Article Text

Abstract
Background: Traumatic stroke usually occurs after dissection of large extracranial or intracranial vessels, leading to disseminated cerebral embolism. Stretching and distorting forces in cerebral intraparenchymal end arteries can cause intimal lesions followed by an occluding thrombus.
Objective: To investigate the importance of traumatic endothelial lesions in intraparenchymal end arteries after minor head injuries.
Methods: The cases of eight children are reported. They were aged between two and seven years (mean 6.2 years), and they developed significant neurological deficits at 15 minutes to 72 hours (mean 16.3 hours) after minor head injuries.
Results: The the patients all had hemiparesis combined with other signs, including central facial paralysis, dysphasia, dysphagia, and extrapyramidal signs. Computed tomography or magnetic resonance imaging showed cerebral infarctions affecting branches of the middle cerebral artery (n = 3), anterior cerebral artery (n = 1), posterior cerebral artery (n = 1), and basilar artery (n = 3). These lesions affected the basal ganglia, the internal capsule, and the brain stem. Neither heart disease nor dissections of large vessels were present. Two children had prothrombotic risk factors (an increase in lipoprotein (a) and a factor V Leiden mutation). The follow up period was between three months and 13 years (mean 3.9 years). Outcome was classified according to the Glasgow outcome scale as moderate disability (n = 4), severe disability (n = 2), non-disabling sequelae (n = 1), and total recovery (n = 1).
Conclusions: Minor head injuries can be cause and co-factor in the aetiology of stroke. The frequency of this may be underestimated, and detailed medical history of the days before stroke manifestation may identify more traumatic events, especially in the group of so called “idiopathic” strokes.
- stroke
- minor traumatic head injury
- hemiparesis
- child
Statistics from Altmetric.com
In head injuries, the connection between the underlying brain injury and neurological symptoms is usually rapid and obvious, and the severity of the trauma correlates with the clinical symptoms. Minor head injuries—mostly brain concussion—are common accidents and usually cause no severe complications. The cases reported here are characterised by inappropriately severe neurological deficits following minor head injuries, reflecting arterial infarcts in small vessel territories.
MATERIALS
We made a retrospective assessment of the clinical data on eight children aged between two and seven years (mean 6.2 years). These children were seen in the department of paediatric neurology of Frankfurt University between 1973 and 1999, partially during the acute phase of the injury or for an expert medical opinion.
There were five boys and three girls All were previously healthy and had no history of neurological or haematological diseases. The topography of the intracerebral lesions was defined by computed tomography (CT) and magnetic resonance imaging (MRI). Sources of possible embolisation (large vessel dissections), vessel malformations, and large vessel diseases were excluded by precordial, cervical, and transcranial Doppler ultrasound and angiography. Investigations of prothrombotic risk factors were performed to a varying degree. Mean follow up was 3.9 years. Outcome was assessed by the Glasgow outcome scale.1
Case reports
Patient 1
A boy aged 3 years and 8 months fell from a height of approximately 120 cm head first on to frozen ground, after which he was drowsy and and complained of a headache; 20 hours later he developed weakness of the right arm and leg, accompanied by tremor of the right arm. Six days later a CT scan showed a 7 × 6 mm hypodense lesion in the left dorsal internal capsule. A control CT scan 1.5 years later still showed the lesion. The ischaemic area affected the thalamogeniculate arteries of the posterior cerebral artery. Four and a half years later the boy still had a spastic hemiparesis of the right side, which was graded as a moderate disability according to the Glasgow outcome scale.
Patient 2
A boy aged 4 years and 9 months ran headlong into a door. He cried immediately and after some consolation fell asleep in the arms of the kindergarten teacher. Four hours later he developed a left facial paralysis and after a further four hours, a left hemiparesis. MRI on the same day showed discrete non-homogeneous T2 hyperintensity in the right basal ganglia region. The next day a CT scan showed a 1.5 × 2.5 cm ischaemic lesion which included medial parts of the caudate nucleus, globus pallidus, and anterior and medial parts of the internal capsule.
One month later MRI confirmed a large ischaemic right basal ganglia lesion in the supply area of the recurrent artery of Heubner, originating from the anterior cerebral artery but possibly also involving lenticulostriate artery branches. The hemiparesis improved somewhat during the following three months, and was graded as moderate disability. One year later this boy developed a second, now non-traumatic, stroke affecting the right middle cerebral artery, with massive deterioration of the left sided hemiparesis resulting in severe disability. Investigation for coagulation disorders showed increased lipoprotein (a) of 34 mg/dl, with kringle 4 polymorphism in the apolipoprotein (a) gene as a prothrombotic risk factor.
