and which merit further assessment are Canadian assessment of tomography for childhood head injury (CATCH),8 Children's head injury algorithm for the prediction of important clinical events (CHALICE)9 and the CDR derived by the Pediatric Emergency Care Applied Research Network (PECARN)2.
Assessment of applicability
Clinicians in the ED treated patients as per their usual practice, which is based on an existing RCHM clinical practice guideline for HI.26 Inclusion and exclusion criteria specific to each CDR were retrospectively applied using the data collected from each patient. We assessed what proportion of patients in the same population were theoretically captured by the CDRs when they were strictly applied using the published inclusion and exclusion criteria.
Ethics approval
Verbal consent was gained either at the time of presentation or at subsequent telephone follow-up. The study was approved by the RCHM ethics committee.
Data collection and analysis
Data were collated in Epidata V.3.1 (Lauritson, JM., The Epidata Association, Odense, Denmark) and analysed using Stata Intercooled V10.0 (Stata Corporation, College Station, Texas, USA). Relevant proportions are presented with 95% CI.
Results
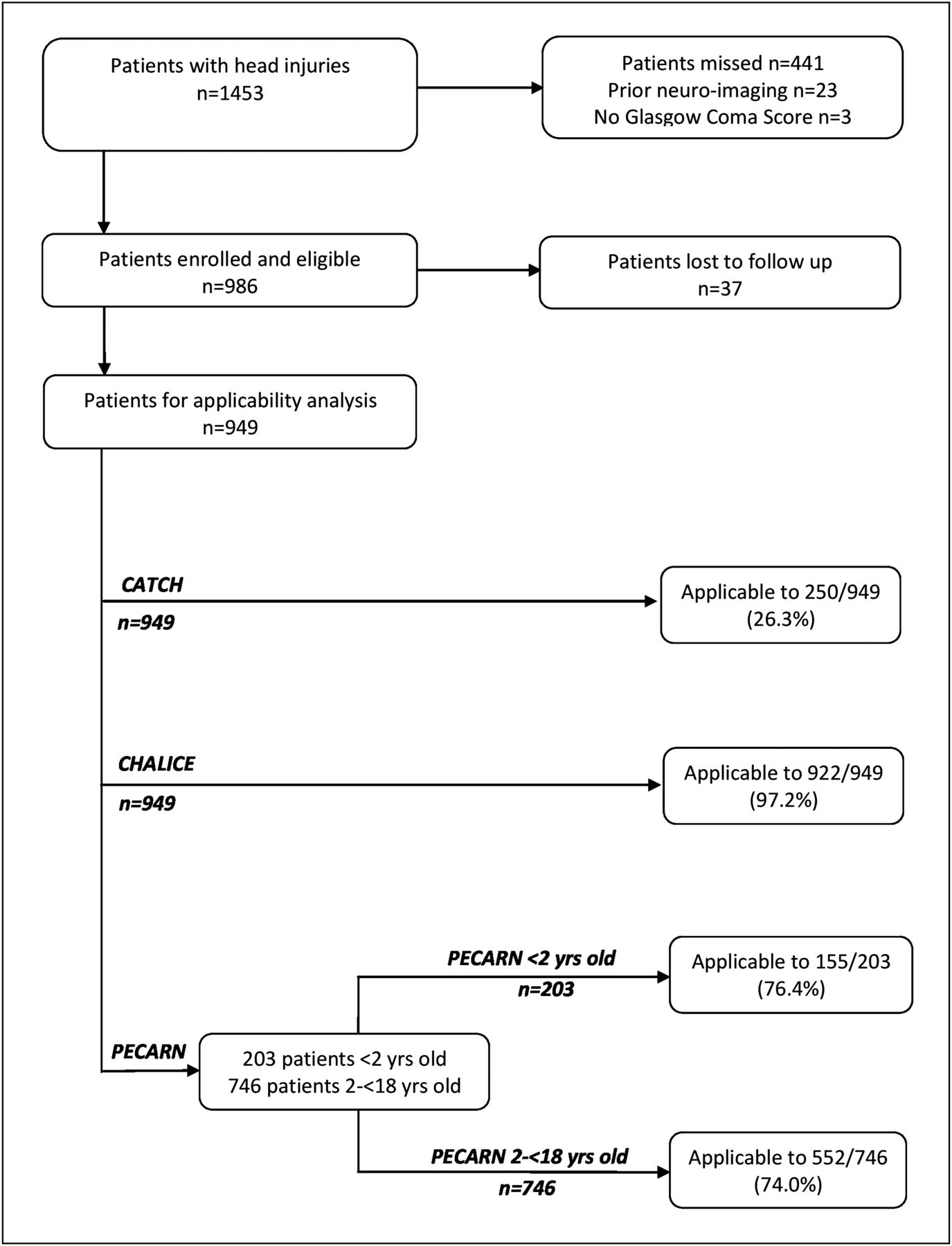
During the study period, there were 1453 patients with head injuries of any severity. Of these, 1012 were enrolled (recruitment rate 69.6%). Twenty-three had neuro-imaging prior to arrival and in three GCS had not been recorded. A total of 37 of 986 (3.8%) remaining eligible patients could not be contacted in follow-up. Therefore, 949 patients (96.2%) either had a CT scan or had a telephone follow-up completed and these represent the study group. The patient flow is illustrated in figure 1. Age range was 18 days to 17 years 11 months, mean age was 6.8 years (standard deviation 5.1 years) and 203 (21.3%) were less than 2 years of age. Overall, 66.6% were male. The majority of patients had a GCS of 15/15. A cranial CT scan was performed in 121 (12.8%, 95% CI 10.7% to 15.0%), and neurosurgery was performed in 7 (0.7%, 95% CI 0.3% to 1.5%) Patient characteristics were compared with the sample characteristics of the other CDR derivation studies (table 1).

{kind=link}
Flowchart to assess applicability of paediatric head injury clinical decision rules. CATCH, Canadian assessment of tomography for childhood head injury; CHALICE, children's head injury algorithm for the prediction of important clinical events; PECARN, Pediatric Emergency Care Applied Research Network.
