Article Text

Abstract
METHODS Three patients with Borrelia burgdorferi infection and intracranial aneurysms are described.
RESULTS All three patients had neurological symptoms. Perivascular and vasculitic lymphocytic inflammation were detected in the brain biopsy specimen of one patient. The aneurysm was located in the internal carotid arteries in two patients and in the basilar artery in one patient. The aneurysm ruptured in two patients.
CONCLUSIONS Cerebral lymphocytic vasculitis and intracranial aneurysms may be associated with B burgdorferiinfection. It is suggested that inflammatory changes caused byB burgdorferi in vessel walls may be a pathogenetic mechanism for the formation of aneurysms.
- intracranial aneurysm
- Borrelia burgdorferi
- Lyme disease
- magnetic resonance imaging
- magnetic resonance angiography
- vasculitis
Statistics from Altmetric.com
- intracranial aneurysm
- Borrelia burgdorferi
- Lyme disease
- magnetic resonance imaging
- magnetic resonance angiography
- vasculitis
The spirochaete Treponema pallidum, the causative agent of syphilis, has in many studies been associated with vasculitis. It is also well known that syphilis may cause aneurysms, especially in the ascending aorta.1 Disseminated T palliduminfection typically causes obliterative endarteritis in small arteries, characterised by perivascular plasma cell and lymphocytic infiltrates. In syphilis, this endarteritis often develops in the vasa vasorum of large arteries and in medium sized arteries, making the vessel wall susceptible to aneurysm formation.1 Another spirochaetal infection, Lyme borreliosis, has recently been described in association with coronary artery aneurysms,2 although a causal relation of Borrelia burgdorferi infection with aneurysms has not yet been shown.
B burgdorferi is able to adhere to and penetrate at an early stage of the infection through the vascular endothelium and cause vasculitis and perivascular inflammation in several organs, including the CNS. This requires the breakdown of the blood-brain barrier.3-15 The factors involved in the development of these vascular changes are poorly known. B burgdorferi may directly activate the vascular endothelium to release several inflammatory cytokines, thus promoting recruitment of leucocytes to the vessel wall and perivascular tissues.16 17 The persistent local production of cytokines by endothelial cells and the recruited leucocytes may further accentuate vasculitis and perivasculitis. In agreement with this view, we have previously shown, using the polymerase chain reaction (PCR), that B burgdorferi exists in brain biopsy specimens with vasculitic lesions,15 and on the other hand, that peripheral blood mononuclear cells (PBMCs) of patients with disseminated Lyme borreliosis produce large amounts of interferon-γ (IFN-γ).18 Furthermore, human atherosclerotic abdominal aortic aneurysms have been shown to produce interleukin-6 (IL-6) and IFN-γ, which may play a part in the pathogenesis of various inflammatory vascular diseases.19Therefore, apart from the direct effects of spirochaetes on the vessel wall, cytokine production by endothelial and Th1 cells recruited to the vessel wall may be a pathogenetic mechanism leading to weakening of the inflamed vessel wall15 18 and thereby even to formation of aneurysms in patients with Lyme borreliosis.
We describe three patients with Lyme borreliosis and intracranial aneurysms. One of the patients had vasculitis diagnosed from a brain biopsy specimen. A single aneurysm was detected in all three patients.
Patients and methods
PATIENTS
All three patients were living in an area where Lyme borreliosis is endemic. They were examined at the Turku University Central Hospital.
ASSESSMENT OF BORRELIA ANTIBODIES
IgM and IgG antibodies against sonicated B burgdorferi were measured using an in house ELISA as previously described.15 Determination of intrathecal antibody production (Lyme Neuroborreliosis Kit; DAKO A/S, Glostrup, Denmark) was carried out only if antibodies were found in the CSF using the in house ELISA.
