Article Text

Abstract
Structured in the format recommended by Hayward et al1 for guideline reports.
Objective: An evidence and consensus based guideline for the management of the child who presents to hospital having had a seizure. It does not deal with the child who is still seizing. The guideline is intended for use by junior doctors, and was developed for this common problem (5% of all paediatric medical attenders) where variation in practice occurs.
Options: Assessment, investigations (biochemistry, lumbar puncture, serum anticonvulsant levels, EEG in particular), and/or admission are examined.
Outcomes: The guideline aims to direct junior doctors in recognising those children who are at higher risk of serious intracranial pathology including infection, and conversely to recognise those children at low risk who are safe to go home.
Evidence: A systematic review of the literature was performed. Articles were identified using the electronic data bases Medline (from 1966 to June 1998), Embase (from 1980 to June 1998) and Cochrane (to June 1998), and selected if they investigated the specified clinical question. Personal reviews were excluded. Selected articles were appraised, graded, and synthesised qualitatively. Statements of recommendation were made.
Consensus: An anonymous, postal Delphi consensus development was used. A national panel of 30 medical and nursing staff regularly caring for these children were asked to grade their agreement with the statements generated. They were sent the relevant original publications, the appraisals, and literature review. On the second and third rounds they were asked whether they wished to re-grade their agreement in the light of other panellists’ responses. Consensus was defined as 83% of panellists agreeing with the statement.
Recommendations in brief: For afebrile seizures all children should have their blood pressure recorded, but no other investigations are routine although a seizing or somnolent child should have blood glucose measured; all children under 1 year should be admitted. For seizures with fever, clinical signs indicating the need to treat as meningitis are given. Children should be admitted if they are under 18 months old, have had a complex seizure, or after pretreatment with antibiotics.
Validation: The guideline has undergone implementation and evaluation in a paediatric accident and emergency department, the results of which will be published separately. Only one alteration was made to the guideline as a result of this validation process, which is included here.
- seizure
- Delphi consensus
- child
- guideline
Statistics from Altmetric.com
Seizures are common in children. Three per cent of all children 6 months to 5 years have a febrile seizure, and 5% of all medical attendances to the accident and emergency department are attributable to seizure.2 Depending on the hospital attended and the clinician seen, about 70% of these children are admitted and undergo varying degrees of investigation3 and length of stay in hospital. The Royal College of Paediatrics and Child Health recommends that priority for guideline development be given to aspects of health care that are common, expensive or serious, and where variations in practice occur.4 Thus the management of childhood seizure is appropriate for guideline development.
Potential benefits (improved health outcome, consistency of care, patient information) and harms (priorities and recommendations flawed) of clinical guidelines have been well documented.5 We developed the guideline with the following goals: (1) to improve the process and outcome of care for children attending our accident and emergency department with a seizure; (2) to promote consistency of care so that patients with similar clinical problems would be managed in the same way; (3) to inform, educate, and improve the clinical decision making of the junior clinicians who see most of these children initially.2
SCOPE OF THE GUIDELINE
The guideline deals with children who have had a seizure as a presenting problem, rather than a defined diagnosis as staff need guidance on determining diagnosis before deciding on management.6 The emergency management of the seizing child is not covered as it is dealt with clearly in accessible texts.7 We present a summary version of the full guideline, which can be obtained from the corresponding author electronically, and to which reference should be made for clarification or further information. The development group assumes that healthcare professionals will use general medical knowledge and clinical judgement in applying the recommendations in this document to the management of individual patients.
METHOD
We chose an algorithm format, where the recommended course of action at each stage depends critically on the available information.8 This has been shown to be successful in education.9
The guideline concentrates on the management of the child up to the point at which the decision is made to admit to hospital or discharge home. As such, the primary options considered are the important features on history and examination directing the clinician to a particular cause and the investigations required for diagnosis and initial management. Key clinical questions concerning the management of the child presenting with seizure drove our search strategy. Specific questions, type of question and specific search terms (as mesh headings and text words) were defined.
