Article Text

Abstract
Background: A recent update suggested that the National Institute for Health and Clinical Excellence (NICE) guidance on head injury had led to safe early discharge, evidence of a reduction in the numbers of admitted patients and cost savings in some centres. The aim of this study was to use national Hospital Episodes Statistics (HES) data to determine whether admissions with head injury have changed since the NICE guidance was introduced.
Methods: HES data coded as S00–S09 “Injuries to the head” from 1998–9 to 2006–7 were examined for admissions, age and length of stay.
Results: Admissions rates did not change markedly until 2003 when the NICE head injury guidelines were issued. From 2003, admissions increased for all adult age groups but not for children. Mean length of stay remained constant between 1998 and 2007, so bed days increased in proportion to admission rates.
Conclusion: Adult head injury admissions in England have increased markedly since the introduction of the NICE guidelines. Given that there is little evidence that hospital admission is beneficial for patients with minor head injury, NICE head injury guidance appears to have failed to promote cost effective care.
Statistics from Altmetric.com
Head injury is responsible for around 700 000 emergency department attendances per year in England and Wales, most of which (90%) will be minor (Glasgow coma score 13–15) and will not need immediate neurosurgical intervention or inpatient care.1 The National Institute for Health and Clinical Excellence (NICE) published guidelines for the management of head injury in 2003.1 The guidance for management of minor head injuries was based upon the Canadian CT head rule and was anticipated to lead to more CT scans being performed, but fewer skull radiographs and admissions. Concerns were raised that these objectives would not be achieved,2 but a recent update suggested that the guidance had led to safe early discharge, evidence of a reduction in the numbers of admitted patients and cost savings in some centres.3
Several small studies in single centres have compared care before and after introduction of the NICE guidelines and have confirmed that more CT scans and fewer skull radiographs are being performed, but have provided mixed results in relation to hospital admissions.4–7 The aim of this study was to use national Hospital Episodes Statistics (HES) data to determine whether admissions with head injury have changed since NICE guidance was introduced.
METHODS
HES is a data warehouse containing details of all admissions to NHS hospitals in England and is openly accessible online (www.hesonline.org.uk). Data on all acute hospital episodes from 1998 have been collected, assembled and made available online. Cases are recorded as Finished Consultant Episodes: a period of admitted patient care under a consultant or allied healthcare professional within an NHS trust. Diagnoses are currently coded according to the International Classification of Diseases, 10th Revision (ICD-10). The data also include patient age, location, hospital and length of stay. HES online data are provided as aggregate tabulated data. This study selected episodes coded as S00–S09 “Injuries to the head” from 1998–9 to 2006–7 and reported hospital admissions, mean length of stay, sex and age categories.