CULTURE AND POLYMERASE CHAIN REACTION (PCR) FOR B BURGDORFERI
The cultivation for B burgdorferi was carried out in BSK-II medium as previously described.15 Extraction of DNA for PCR was also according to our previous report.15 A 5 μl volume of extracted DNA was added to the reaction tube. The target chosen for PCR was a fragment from the flagellin gene of B burgdorferi. PCR was run as described earlier with primers WK1 and FL7, resulting in a 497 bp PCR product.20-22 Each PCR run included a positive control containing DNA extracted from a reference strain (B31) of B burgdorferi sensu stricto (ATCC 35210). Every sixth tube of each run was used as a negative control subjected to all the above sample treatments. The negative controls remained negative on each run. The sensitivity of PCR was found to be 10–100 B burgdorferi cells/reaction. The PCR test used was highly specific for B burgdorferi sensu lato. Other Borrelia species (B hermsii, B parkeri, and B turicatae) and treponemes (Treponema denticola, T pectinovorum, T socranskii, andT vincentii) gave negative results.
PROLIFERATION OF PERIPHERAL BLOOD MONONUCLEAR CELLS (PBMCS)
ThePBMCs were isolated and stimulated with heat killed B burgdorferi as previously described.18
NEUROPATHOLOGY
Surgical samples of patient 1 were processed as described previously.15
Results
Table 1 shows selected demographic data, symptoms, signs, and selected laboratory results. Table 2 shows laboratory results ofBorrelia tests in the three patients. The plasma or serum specimens of patients 1 and 2 contained DNA of B burgdorferi. In patients 1 and 2, a positive PCR result was obtained from more than one specimen taken and analysed at different times. Only patient 3 had serum antibodies as well as intrathecally produced CSF antibodies against B burgdorferi.
Selected demographic data, symptoms, signs, and non-specific laboratory findings in three patients with Lyme borreliosis and intracranial aneurysms
Laboratory results of borrelia tests and interval between onset of symptoms and antibiotic treatment of three patients with Lyme borreliosis associated with intracranial aneurysms
All three patients had intracranial aneurysms: in patients 1 and 2 the aneurysm was lying in the internal carotid arteries (in patient 2 it was mainly extracranial but extended intracranially) and in patient 3 it was in the basilar artery. The aneurysm ruptured in patients 1 and 3, causing subarachnoid haemorrhage. Brain MRI showed meningeal enhancement in patient 1 before but not after antibiotic therapy. Endovascular treatment of the aneurysm was carried out in patients 2 and 3. Perivascular or vasculitis associated lymphocytic inflammation was detected in the brain biopsy specimen available in patient 1. Detailed laboratory results and neuropathological description are included in the following case reports.
PATIENT 1
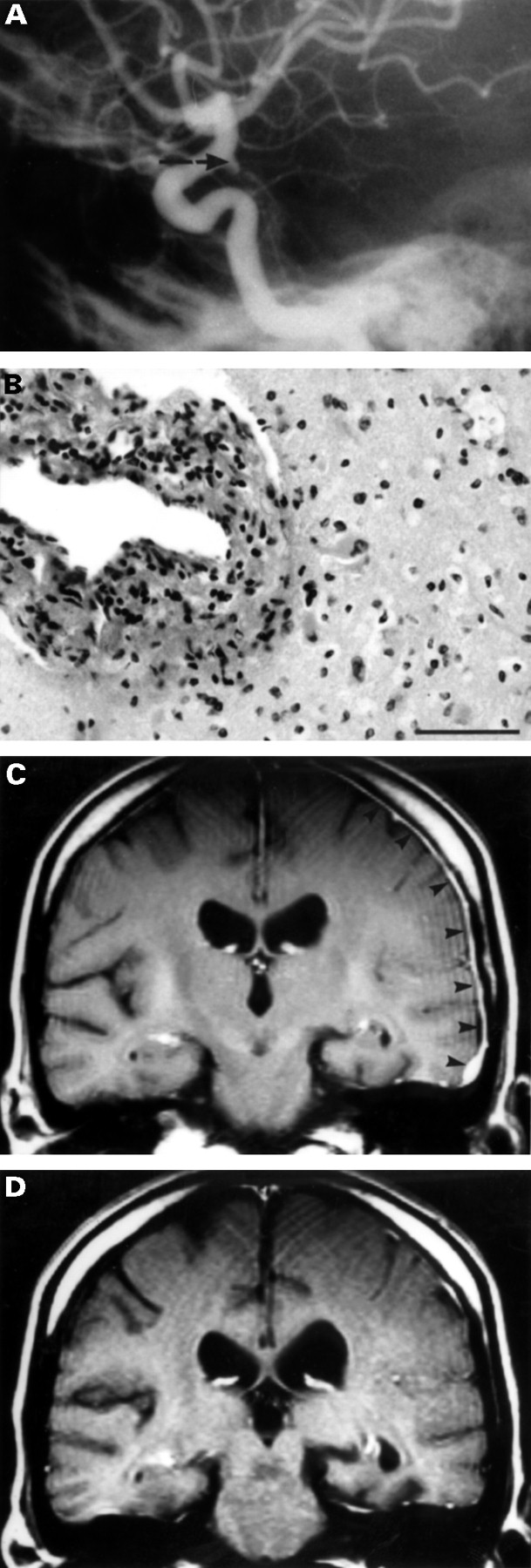
A previously healthy 43 year old woman was admitted to the hospital in December 1992 for intensive headache. Brain CT was suggestive of subarachnoid haemorrhage. She was referred to the Turku University Central Hospital, where cerebral angiography showed an aneurysm in the left internal carotid artery (fig 1 A). The aneurysm was clipped. After operation, the patient’s personality changed, and her speech mode became slow and dysarthritic. Pronounced inertia developed in her mental and motor performance. Her headache was not improved by the operation, and progressive memory impairment was also found. However, no other abnormalities were detected at neurological examination.