We used electronic databases (Cochrane library (to March 1998); Medline (1966 to March 1998); Embase (1980 to March 1998), confined to humans aged 0–16 and English language), and citations in references found. The references generated were sifted for relevance to the clinical questions by their titles and abstracts. Inclusion criteria were: articles that investigated the clinical questions identified; scientific literature reviews; review or clinical guideline written by a national body; large well designed clinical trials (RCT, matched case control, cohort). Non-experimental, descriptive, or opinion based studies were excluded. Some retrospective cohort studies were included in the absence of stronger evidence and were graded accordingly. Articles were appraised using a pre-designed proforma and graded using a standard scale (appendix 1). Statements of recommended management were made based on this literature.
The statements were subject to consensus development by means of a postal Delphi process. Panellists selected were drawn from the United Kingdom, represented practice in both urban and rural settings and were clinicians who would be involved in management of a child after presentation at hospital. Eighty medical and nursing staff were invited, of whom 30 took part (panel composition in appendix 2). They rated their level of agreement on a 1 to 9 Likert scale and were asked to comment. Consensus agreement was defined as 83% of panellists rating 7 to 9. Two rounds of feedback and further rating were made. Those statements that gained consensus are included in the guideline.
THE GUIDELINE
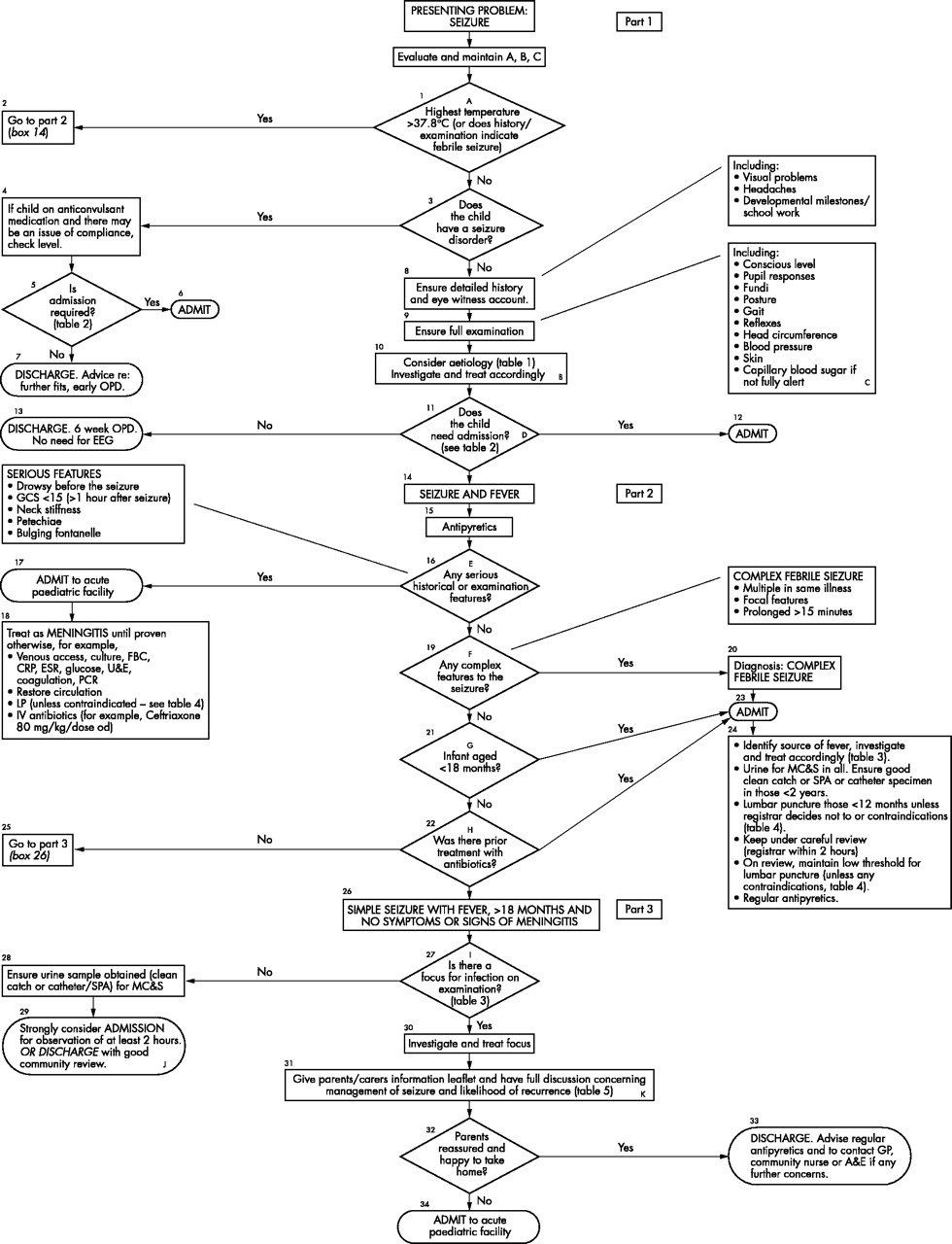
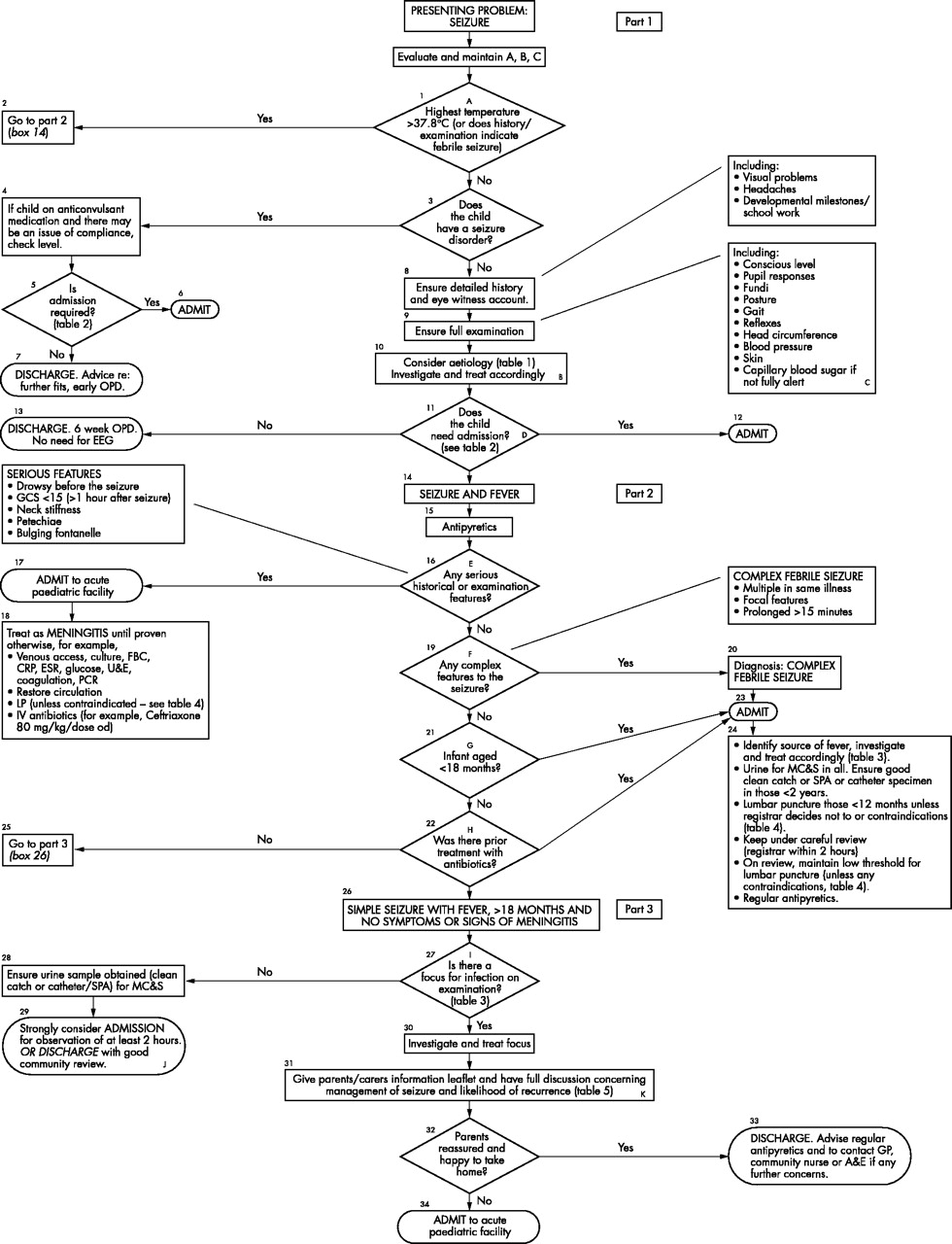
The final guideline is in the form of an algorithm (flow diagram or decision tree) and is shown in figure 1, with integral tables 1 to 5. Each box is numbered, and key decision points are allocated a letter, with recommendations explained in the text. A brief discussion concerning the evidence base is given, followed by the consensus guideline statements in italics, with their level of evidence and grade of recommendation.