The NICE head injury guidelines were published in 2003 and updated in 2007. They were disseminated to clinicians working in emergency care, radiology, neurosurgery and rehabilitation, and were widely discussed in the medical literature. Local service providers were responsible for implementation of the guidelines. There were no specific resources allocated to support implementation or incentives developed to promote implementation.
RESULTS
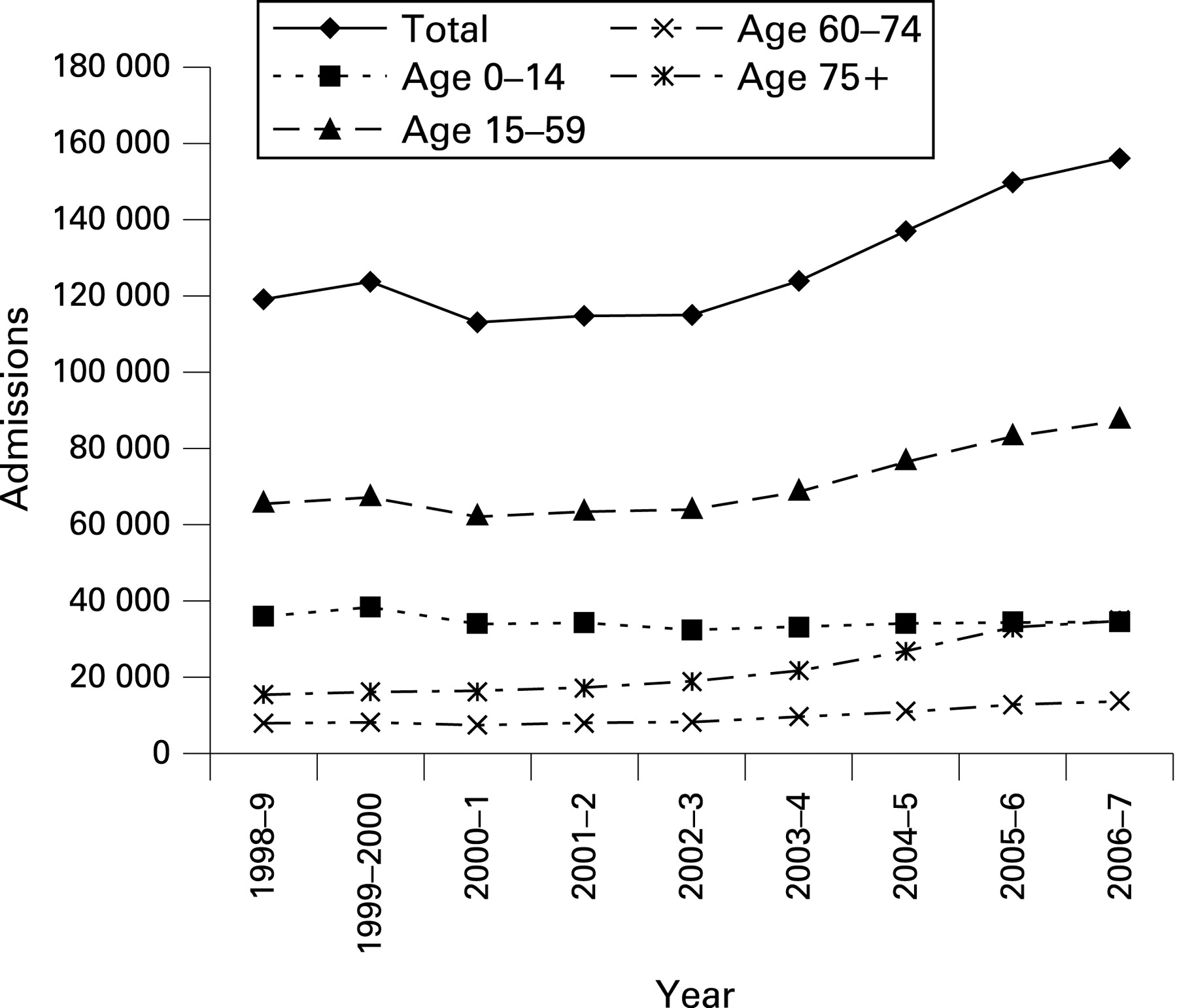
HES head injury data are shown in table 1 and the admissions data are shown in fig 1. Admissions rates for all age groups did not change markedly until 2003 when the NICE head injury guidelines were issued. Since 2003, admissions have increased for all adult age groups but not children. Mean length of stay has remained constant between 1998 and 2007, so bed days have increased in proportion to admission rates.
{kind=link}
DISCUSSION
Head injury admissions in England have increased markedly since the introduction of the NICE guidelines. There may have been other factors influencing practice over this time so we cannot conclude that the guidelines have definitely caused this increase, but they have not achieved the anticipated reduction in admissions. It is possible that concurrent changes in practice, such as the 4 h target for waiting times in the emergency department or changes in the specialty responsible for admission, may explain the recent increase in admissions. However, if the increased admissions were merely an administrative artefact, we would expect mean length of stay to have fallen, but there is no evidence of this. As a result, total bed days have increased.
This study is based upon routine health service data and is thus subject to some inevitable limitations. Detailed reasons for admission are not recorded, so it is not possible to determine whether the increase in admissions was due to particular issues such as drug or alcohol intoxication or medical co-morbidities. It is also not possible to determine why admissions appear to have increased. It may be that the increased use of CT scanning promoted by NICE guidance has resulted in detection of additional injuries prompting admission or, alternatively, that the reduced use of skull radiography has prompted clinicians to be more cautious in their approach to patient discharge. A more detailed analysis of the patients admitted is required to address this issue.
This analysis cannot determine whether patients may have received benefit from hospital admission, either through early detection of intracranial injury or management of psychosocial issues with careful discharge planning and appropriate follow-up. Previous studies have identified little evidence of benefit from hospital admission for minor head injury,8–10 but these have not looked carefully for subjective health benefits such as early return to normal activities. However, it appears clear from this study that there has been a considerable increase in resources used to care for patients with head injury. Without corresponding evidence of patient benefit, it may be reasonable to conclude that the NICE head injury guidelines have failed to promote cost effective care.
Footnotes
Competing interests: None.
Linked Articles
- Primary survey