(A) Carotid angiography in patient 1 showing an aneurysm (arrow) in the left internal carotid artery in December 1992. (B) In the surgical brain specimen from a temporally located brain lesion suggestive of vascular damage or neoplasia, obtained in December 1993, the arterial wall is infiltrated by lymphocytes. In the surrounding parenchyma there is oedema and gemistocytic astrogliosis (haematoxylin and eosin, originally×280, bar= 500 μm). (C) In January 1994, pronounced dural gadolinium enhancement is shown (arrowheads) on T1 weighted MRI in the left frontal areas. (D) In September 1994, the enhancement of meninges had almost disappeared after treatment.
In October 1993, a brain MRI showed an abnormal lesion in the left temporal area, suggestive of vascular damage, although a slowly growing neoplasia could not be excluded. Craniotomy was carried out on 10 December 1993. Abnormal tissue and a change suggestive of neovascularisation were detected in the left temporal lobe. At histopathological examination, several arterioles with thickened vascular walls affected by fibrosis and pronounced perivascular lymphocytosis were seen, indicating chronic inflammation (fig 1B). In the surrounding white matter, an increased number of gemistocytic astrocytes was detected in a slightly oedematous parenchyma.
B burgdorferi DNA was amplified in two plasma specimens, obtained on 14 and 31 December 1993. Erythrocyte sedimentation rate was 3 mm/h, leucocytes 6.7×109/l, and thrombocytes 269×109/l. Serum antinuclear antibodies, tests for syphilis, and antibodies against HIV were negative. Antibodies againstB burgdorferi were negative in the serum and CSF. Leucocyte and protein concentrations in CSF were normal, and no oligoclonal bands were detected. PCR and culture for B burgdorferi from CSF and brain biopsy specimens were negative.
The patient was referred to a psychiatric hospital for paranoid psychosis. After positive results had been obtained on PCR amplification of B burgdorferi DNA in the plasma, the patient was referred back to the Turku University Central Hospital in January 1994. Her short term memory was very impaired, as she did not remember her previous hospital stay one month earlier. She also complained of a persistent headache and, despite antiepileptic therapy, had epileptic seizures with occasional episodes of severe memory loss and at times even loss of consciousness. In addition to postoperative changes in the left temporal area, MRI of the brain in the left frontal area showed pronounced meningeal enhancement that may have been caused by vasculitis, or simply by postoperative reaction (fig 1C). Antibiotic therapy with ceftriaxone (2 g intravenously daily) was instituted for two weeks and continued with amoxicillin (500 mg every eight hours) combined with probenecid (500 mg every eight hours) for 100 days. On 30 March 1994, PCR for B burgdorferi was negative in plasma samples.
