Seasonality and the sudden infant death syndrome during 1987-9 and 1991-3 in Australia and Britain
BMJ 1996; 312 doi: https://doi.org/10.1136/bmj.312.7043.1381 (Published 01 June 1996) Cite this as: BMJ 1996;312:1381
- A S Douglas, emeritus professor of medicinea,
- T M Allan, retired assistant director, blood transfusion serviceb,
- P J Helms, professor of child healthc
- a Department of Medicine and Therapeutics, University of Aberdeen Medical School, Foresterhill, Aberdeen AB9 2ZD
- b Wellcome Research Library, University of Aberdeen Medical School
- c Department of Child Health, University of Aberdeen Medical School
- Correspondence to: Professor Douglas.
- Accepted 29 February 1996
Abstract
Objective: To determine whether seasonality of the sudden infant death syndrome persists now that rates have fallen, mostly after widespread adoption of the “face upwards” sleeping position.
Design: Monthly data on the sudden infant death syndrome during 1987-9 were compared for seasonality with those of 1991-3; rates were studied as deaths per 1000 live births.
Setting: Australia and Britain (England, Wales, and Scotland).
Subjects: Infants under 1 year dying of the syndrome (2401 for Australia and 6630 for Britain).
Main outcome measure: Extent of seasonal variation (amplitude) was established by cosinor analysis; amplitudes for the earlier and later years were compared.
Results: The rate fell in every month, and, though it did so relatively more in winter than summer, seasonality remained a distinctive feature. In the comparison of amplitudes the ratio between the earlier and later years was 1.4 in both Australia and Britain. Some differences between the hemispheres were noted.
Conclusions: Seasonality of the sudden infant death syndrome remains to be explained and continues to be an important aetiological lead. Studies from other countries are needed.
Key messages
Analysis of two large series has shown that seasonal variation in incidence persists but has been reduced by about one quarter
Seasonal variation is an unexplained epidemiological feature with the potential to be an important clue to aetiology
Introduction
The seasonality of sudden infant death syndrome was reported in 1855 by Wakley1 and in 1944 by Abramson,2 who was also the first to demonstrate the advantage of the “face upwards” sleeping position. The reappreciation and recommendation of this position3 4 5 6 7 8 has been followed by a dramatic fall in incidence, after an earlier period of more gradual decline,9 perhaps from other changes in infant care practice, such as avoidance of overwrapping and of exposure to cigarette smoke. Researchers in Australasia10 11 and in Britain12 13 have reported that this more recent fall has been predominantly in winter. We re-evaluated this conclusion by using two large series and including data for 1993—that is, after the precipitous part of the fall had occurred.
Material and methods
Monthly data on the sudden infant death syndrome (International Classification of Diseases, 9th revision (ICD-9) code 798.0) were obtained from the Office of Population Censuses and Surveys (now the Office for National Statistics) for England and Wales and the General Register Office for Scotland, these being here combined as data for Britain.
The periods 1987-9 and 1991-3 were compared to examine seasonality before and after 1990. Data for 1990 are also shown, but that year was treated as an arbitrary watershed between the slow9 and rapid declines in incidence of the syndrome. The sexes were combined, and the monthly rates of the syndrome per 1000 live births were established. Deaths in the first month of life were included. The main conclusions were drawn from the aggregated years, but data are also provided on single years.
Cosinor analysis14 15 16 17 was used to assess seasonality. This technique is reliable provided that the data fit a single sine curve; the best fit of a cosine function curve to annual data is then calculated. In this analysis the year is taken as 360°, and the midpoint of each month of the year is assigned an angular value t for January (15°) through to December (345°). Multiple regression analysis is completed between monthly data and sine (t) and cos (t). This analysis gives the multiple correlation coefficient (r) its significance (P) and its angular position in the year where the fitted sinusoidal regression line has its highest value.
Monthly data were corrected to a 31 day month. The mean monthly value was calculated and given a value of 100%. Individual values were expressed as a percentage above and below the mean. The extent of the seasonal fluctuation (amplitude A) was measured as the percentage above the mean for the highest value of the sine curve (the acrophase). The amplitude expressed in this way is therefore half of the total seasonal fluctuation. This technique imposes a single sine curve on the data, the nadir coming six months after the peak (acrophase). The term significance relates here to the presence or absence of seasonality, and 95% confidence limits are established. (These features are illustrated in the figures.)
Results
The monthly rates for the earlier and later years in both countries are shown in figure 1 and table 1. The well known general seasonality is seen in figure 1.