List of causes of an afebrile seizure in a child presenting to the accident and emergency department
Criteria for admission of a child with a first afebrile seizure to an acute paediatric facility
Common causes of fever in children presenting with fever and seizure
Contraindications to lumbar puncture
Prognosis of febrile seizures
{kind=link}
Seizure guideline algorithm.
Throughout, the word “admit” is defined as follows: any admission to a paediatric facility with paediatric trained staff for observation, further investigation, and management regardless of the expected length of stay.
Children are managed differently depending on whether they are thought to have had a febrile or an afebrile seizure. The upper part of the algorithm deals with afebrile seizures, whereas the middle and bottom parts deal with febrile seizures. Crucial to this division is the definition of febrile seizure.
A Definition of fever in febrile seizure
There is no compelling evidence in the literature concerning the level of fever required to diagnose febrile seizure. Definition of fever depends on the method of measurement and these guidelines should be adapted to a locally preferred method. An axillary temperature of >38°C was proposed in the first Delphi round 10–12(Vb,D) but consensus was not achieved. In the second round the Likert scale was modified such that actual temperatures (between 37.0°C and 38.6°C in increments of 0.1 of a degree) were given. Panellists were asked to “place one cross only in the temperature box that corresponds to the lowest recorded axillary temperature that would lead you to make a preliminary diagnosis of seizure with fever”. The median and modal values were 37.8°C with a range of 37.7°C to 38.0°C and interquartile range all within box 37.8°C.
During the validation study it was clear that a simple temperature cut off was not practical and therefore the statement was modified to allow diagnosis of “febrile seizure” if the history and examination was indicative. This decision was in keeping with the definition developed at a consensus conference at the National Institutes of Health in 1980.
RECOMMENDATION on defining febrile seizure:
-
The temperature level to define fever with seizure is above 37.8°C.
-
Modification during validation: “However, if the clinical history and examination is indicative of a febrile seizure (seizure associated with fever but without evidence of intracranial infection or a defined cause) the patient should be managed as such”.
(level of evidence Vb, Delphi panel based, no consensus reached, precise wording decided during validation study, grade D recommendation)
AFEBRILE SEIZURES
B Determining the aetiology of a child presenting with an afebrile seizure
RECOMMENDATION on most likely causes of an afebrile seizure:
Table 1 (based on Smith et al13 observed diagnoses in children presenting to an A&E department over a one year period with a first seizure) for differential aetiology of an afebrile seizure.
(Based on Level Vb evidence and Delphi consensus, grade D recommendation)
C Diagnostic tests for the child presenting with an afebrile seizure
Studies on afebrile seizures have found no routine investigations to be of consistent value (in children13,14 and adults15,16). Unusual historical or examination features should direct investigations. Studies on the positive yield of EEG were done in adults only, where it is not a useful diagnostic test after a first simple seizure.15,16 Children should have systemic hypertension presenting as a seizure excluded by sphygmomanometry.
RECOMMENDATION on investigations for afebrile seizure:
-
All children presenting with an afebrile seizure should have their blood pressure measured at the time of presentation.
-
A finger prick blood glucose should be performed if a child is still seizing or not fully alert.
-
No other investigations (that is, other than blood pressure and blood sugar) are routinely indicated in a child over 1 year of age with a simple afebrile seizure, who does not fulfil the criteria for observation or admission.
-
There is no need for an EEG after a first simple afebrile seizure.
(The above based on Level Vb evidence and Delphi consensus, grade D recommendation)
D Need for admission in children with afebrile seizures
Seizures in early infancy are often “symptomatic” (that is, secondary to underlying pathology) and therefore investigation and observation are essential17(Vb,D). No other literature was found investigating this issue. Initial statements were derived from text book recommendation, and modified by consensus.