In the spring of 1994, her headache much less severe. In September 1994, considerable improvement was shown by MRI of the brain. Most of the enhancement with gadolinium in the periventricular and frontal areas had disappeared (fig 1D). A CSF specimen (22 September 1994) showed no inflammatory cells or raised protein concentration. Culture and PCR for B burgdorferi, as well as antibody assays, were negative. The CSF Treponema pallidum hemagglutination test and PCR for M tuberculosis were negative. Serum antibodies against neutrophil cytoplasmic antigen as well as antinuclear and phospholipid antibodies were negative. The only abnormal laboratory result was detection of circulating immune complexes. After 1994, there are no records on this patient in the Turku University Central Hospital.
PATIENT 2
An 18 year old man presented with headache and progressive paresis of the right abducent nerve in April 1994. His brain MRI of June 1994 was normal. Serum antibodies against B burgdorferi were repeatedly negative and also antibodies against herpes viruses,Chlamydia pneumoniae, and Mycoplasma pneumoniae. Erythrocyte sedimentation rate was 1 mm/h, C reactive protein (CRP) <10 mg/l, leucocytes 5.9×109/l, and haemoglobin 157 g/l. Serum antinuclear antibodies and angiotensin converting enzyme were normal. On 22 June, CSF was normal (including antibodies against B burgdorferi and the ratio of IgG to albumin). DNA of B burgdorferi was found by PCR in plasma specimens obtained on 22 June and 26 August. In addition, the PBMCs of the patient proliferated after stimulation with B burgdorferi. In August 1994, an aneurysm was found behind the right orbit by CT. Magnetic resonance angiography (MRA) detected the same aneurysm, 2 cm in diameter, in the right internal carotid artery (fig 2A). This aneurysm was lying mainly extracranially but extended also intracranially compressing the lower part of cavernous sinus and the abducent nerve. However, infection with B burgdorferiwas also probable. Intravenous ceftriaxone given as 2 g daily for 14 days was instituted and followed by oral amoxicillin combined with probenecid (500 mg each every eight hours) for 100 days. In October 1994, endovascular occlusion of the aneurysm was carried out by embolisation. His headache disappeared gradually after the antibiotic treatment and endovascular treatment of the aneurysm, which was also shown to be successful by a control angiogram (fig 2B). At one year of follow up, the patient had made an almost complete recovery from the paresis.

(A) Magnetic resonance angiography of patient 2 showing an aneurysm with a diameter of 2 cm in the right internal carotid artery compressing the VIth cranial nerve and causing severe diplopia. (B) The same aneurysm showed by digital subtraction angiography after the endovascular embolisation.
PATIENT 3
A 42 year old woman with a presumptive diagnosis of erythema migrans (20 cm×10 cm) in her right lower leg in May 1994. Unaware of Lyme borreliosis, she did not seek medical attention although the rash slowly expanded and persisted until October 1994. She did not recall any tick bites. She gave a history of right sided peripheral facial nerve paresis in December 1989, and at that time a borderline level of serum IgG antibodies against B burgdorferi was detected. One month later, however, the antibodies were negative. Antibiotics were not prescribed, and she recovered from the paresis.
In January 1995, severe radicular pain developed first in the right leg, with no relief with anti-inflammatory drugs. After three weeks, the pain moved to the left leg. Again after three weeks, when both her legs were already symptomless, the pain moved to the back, first to the right and then to the left. After two weeks, her right arm began to ache in a way similar to that previously occurring in her legs. Again the pain moved from right to the left after two to three weeks. In April 1995, all radicular pain had disappeared.
On 22 February 1995, serum IgG antibodies against B burgdorferi were high (>6 SD above normal level) and IgM antibodies were at a borderline level. A similar very high level of IgG antibodies was detected against B burgdorferi flagellin. On 21 April 1995, examination of CSF disclosed 5 ×106/l leucocytes (no erythrocytes), and the protein content was also at the upper limit of the normal range, 619 mg/l. The ratio IgG to albumin in the CSF was normal, as was the IgG index. Intrathecal production of IgG antibodies against B burgdorferi was detected with an index of 1.50. PCR for B burgdorferi DNA in the CSF and plasma specimens was negative, and so was the venereal disease research laboratory test. Erythrocyte sedimentation rate was 7 mm/h, CRP<10 mg/l, haemoglobin 142 g/l, leucocytes 7.0×109/l, and thrombocytes 227×109/l. Blood pressure was 160/95 mm Hg.