CATCH was applicable to 250 patients (26.3%, 95% CI 23.6% to 29.3%) and CHALICE to 922 (97.2%, 95 CI 95.9% to 98.1%). PECARN was applicable to 155 of 203 patients aged less than 2 years (76.4%, 95% CI 69.9% to 82.0%), and 552 of 746 patients aged from 2 years until their 18th birthday (74.0%, 95% CI 70.7% to 77.1%) (table 2).
Overall applicability of CATCH, CHALICE and PECARN
In those patients to whom CATCH was not applicable, the most common reason (682/699, 97.6%) was that they did not fulfil the CATCH definition of minor HI: (i) injury within the last 24 h with (ii) witnessed loss of consciousness, definite amnesia, witnessed disorientation, persistent vomiting (more than one episode) or persistent irritability (in a child under 2 years of age) (iii) in a patient with a GCS of 13–15 (table 3).
CATCH: criteria for non-applicability
In the study group, CHALICE was not applicable to 27 patients as they were 16 years of age or older. There were no other reasons for non-applicability. When used specifically for minor HI (GCS 13–15), CHALICE was applicable to 908 (95.7%) patients, with a further 14 ineligible as they had an initial GCS of <13.
In those children to whom PECARN was not applicable, the most common reasons were that the HI was trivial (defined by PECARN as ground level falls or walking or running into stationary objects, and no signs or symptoms of head trauma, other scalp abrasions and lacerations) or that the ED attendance was more than 24 h after the injury. In children aged <2 years, these accounted for 31/48 (64.6%) and 15/48 (31.3%), respectively, and in those aged 2–<18 years, 92/194 (47.4%) and 68/194 (35.1%), respectively. In both groups, there were some children who fulfilled more than one criterion for non-applicability. There were no children who were outside the specified age range (table 4).
PECARN: criteria for non-applicability
Discussion
Our data show that when applied as published, the three CDRs investigated—CATCH, CHALICE and PECARN2 ,8 ,9—apply to very different proportions of children presenting to the ED following HI. The CDRs we assessed were developed with the same overarching purpose (to aid management of paediatric HI) and were derived to high methodological standards.24 This variability in applicability reflects the differences in HI severity, predictor variables, and inclusion and exclusion criteria in the derivation studies. Our population broadly reflected the derivation population of each CDR in terms of age, sex and injury severity (defined by GCS).