Patient 3
A girl aged 7 years and 8 months fell and hit her head on asphalt while rollerskating. Immediately afterwards she felt dizzy and vomited. Three days later she developed a left sided spastic hemiparesis. MRI showed T2 hyperintensity in the right anterior internal and external capsule and anterior parts of the putamen, associated with an ischaemic lesion of the right lateral lenticulostriate arteries originating from the middle cerebral artery. Nine months later a residual spastic hemiparesis caused moderate disability.
Patient 4
A boy aged 6 years and 1 month ran headlong against a bar and hit the back of his head on the ground. He felt nauseous and vomited after some minutes. Six hours later he developed a left facial paralysis and was unable to walk. An initial CT scan showed no abnormalities, but 14 days later MRI showed a T2 increased intensity in the inferior pons. The lesion contained dots suggesting haemosiderin deposition caused by a haemorrhagic infarct of the perforating vessels originating from the basilar artery. The facial paralysis and the hemiparesis improved during the following 10 days, and his walking improved as well. At a three month follow up he was moderately disabled.
Patient 5
A girl aged 7 years and 7 months fell head first on to the ground while playing in the schoolyard. She started vomiting immediately and was confused. On clinical examination she showed no neurological abnormalities except for a bilaterally positive Babinski sign. Twelve hours later a right facial paralysis and hemiparesis developed, and after a further 14 days she began to have tremor of the right hand and dystonic movements of the right foot. Three years after the accident, a CT scan showed a 1.0 × 2.5 cm hypodense area in the left putamen indicating an infarct of the lenticulostriate arteries of the middle cerebral artery. At follow up 1.5 years after the accident the girl still had a right hemiparesis with torsion dystonia, circumdicting movements, increased muscle tone, and central facial paralysis. Two years later she developed rigor, dystonia, and spasticity in the right foot. After three years of follow up she remained severely disabled.
Patient 6
A boy aged 7 years and 7 months was pushed off a climbing frame approximately two metres high by another boy. He hit the back of his head against the lowest metal rung. He was unconscious for a few seconds and was then disorientated and complaining of a headache for some minutes. Eight hours after the accident his mother noticed a right facial paralysis and hemiparesis accompanied by dysphasia. Immediate cerebral CT showed no abnormalities. Thirteen days after the accident, MRI showed an 8 × 12 mm ischaemic lesion in the caudal left pons region caused by an occlusion of a paramedian perforating branch of the basilar artery entering the caudal rostral brain stem. Four years later MRI showed a 4 × 7 mm cystic lesion in the left caudal pons region. Thirteen years later the boy passed his school leaving examinations and was able to play ice hockey, though with mild neurological signs of hemiparesis, classified as non-disabling.
Patient 7
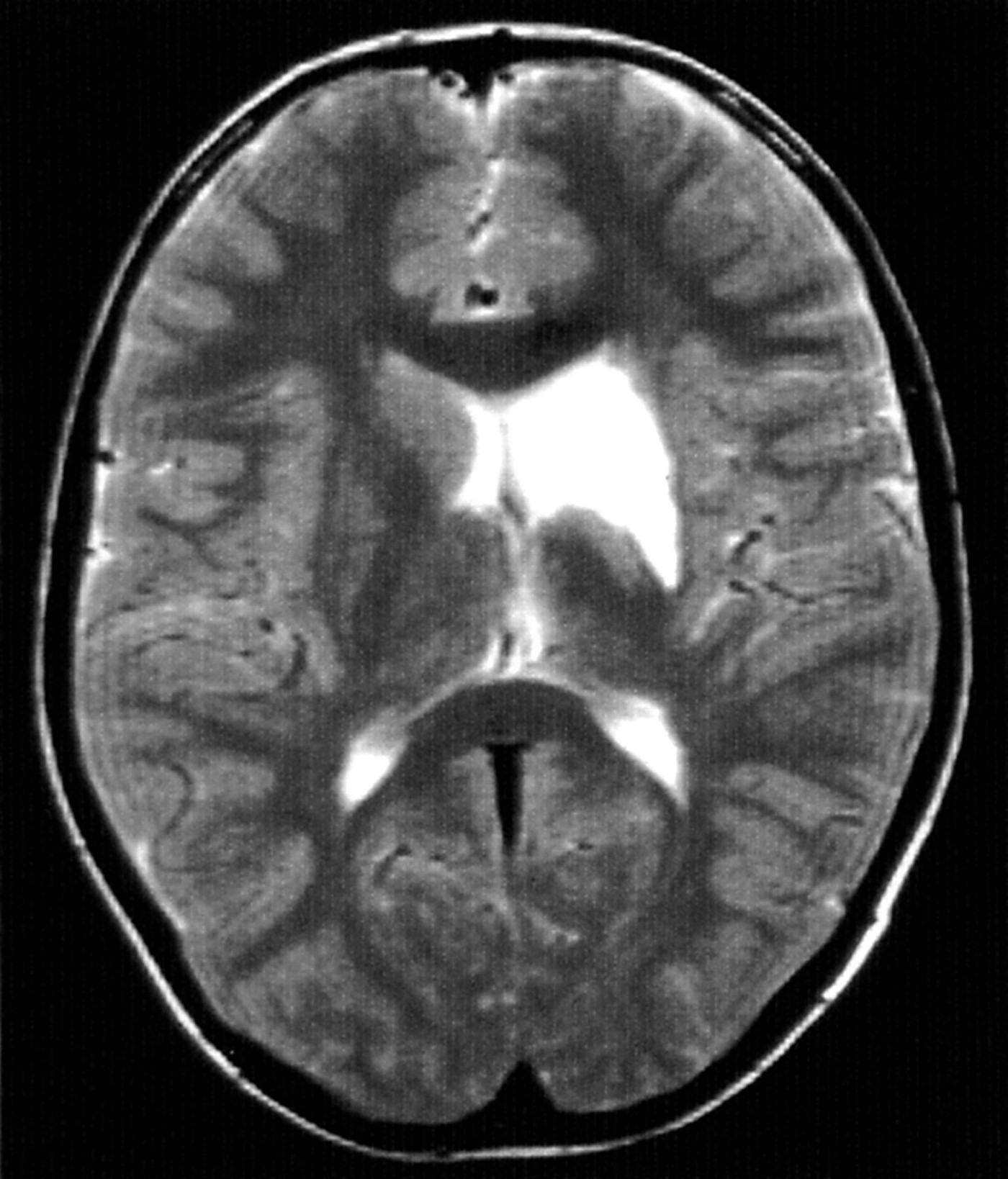
A girl aged 2 years and 7 months fell from a height of 60 cm head first out of bed on to a carpeted floor, cried for 10 minutes, and then fell asleep again. The next morning, eight hours later, she developed dysphasia, dysphagia, right facial paralysis, and mild right hemiparesis. Cerebral CT showed a hypodense 4 × 6 mm lesion in the left pons. Two weeks later MRI confirmed this ischaemic lesion in the caudal left pontine region, reflecting to an occlusion of a paramedian perforating branch of the basilar artery entering the brain stem. The neurological symptoms diminished over the following four weeks. A little over eight years later, neurological examination showed no signs of hemiparesis (total recovery), while MRI still showed a residual lesion of the left pontine region (fig 1).