On 25 May 1995, intravenous ceftriaxone (2 g) daily was instituted for 14 days and followed by oral amoxicillin (500 mg) combined with probenecid (500 mg) three times daily each for 100 days. In December 1995, serum IgG antibodies against B burgdorferi had decreased and were now at a moderate level. At a follow up visit in June 1996, she gave a recent history of headache lasting for a few weeks in January and April 1996. In addition, she had had temporary radicular pain in her left arm. She had also had mild arthralgias and temporary dyspnoea. Her blood pressure was 180/100 mm Hg, and she was advised to attend regular blood pressure check ups. The results of a neurological examination were normal. Lumbar puncture was carried out in June 1996. The CSF showed 0 erythrocytes, 4–5×106/l leucocytes, normal protein, and negative borrelia antibodies as well as negative PCR and culture for B burgdorferi. Serum IgG antibodies against B burgdorferi were now at the lower borderline level, suggesting eradication of the spirochaete.
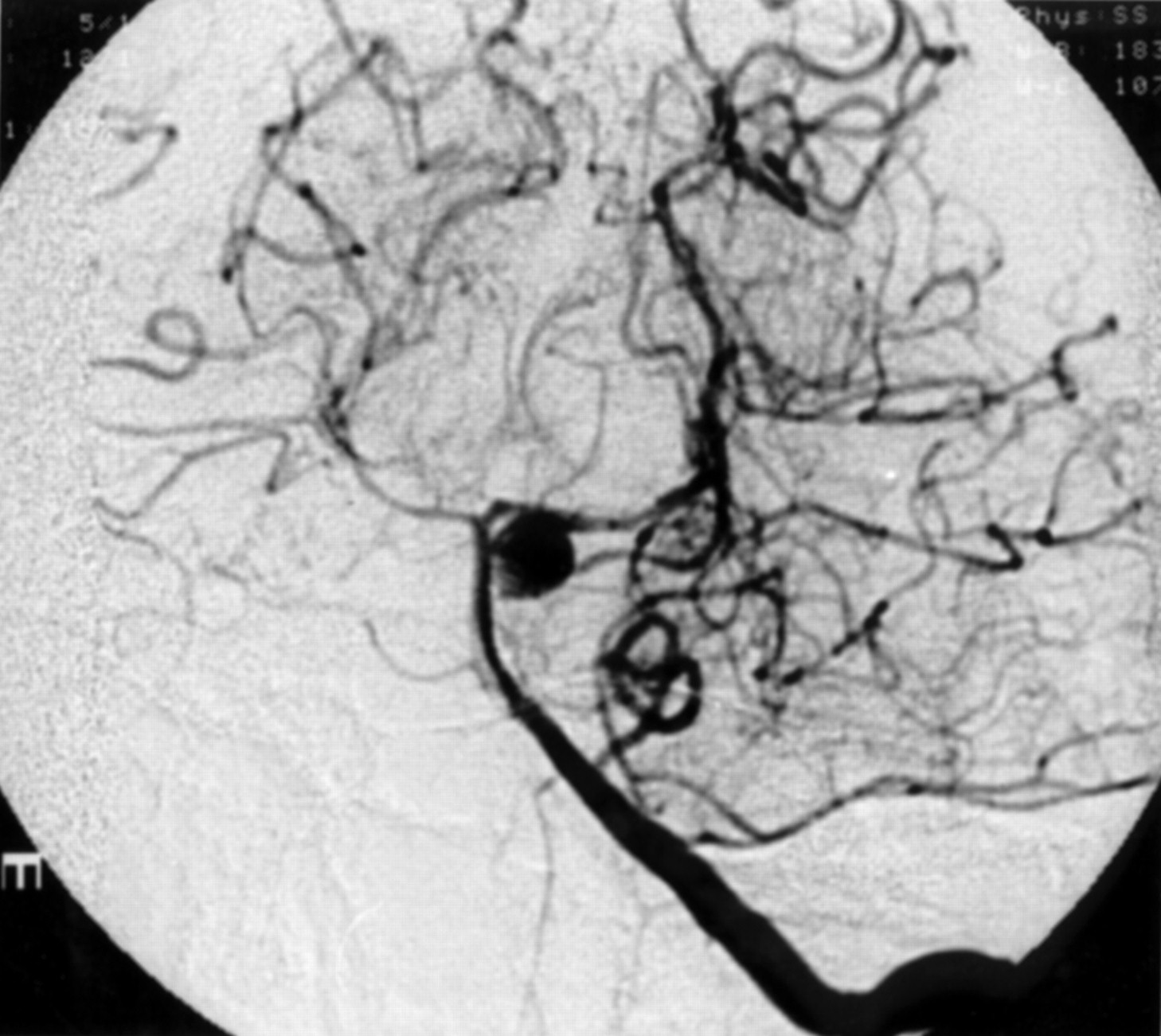
On 27 July 1996, she was admitted to the hospital for sudden and severe headache and unconsciousness. In the emergency room, convulsions were noted and subarachnoid haemorrhage was detected by CT. She soon recovered consciousness. Angiography showed an aneurysm, diameter 1 cm, arising from the basilar artery near the bifurcation of the left superior cerebellar artery (fig 3). On 1 August 1996, endovascular occlusion of the aneurysm was carried out by embolisation. After a normal recovery, a control angiogram showed that the aneurysm had been embolised successfully.