RECOMMENDATION concerning admission in afebrile seizure:
After a first afebrile seizure, children conforming to the stated criteria (table 2) should be admitted to an acute paediatric facility for observation and further investigation.
(Level Vb evidence and Delphi consensus, grade D recommendation)
FEBRILE SEIZURES
E Febrile seizure, risk of meningitis, and clinical features
In children admitted to hospital there are several studies of variable validity looking at the probability of meningitis (table 6). The signs included in the statement below were found to indicate an increased risk of meningitis in a child with seizure and fever18,19 (III, C):
Published reports of the probability of bacterial meningitis in children with fever and a seizure
RECOMMENDATION on clinical features indicating meningitis:
-
A child who presents with seizure and fever and has any of the following on history or examination should be treated as having meningitis until proven otherwise: drowsy pre-seizure, neck stiffness, petechial rash, bulging fontanelle, a Glasgow Coma Scale of <15 (more than one hour post seizure).
(Level III evidence and Delphi consensus, grade C recommendation)
F Complex febrile seizures
The literature suggests that complex febrile convulsions (prolonged seizure (>15 min), multiple seizures in 24 hours and focal features) increase the risk of further seizures and epilepsy20–23 (III,C) and are also predictive of CNS infection18,19(III,C) 24,25(Vb, D). The risk of bacterial meningitis in children presenting with fever and seizure is about 3%18,19,25–27(III,C) and in a complex seizure, 9%.
After the first Delphi round it was agreed that children with complex seizures should be admitted to hospital. Two alternative statements were then given suggesting that children with a complex seizure should either have a lumbar puncture on admission or be reviewed in two hours. The second option gained consensus.
RECOMMENDATION in children with complex febrile seizures
-
A child presenting with a complex febrile seizure (defined above) with no clinical signs of meningitis (section E) should be observed closely and reviewed within two hours by a paediatrician of at least registrar level to decide on need for lumbar puncture.
(Implied by Level III evidence. Delphi consensus, grade C recommendation)
RECOMMENDATION on contraindications to lumbar puncture:
Table 4 shows the contraindications to LP.28,29
(Level Vb evidence and Delphi consensus, grade D recommendation)
G Age and risk of meningitis in febrile seizures
The population risk of meningitis (with or without seizure) based on figures from 1980 to 199030 is highest in those aged 1 to 11 months (115/100 000 versus 28.5/100 000 for 1–5 years and 2.8/100 000 for 5–16 years). This rate has decreased since the introduction of HIB vaccine, but remains highest in the under 1 year olds. The statement that children under 1 years of age (often extended to 18 months) can have meningitis without displaying any of the classic signs seems to be based on clinical experience and some early published case reports but is not born out by formal studies.18,19,24
Consensus views from the RCPCH (then BPA)11 and The American Academy of Pediatrics31 (AAP) suggest lumbar puncture under 18 months (probably) and almost certainly under 12 months. No view on admission is given.
RECOMMENDATION on age for admission and lumbar puncture in febrile seizure:
-
All children under 12 months with a first simple febrile seizure should be admitted.
-
Children under 12 months with a simple febrile seizure should have a lumbar puncture unless an experienced paediatrician (at least paediatric registrar) has decided not to lumbar puncture and will review within two hours.
-
Children 12 to 18 months with a simple febrile seizure should be admitted to an acute paediatric facility for a period of observation (at least two hours).
-
Maintain a low threshold for an lumbar puncture in children 12 to 18 months with a simple febrile seizure.
(Level Va evidence and Delphi consensus, grade D recommendation)
H Antibiotics and meningitis risk in febrile seizures
There is little evidence to support the statement that prior antibiotic treatment masks the signs of meningitis.18,19,24 However, the AAP31 suggest that lumbar puncture be strongly considered in these children. Three options were given to the panel after the first round of comments (i) admit and observe, (ii) lumbar puncture, or (iii) discharge if source of infection is evident and does not require hospital treatment. The first gained consensus.