Transverse T2 weighted magnetic resonance tomography, showing a postischaemic lesion in the left pontine area in patient 7.
Patient 8
A boy aged six years collided head on with another child while playing. He cried initially and 15 minutes later he fainted and developed a right sided hemiparesis, aphasia, and facial paralysis. Immediate cerebral CT showed no abnormalities. On the following day, MRI revealed an infarct of the left striatum caused by damage to the lenticulostriatal branches of the left middle cerebral artery (fig 2). His neurological symptoms improved during the following months. MRI after eight months showed that the lesion in the left basal ganglia was unchanged. On neurological examination he had a moderate disability caused by residual hemiparesis. Coagulation tests showed increased activated protein C (APC) resistance (ratio 1.32), and on genetic analysis he was found to have a heterozygous factor V Leiden mutation G1691A.
{kind=link}
{kind=link}
Transverse T2 weighted magnetic resonance tomography, showing a postischaemic lesion in the left striatal area in patient 8.
Clinical features and pathology
All eight children had a so called minor head injury without skull fracture. The mechanism of accident was a fall in five cases, and in three cases there was a combination of crushing against an object and falling to the ground (table 1). Primary symptoms were compatible with brain concussion, mainly vomiting, weariness and cephalgia. Only one child had initial vertigo and two a short period of disturbed consciousness.
General data on the patients
The latency period between the accident and the development of focal neurological symptoms varied between 15 minutes and 72 hours, with a mean of 16.3 hours. All children developed hemiparesis. This was accompanied by central facial paralysis in six, dysphasia in three, and dysphagia in one. One girl developed a severe hemiparetic dystonia caused by a lesion in the putamen. CT or MRI showed focal lesions of the basal ganglia in five and of the brain stem/pons region in three. Apart from one patient with a haemorrhagic-ischaemic lesion, the lesions were solely of ischaemic origin. In three children the infarct affected the lenticulostriate branches of the middle cerebral artery, in one case the Heubner artery originating from the anterior cerebral artery, in another the thalamo-geniculate branches of the posterior cerebral artery; in three cases the vessels affected were the perforating branches of the basilar artery. Sources of possible embolisation were excluded by Doppler ultrasound and angiography.
The follow up period for these eight children varied between three months and 13 years, with a mean of 3.9 years. Most of the children had residual sequelae in the form of hemiparesis of different degrees. On the Glasgow outcome scale, four children remained moderately disabled, two were severe disabled, one had non-disabling sequelae, and one made a total recovery. Depending on the year of the accident, diagnostic procedures for prothrombotic risk factors were performed to a varying degree. Patient 2 had an increased lipoprotein (a), and this boy developed a second ipselateral non-traumatic stroke one year later. Patient 8 had a factor V G1691A (Leiden) mutation.