CDRs help clinicians cope with the uncertainty of medical decision making.21 When selecting a CDR for implementation, consideration must be given as to which patients will benefit. In paediatric HI, it could be argued that they may be most clinically useful for those patients who present diagnostic difficulty as for other patients decisions on imaging are clear. This approach has given rise to some of the heterogeneity of the derivation studies, and hence the variable applicability of the CDRs. CATCH and PECARN were developed to aid in the management of minor paediatric HI, though their definitions of minor HI differ, contributing to the varying applicability rates. The CATCH definition serves as their inclusion criteria, and has the greatest effect on the applicability of the CDR. The CATCH group deliberately used a very specific definition of minor HI to create a CDR for patients in whom decisions regarding neuro-imaging were difficult, rather than those in whom the decision to CT or not to CT was seemingly obvious. CHALICE is applicable to almost all patients, but the authors also reported the performance accuracy for minor HI (GCS 13–15). In this cohort CHALICE applicability decreased, but was still higher than the other two CDRs which focus on minor HI. PECARN also focused on a specific population, most notably excluding those with a defined trivial HI, a cohort of patients which no clinician would consider scanning as the risks clearly outweigh the benefits. This is the cohort of patients which most affects the applicability rates of PECARN, though it remains applicable to the majority of patients.
Clinicians may apply a CDR inaccurately or unreliably,22 and all CDRs should be applied with careful attention to the exact definitions of clinical predictor variables.27 When assessing patients some clinicians may use only the flowchart or figure illustrating the CDR as an aide memoire and not refer to other published criteria. This results in the CDR being applied to a wider population than that intended. When using the illustrative flow chart or figure alone without the text of the publication for applicability, CATCH would have been applicable to an additional 2% patients, CHALICE an additional 3% patients, and PECARN <2 years and 2–<18 years an additional 24% patients each. Our data indicate that careful attention should be paid to the details of inclusion and exclusion criteria of the CDRs as published.
The demonstrable difference in applicability highlights the need for a sufficiently powered multi-centre validation and comparison of these CDRs prior to selection of one for widespread implementation. A study of this magnitude would facilitate identification of the cohort of children with HI most in need of a CDR, and this applicability data will therefore aid in deciding which CDR to implement. In addition to an assessment of their performance accuracy in an independent setting, any such comparison should also evaluate the projected cranial CT rate and the impact on the healthcare system through a cost effectiveness analysis.
Limitations
This is a single centre study in a tertiary paediatric ED and therefore its findings may not be generalisable. However, given the size of the sample and the consistency of the patient characteristics with the CDR derivation studies, applicability rates are likely to be broadly similar in similar settings. Previous studies of the epidemiology of HI at RCHM have shown peaks in incidence in March and December. This study was not performed over a full year but it is unlikely that this would significantly affect applicability rates.
Conclusions
Due to heterogeneity in their derivation, each CDR is applicable to a different proportion of children with HI when used as published. This makes direct comparison difficult. Clinicians should pay careful attention to the details of derivation studies in order to ensure correct application. Prior to selection of any for implementation, these CDRs should undergo prospective validation coupled with comparison of their performance accuracy, usability and cost effectiveness. This should be undertaken both for the specific cohorts to which they are applicable and for the whole population of children with HI.
Acknowledgments
We acknowledge grant support from the Murdoch Children's Research Institute, Melbourne, Australia, and the Victorian Government's Operational Infrastructure Support Program.
References
Footnotes
-
Contributors ML and FB participated in all stages, including study design, production of materials, enrolment of subjects, data collection and analysis, and authoring the article. JC, CB, EO, BW and AF assisted in study design, patient enrolment, data collection and contributed to the article. KJ designed the database and analysed the data, and contributed to the drafting of the article.
-
Funding The study was supported in part by grant funding from the Murdoch Children's Research Institute (MCRI), Melbourne, Australia. MCRI is a non-governmental paediatric research institute. There was no influence from the part funder on design or conduct of the study.
-
Competing interests None.
-
Ethics approval Royal Children's Hospital, Melbourne, Australia.
-
Provenance and peer review Not commissioned; externally peer reviewed.