RECOMMENDATION on management of the child who has already received antibiotics:
-
Those children with a simple febrile seizure, >1 year of age and with no serious historical or examination findings indicating meningitis who have had prior antibiotic treatment should be admitted to an acute paediatric facility for a period of observation (at least two hours)
(Level Va evidence and Delphi consensus, grade D recommendation)
I Causes of fever in children presenting with febrile seizure
RECOMMENDATION for differential diagnosis of fever in febrile seizure:
Table 3 gained consensus and was based on literature summarised in table 7.13,26,32,33
Identified or attributed causes of fever in children presenting with a febrile seizure (%)
Levels of evidence and grade of recommendation
Delphi panellists
(Level Vb evidence and Delphi consensus, grade D recommendation)
J Management of the child with febrile seizure and no focus of infection
There was no published evidence on this issue. The need for a good urine sample collected without contamination34 was agreed in the first round.
RECOMMENDATION on management of child with no focus of infection:
-
A child who has had a simple febrile seizure where no source for infection has been found clinically, should have a urine sample (clean catch, SPA or catheter specimen) taken for microscopy and culture.
After first round comments, two statements were given as alternative management plans concerning admission or discharge, and both achieved consensus, at the same level of agreement.
-
Children with no focus for infection can be admitted for a short period of observation (minimum two hours) OR
-
Children with no focus for infection can be discharged home if the child looks well, parents/carers have ready access to health care if required and they are happy with this decision.
(All the above based on Delphi consensus only, no published evidence)
K Prognosis after a first febrile seizure
RECOMMENDATION for prognosis of febrile seizure:
Information concerning prognosis is given in table 5 of the guideline21,35 and is available to inform the clinician’s discussion with parents.
(Level III evidence and Delphi consensus, grade C recommendation)
L Follow up for the child with febrile seizure
There is no published evidence concerning the need for follow up of children discharged following a simple febrile seizure.
RECOMMENDATION on follow up for the child with febrile seizure:
-
The Delphi panel agreed that an information sheet should be supplied (available from corresponding author) and follow up does not need to be arranged.
-
Parents of children sent home from A&E with a diagnosis of first simple febrile seizure should be encouraged to contact their own GP or community nurse specialist if they feel they need further information or care.
(No published evidence, Delphi consensus).
RESEARCH QUESTIONS
During the development of this guideline several areas were identified where good research evidence was lacking. The following questions were identified.
-
Is measuring the anticonvulsant level routinely justified in a child who presents with seizure and who is already taking anticonvulsant medication? If not, in which children and on which anticonvulsants should blood levels be measured?
-
What is the true population risk for meningitis in a child presenting with fever and seizure?
-
In children who present with a first simple febrile seizure, is discharge to general practitioner care as good as in patient care for limitation of risks, cost effectiveness, patient and parent satisfaction and education?
-
In a child presenting with a febrile seizure and a cause for fever is suspected on clinical examination, is it cost effective to take a routine urine sample? In what age group and by what method?
DISCUSSION
A comprehensive guideline is presented for the management of the child who has had a seizure based on best evidence and formal consensus using a Delphi panel. Management for those presenting with an afebrile seizure differs from those with a seizure associated with fever. Consensus was not achieved in defining a temperature level below which afebrile seizure could be diagnosed. However, panelists’ responses were tightly grouped from 37.7°C to 38.0°C. The reason for the lack of consensus may be that clinicians take into account many other factors in the history and examination when deciding on a diagnosis of “febrile seizure”. The guideline therefore recommends that the cut off level be decided locally. During the validation study it was clear that clinicians wanted the freedom to diagnose “febrile seizure” if the history and examination were highly suggestive even if the temperature did not reach the required level. For this reason the guideline suggests that clinicians should use their clinical judgement.
Key recommendations
For afebrile seizures
-
All children should have blood pressure recorded and a blood glucose taken if still seizing or not fully alert. Other investigations should be directed by history and clinical findings.
-
Children under 1 year of age should be admitted to hospital for further observation and investigation.
-
There is no need for an EEG in a first uncomplicated seizure.
-
An outpatient appointment should be offered.
For a seizure with fever
-
Admit and treat as meningitis children who were drowsy at home before the seizure, have a GCS<15 more than one hour after seizure, have neck stiffness, petechiae, or a bulging fontanelle.
-
Admit children with complex seizures, those less than 18 months, and those who have had antibiotics. The child should have an experienced paediatric review (at least registrar) within two hours concerning need for lumbar puncture.