DISCUSSION
Endothelial lesions play a major role in the development of ischaemic or haemorrhagic vascular occlusion. Dissection of large extracranial or intracranial vessels such as the carotid artery or the vertebral artery, with disseminated cerebral embolism, can occur after traumatic or even sporadic hyperextension of the proximal cervical spine.2 Diffuse vascular lesions after severe head injuries, especially ones affecting the corpus callosum and the white matter, are quite common and are caused by acceleration-deceleration shearing forces at intraparenchymal borders. They are described as diffuse axonal injuries.3 In our cases the affected vessels were small end arteries leaving their originating vessels (basilar artery and middle, anterior, or posterior cerebral artery) almost at right angles to perforate the brain parenchyma. The angle at which the perforating branches arise from the middle cerebral artery varies with age.4,5 Children are particularly vulnerable to translating, stretching, and distorting forces, which can be imposed by even minor head injuries. The impact on the skull causes an opposing movement of the brain parenchyma, with stretching and shearing effects on the vessels because of the high moment of inertia. This leads to a traumatic endothelial intimal lesion, followed by fibrin accumulation, leucocyte reaction, and the formation of a white thrombus occluding the lumen. This vessel obstruction causes ischaemia of cerebral parenchyma with clinical symptoms after a symptomless latency period.6
Maki et al described four paediatric patients with basal ganglia lesions following minor head injuries, after latencies of between 15 minutes and 16 days.7 They found that when the stretching force was severe, rupture of the entire thickness of the vessel resulted, which led to an acute haemorrhage, while a milder stretch gave rise only to endothelial rupture. The shearing force in a child's brain seems to be stronger than in adult's brain because of the elasticity of the skull vault. Brett et al reported a five year old girl who developed a hemidystonia, comparable with our patient 5, secondary to an infarction of the putamen and posterior limb of the internal capsule five days after a mild head injury.8
Demierre and Rondot9 described a three year old boy who developed a dystonic hemiparesis with dysarthria caused by an ischaemic lesion involving the head of the left caudate nucleus, the putamen, and the anterior limb of the internal capsule, two days after a minor head injury. Dharker et al reported 23 children below the age of 6.5 years who developed immediate unilateral weakness after apparently minor head injuries, accompanied by hypodense CT lesions in the basal ganglia.10 All but one of these children recovered completely within four months. Trauma is of course very common in childhood, and in the absence of data from case–control studies it is possible that in some of the reported cases the association with recent trauma may have been coincidental.
Stroke in childhood is a rare condition with an estimated incidence of 1–13/100 000.11,12 It is considered to be a multifactorial problem with a multifactorial aetiology. Common conditions predisposing to stroke include embolism associated with congenital or acquired heart disease, or arterial malformations as in the Ehlers–Danlos syndrome and fibromuscular dysplasia. Further risk factors are sickle cell disease, dehydration, meningitis, varicella infection, acquired immunodeficiency syndrome, homocystinuria, mitochondriopathy (MELAS), and haemolytic-uraemic syndrome.13,14 The role of prothrombotic risk factors as predisposing factors for stroke is unknown. The most common prothrombotic risk factors found in children with stroke are factor V G1691A (Leiden) mutation, protein C deficiency, and prothrombin mutation G20210A.14–17 Further relevant prothrombotic risk factors are protein S deficiency, antithrombin III deficiency, heparin cofactor II, histidine-rich glycoprotein, dysfibrinogenaemia, plasminogen deficiency, plasminogen activator inhibitor (PAI) deficiency, lipoprotein (a), factors II, VII, XII, VIII, von Willebrand factor, antiphospholipid syndrome, and hyperlipidaemia.13,14,15,18
One of our patients had raised lipoprotein (a) with kringle 4 polymorphism in the apolipoprotein (a) gene, and another had a factor V G1691A mutation. In a symptomless paediatric control group (n = 150), the prevalence of this mutation was 4.7%.15 In our two patients with proven prothrombotic risk factors, the minor head injury had the implication of a co-factor in the pathogenesis of stroke. In the other six children we assume that the shearing of the small end arterial vessels was responsible for the stroke. Children are at higher risk of this than adults, and in view of the risk of relapse and the possible need to initiate antithrombotic prophylaxis, diagnostic investigations for coagulation abnormalities are mandatory. Large vessel dissection must also be excluded. Perhaps the frequency of this shearing mechanism in minor head injuries is underestimated, and a detailed medical history of the days preceeding the stroke manifestations may identify more traumatic events, particularly in the group of so called “idiopathic” strokes.