Sudden infant death syndrome in Britain and Australia, 1987-9 and 1991-3. Incidence in 1987-9 (*) compared with that in 1991-3 (*) in both countries. Discontinuous lines indicate 95% confidence intervals. Discontinuous horizontal line gives mean values. A=amplitude
{kind=link}
Rates of sudden infant death syndrome and percentage fall in incidence between 1987-9 and 1991-3 for Britain and Australia
Figure 1 shows that seasonality was sustained in the later years but at a lower amplitude. The amplitude fell from 45% to 32% in Britain and from 35% to 26% in Australia, leaving a substantial seasonal difference. The ratio of amplitudes of earlier to later years was 1.4 in both countries. The cosinor analysis (fig 1) gives r values for the United Kingdom of 0.98 for 1987-9 and 0.95 for 1991-3 and for Australia of 0.90 for 1987-9 and 0.94 for 1991-3. All P values are <0.001. By changing the scaling on the ordinate in figure 2 the persistence of the seasonality in 1991-3 is made clearer.
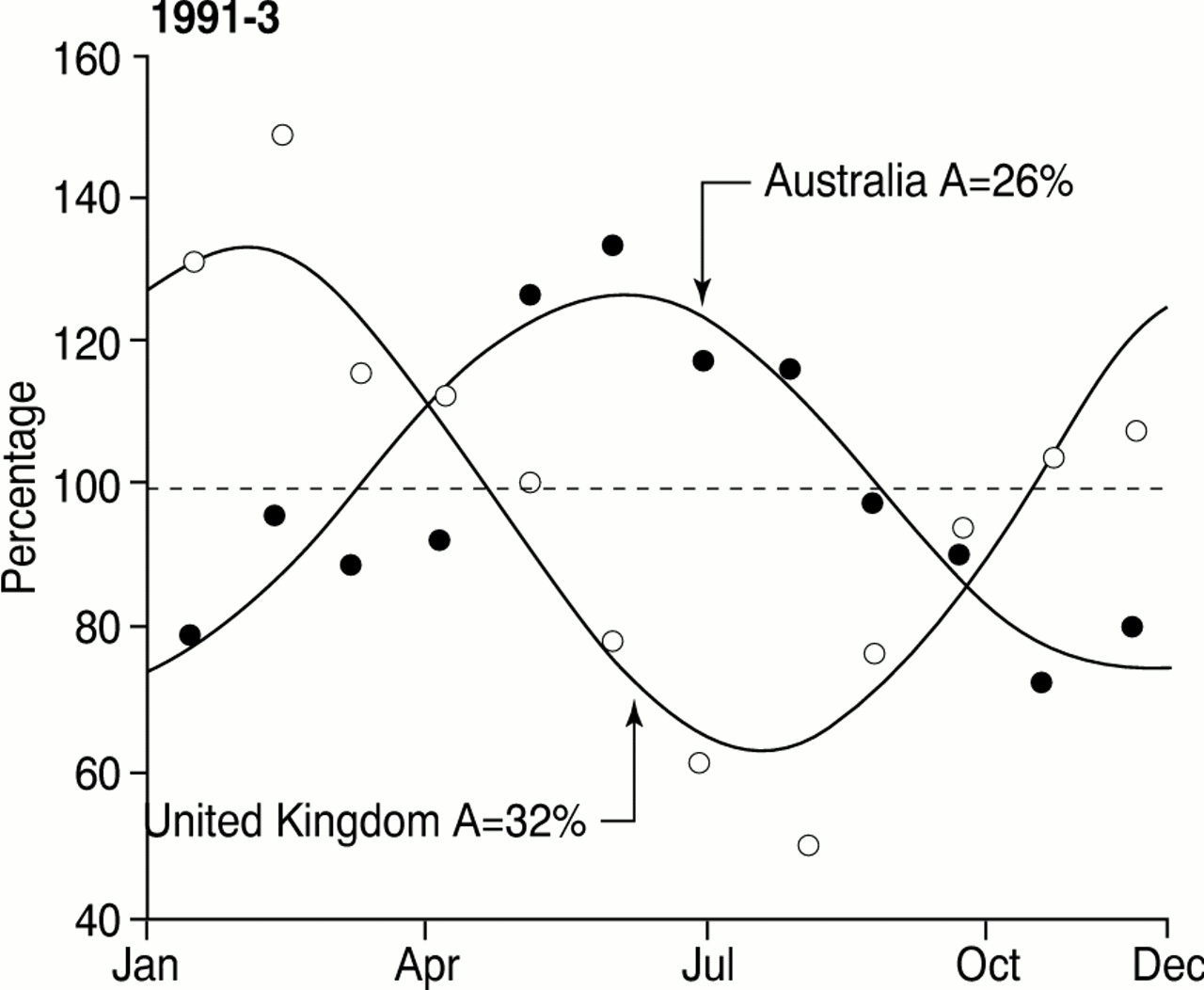
Sudden infant death syndrome in Britain and Australia, 1991-3 only. Ordinate shows a scaling in percentages above and below the mean. This figure provides clearer visual presentation of continuing seasonality during 1991-3, the scale on the ordinate being altered. Discontinuous horizontal line shows mean value. A=amplitude
{kind=link}
The main conclusions have been drawn from the aggregated data, and this can be criticised as blurring the effects by averaging the trend over three years. Accordingly single year results are also given (table 2). The incidence of the sudden infant death syndrome had been falling for some years up to 1990,9 but soon thereafter there was a dramatic fall, usually ascribed to the campaign to have babies placed in the face upwards sleeping position. The campaign for this in Britain started in the autumn of 1991 but took place earlier in Australia, with the result that its impact became apparent there in 1991 and in Britain in 1992 (table 2). For these years the cosinor analysis for seasonality fell in amplitude and significance, but in 1993 it rose again in both countries, suggesting that the rapid secular trend after the change in clinical practice distorted the seasonal features until the lowered rate became more “stable.”