-
Consider admission in those in which no focus for infection was found.
-
Others may go home with adequate parental information, reassurance, and ready access to health care.
Evidence from randomised trials was not available for constructing the original management statements. The highest level of evidence was level III on which only two statements (of 42) were directly based and seven were based by implication. The highest level of evidence (grade I) is that of a systematic review of randomised controlled trials using meta-analysis, and grade II is a good single randomised controlled trial with enough power to detect a difference. However this type of evidence only applies to questions concerning treatment, which are in the minority in a presenting problem based guideline. Different types of studies answer questions concerning population risk and diagnostic tests (symptoms and signs and laboratory investigations). A multicentre randomised controlled trial could be designed for practical management issues such as need for admission and follow up, but measurable outcomes are difficult to define. Thus for many practical clinical questions good evidence is lacking and is unlikely to be available in the near future, which highlights the need for good consensus methods.
Delphi consensus enabled a guideline to be produced where good published evidence is sparse. The guideline reflects a consensus of peer practice in that country at that time. Clinicians expressed reservations in some areas despite consensus being achieved. For example, the panel agreed that a urine sample should be taken from a child with febrile seizure in whom another source of infection is suspected. Despite this consensus, 14 of the panellists made written comments that expressed reservations about such a policy. It is possible that the “safest” options achieve consensus using this process but clinicians may act differently when they are seeing an individual child and can take other information into account.
There is little research into the method of Delphi consensus development, including the influence of different panels of individuals on outcome. While the panellists in this study were “self selected” in that they agreed to take part, it is difficult to conceive of an alternative to this.
As there was no level I or II evidence, these recommendations should be treated as a guide only. They will need adaptation for each local unit, and clinicians must exercise their own judgement as to whether the guideline applies to the individual patient seen.
The guideline has been validated in a paediatric A&E department and we intend to publish the results of the implementation study. Formal assessment of the costs of development of a presenting problem based guideline using Delphi consensus was not undertaken. We intend to evaluate costs during the development of the next guideline using the same methodology.
Acknowledgments
The following Delphi panelists for contributing a great deal of time and effort: H Allen (paediatric SpR), J H Baumer (paediatric consultant), R Bell (paediatric consultant), D Beverley (paediatric consultant), A Chambers (paediatric nurse), C Cramp (paediatric consultant), J Dawling (paediatric SpR), H Dixon (Paed. SpR), S Edees (paediatric consultant), M Everard (paediatric consultant), A Gregory (paediatric SpR), P Hardy (paediatric A&E SpR), S Hartland (paediatric A&E nurse), H Huynh (paediatric SpR), K Jackson (paediatric nurse), J Jenkins (paediatric consultant), B Lloyd (paediatric consultant), I Mecrow (paediatric consultant), J Moorcraft (paediatric consultant), R Morton (paediatric consultant), R Newton (paediatric neurologist), J Nixon (paediatric A&E nurse), K Palmer (paediatric consultant), A Raffles (paediatric consultant), C Simpson (paediatric nurse), C Smith (paediatric SpR), E Szondy (paediatric nurse), T Tinklin (paediatric consultant), C Upton (paediatric consultant), R Watkins (paediatric SpR), L Williams (paediatric A&E consultant). The authors thank Jeanette Taylor-Meek for her efficient and effective administration of the Delphi process
Contributors Kate Armon planned and coordinated the development of the study, developed core ideas, performed the literature review, appraised the articles found, generated initial guideline statements, coordinated the Delphi process, collated and analysed the data, produced the final guideline, and wrote the paper. Terence Stephenson had the original idea for the research and oversaw its development, participated in literature appraisal, development of guideline statements, and interpretation of data, discussed core ideas, edited the paper, and will act as guarantor. Roddy MacFaul initiated the research, had original ideas and discussed its development, participated in developing guideline statements, interpretation of data, and edited the paper. Pippa Hemingway discussed core ideas and development of research and edited the paper. Ursula Werneke had original ideas concerning the Delphi process, discussed the development of the research, and edited the paper. Stephanie Smith discussed core ideas and development of the research and participated in the Delphi process.
REFERENCES
Footnotes
-
Funding: Children Nationwide Medical Research Fund.
-
Conflicts of interest: none.
Linked Articles
- Primary Survey