{kind=link}
{kind=link}
{kind=link}
Digital subtraction angiography showing an aneurysm with a diameter of 1 cm in the basilar artery of patient 3 near the bifurcation of the left superior cerebellar artery.
Discussion
This study presents three patients with Lyme borreliosis associated with an intracranial aneurysm. In patient 1, surgical brain specimens were available, disclosing vasculitis or perivascular inflammation. Aneurysm formation of arteries may be due to vasculitic damage, endarteritis obliterans of the vasa vasorum in the vessel wall.1 Spirochaetes are known to cause vasculitis, and chronic T pallidum infection has been causally related to aneurysms.1 This may also apply to B burgdorferi, because coronary artery aneurysms have been recently reported in two patients as a complication of serologically established Lyme borreliosis.2 Our study is the first to associate cerebral artery aneurysms and subarachnoid haemorrhage with Lyme borreliosis. Additionally, we showed an ongoing infection withB burgdorferi by PCR from plasma in patients 1 and 2 with ruptured aneurysms. However, the causal relation of aneurysms with this spirochaetal infection could not be confirmed, as it was not possible to carry out a histological or microbiological study of the walls of the aneurysms in any of our patients.
The prevalence of intracranial aneurysms in the general population has been given as 0.2–9% in various postmortem series, depending on whether aneurysms were searched for or merely recorded as incidental findings.23 The annual incidence of subarachnoid haemorrhage from confirmed intracranial aneurysms is slightly above 10/100 000 in Finland.23 Epidemiological evidence suggests that the great majority of saccular intracranial aneurysms (commonly referred to as berry aneurysms) do not develop until adulthood.23 Although some aneurysms are due to congenital defects in the vessel wall, most seem to result from an acquired degenerative process in the arterial wall. However, a considerable proportion of the cases may be familial.24 The familial cases may be due to genetic and possibly also to additional environmental factors, including infections. One of the degenerative processes in the vessel wall is atherosclerosis, which is increasingly regarded as an inflammatory process.23 25 26Furthermore, high numbers of inflammatory cells have been found at the site of rupture of human berry aneurysms, suggesting that inflammation may contribute to the yielding of the aneurysm.26
The intracranial aneurysms and subarachnoid haemorrhages in our patients with concomitant or recently treated Lyme borreliosis may be purely coincidental findings. The prevalence of antibodies againstB burgdorferi in our area including the archipelago (but excluding the Åland Islands) has been investigated (unpublished observations). In randomly chosen inhabitants (n=750) the prevalence was 6% using a cut off of +2 SD above the mean of the previous normal control material (obtained from different parts of Finland) and 2% using a cut off of +4 SD. Based on these numbers, it is possible but unlikely, that the concomitant intracranial aneurysms and Lyme borreliosis occurred by chance in these three patients. Furthermore, the aneurysms were not the only manifestation in our patients, indicating a closer, possibly common causal association of the aneurysms with other symptoms and findings. Patient 1 had neurological as well as psychomotor signs and symptoms that could not be considered to be complications of the aneurysm or subarachnoid haemorrhage. Patient 3 was treated with long term antibiotics for migrating radiculitis due to Lyme borreliosis, and at follow up visits she reported intensive headaches months before the rupture of her intracranial aneurysm.