Data on incidence of sudden infant death syndrome for 1987-93 with results of cosinor analysis
When the later and earlier years are compared the rates fell in every month of the aggregated data. The cosinor amplitude fell, and this was probably due to the falls in each winter month being relatively greater than those in each summer month. These data are shown in table 1 and support that conclusion. There are some differences between Britain and Australia. In table 1, January and July have been matched as being seasonal equivalents, and this shows that the relative fall began two months later in Australia than in Britain and continued for longer.
Discussion
The incidence of the sudden infant death syndrome fell during every month of the year (table 1). Though this fall was absolutely and relatively greater in the colder (and darker) months than in the rest, seasonal variation persisted generally.
COMPARISON OF HEMISPHERES
Given a six month shift in hemispheric phase, the results in the two hemispheres are similar. Though there are apparent differences between them in the pattern of relative fall, these could have arisen by chance. There has been interest in seasonality of the sudden infant death syndrome in many countries,18 and further investigation might clarify these differences. If they are genuine, this could be a latitude effect as Australia lies between the equator and mid-latitude and Britain between mid-latitude and the polar region. Latitude, and therefore length of day, differs considerably between Britain (50-60°C latitude) and Australia (10-40° latitude). Again, despite the broad similarity, the temperature differences between the two countries are considerable, ranging in London from 14°C to 4°C and in Sydney from 23°C to 12°C,19 a contrast which strongly suggests that absolute temperature differences alone do not explain the observed seasonal variation in the syndrome. It is interesting, however, that in studies in both countries Campbell found that the incidence of the sudden infant death syndrome was correlated with a fall in environmental temperature two to five days previously.20 In 1987-90 the extent of the seasonal variation in Britain was slightly greater than that in Australia, but in the single year 1993 it was almost the same (table 2); the results of a single year, however, must be viewed with great caution.
POSSIBLE ROLE OF PHOTONEUROENDOCRINE SYSTEM
It has been argued that recent changes in infant care practice have been partly instrumental in lowering the incidence of the syndrome, as the fall began before the widely publicised advice on a change from the prone to the supine sleeping position.9 There are several possible explanations of the association of the prone position with increased risk of the syndrome, these including thermoregulation,4 5 21 cardiorespiratory reflex interaction,22 and rebreathing of carbon dioxide.23 Another is that there is less exposure of the eyes to light in the prone than the supine position, a fact which is relevant to a unifying hypothesis24 in which the sudden infant death syndrome has been ascribed to a failure of maturation of the photoneuroendocrine system, with resulting impaired production of melatonin. In Britain in 1987-9 the seasonal rise began in autumn, when the days become shorter and darker as well as colder, and in the darkest month (December) not the coldest month (January), while the seasonal change in production of melatonin likewise peaks in December.25
Seasonality of the sudden infant death syndrome has always been an important epidemiological feature, and its importance as a source of possible clues to aetiology remains despite its contraction. Those who have suggested that it may be in the process of disappearing, as a byproduct of the fall in the incidence of the syndrome, were dealing either with small numbers or with a distorting period of rapid secular change in incidence.10 11 12 13 Moreover, each individual year of our data for Britain has had the albeit small advantage of addition of the Scottish figures to those of England and Wales. Only time, however, will tell whether seasonality will contract even further or, instead, will re-expand.
We thank Dr John Rawles, who prepared the cosinor programme. We are grateful to the staff of the medical library and the department of medical illustration of Aberdeen University and to Dr R G Carpenter of the London School of Hygiene and Tropical Medicine for their cooperation. Mrs Muriel Burnett undertook repeated typing of the manuscript.
Footnotes
-
Funding Part of this work was supported by the Scottish Cot Death Trust. ASD was also supported by the Maryland Medical Research Institute.
-
Conflict of interest None.