Recent findings indicate that B burgdorferi can acquire proteolytically active host components.27 This mechanism could facilitate the dissemination and adhesion of the spirochaetes to sites of endothelial injury. Interaction between the intraluminal endothelial surface and the spirochaete, directly or via generalised or focal production of cytokines, has been found necessary to increase the permeability of the blood-brain barrier.10 Our findings support our earlier suggestions and those of others that vasculitis may be one of the primary pathophysiological mechanisms in Lyme borreliosis.3-15 28 29
Vasculitis is a predominant finding in T palliduminfection.1 30 In meningovascular syphilis, obliterative endarteritis may cause multiple small infarctions in the CNS or involve the vasa vasorum of large or medium sized vessels and lead to aneurysms or ischaemic infarction months or years after onset of infection.1 30 31 The immune pathogenesis of cardiovascular syphilis has remained controversial. Focal inflammation or infection in the vessel wall by spirochaetes may be a pathogenetic mechanism leading to the formation of an aneurysm. Intracranial aneurysms in our patients with Lyme borreliosis, as well as the case of a patient with Lyme borreliosis and brain MRI showing meningeal enhancement, may indicate that mechanisms similar to syphilis are possible in Lyme borreliosis.
The diagnosis of Lyme borreliosis has usually been based on non-specific findings, serological testing, and other indirect methods. Our patient 3 was the only one with serum antibodies or intrathecal production of borrelial antibodies in the CSF. There are three plausible explanations for the lack of antibody production in Lyme borreliosis. Firstly, recent studies with T cell clones and patients with disseminated Lyme borreliosis suggest that B burgdorferi may shift the immune response of the host towards cell mediated immunity at the expense of antibody production.18 32 An association between PCR positivity and the absence of a serological response in Lyme borreliosis has been suggested.33 34 Secondly, the binding of antibodies to immune complexes may make antibodies undetectable by routine assays.35 Thirdly, the CNS can be considered an immunoprivileged site where the spirochaete can lie latent out of reach of the host immune system.36-38
The presence of B burgdorferi was repeatedly shown by PCR in plasma specimens in patients 1 and 2. We consider our PCR results reliable, because contamination control was rigorous and all control specimens gave negative results. A few spirochaetes or their structures may occasionally circulate in the blood not only in early infection but also during the later stages of Lyme borreliosis.33 39-43 Thus MRI, MRA, or carotid angiography findings compatible with aneurysm or vasculitis in association with a positive PCR result from the CSF or plasma, even without direct demonstration of the spirochaete in the vessel wall, might be an indication for antimicrobial treatment against B burgdorferi.
A recent study showed that the dura can be affected in the rhesus macaque experimentally infected with B burgdorferi.44 This is in agreement with the results of our MRI studies showing pronounced dural enhancement with contrast medium in patient 1. This patient also had epileptic seizures. Epilepsy induced by Lyme borreliosis has been reported recently.15 45 46 The incidence of seizures in neurosyphilis ranges from 14% to 60%.47 There is circumstantial evidence that Lyme borreliosis may cause psychiatric symptoms.48 In the case of patient 1, who had personality changes and pronounced memory impairment and needed psychiatric hospital care, a causal relation between CNS lesions and psychiatric manifestations is possible. Patients with chronic Lyme borreliosis encephalopathy may have multifocally reduced blood perfusion to the cerebral hemispheres, particularly in white matter, and objective improvement in brain perfusion after antibiotic treatment can occur.49 The causative role of borrelial infection with the CNS findings and neurological symptoms was supported by disappearance of the dural enhancement in patient 1 and by improvement of clinical condition in all patients after antimicrobial therapy directed against B burgdorferi.
We conclude that lymphocytic vasculitis associated with B burgdorferi infection may be a pathogenetic mechanism for intracranial aneurysms.
Acknowledgments
This study was financially supported by The Emil Aaltonen Foundation, The Maud Kuistila Foundation, The Orion Corporation Research Foundation, The Turku University Foundation, and The Finnish Medical Foundation. The language of this manuscript was revised by Simo Merne.