Article Text

Abstract
Objective To study a novel intervention (REFRESH) aimed at reducing children's exposure to secondhand smoke (SHS) in their homes.
Design A randomised feasibility study.
Setting Aberdeen City and Aberdeenshire.
Participants A total of 59 smoking mothers with at least one child younger than 6 years. Participation took place between July 2010 and March 2011.
Intervention Four home visits over a 1-month period, which involved two 24-h measurements of home air quality (PM2.5) and a motivational interview to encourage changes to smoking behaviour within the home in order to reduce child SHS exposure. The enhanced group received their air quality data as part of their motivational interview at visit 2; the control group received that information at visit 4.
Main outcome measures The main outcome measures were comparisons of the data from visits 2 and 4 on the 24-h average concentration of PM2.5, the peak concentration of PM2.5, the percentage of time when household PM2.5 concentrations exceeded a health-based threshold of 35 μg/m3 and child's salivary cotinine (in nanograms per millilitre). The views of the mothers from the enhanced group about their understanding of the intervention and the measures used were also analysed to assess the acceptability and utility of the intervention.
Results Of the recruited 54 participants, 48 completed the study: 27 from the control group and 21 from the enhanced group. Both groups experienced reductions in PM2.5 concentrations. When testing paired samples for the enhanced group, there was a significant difference (p<0.05) between visit 2 and visit 4 values for maximum PM2.5 (p=0.006) and for percentage of time over 35 μg/m3 (p=0.017), with average PM2.5 approaching significance (p=0.056). There was no significant difference for salivary cotinine. The qualitative findings showed that mothers were able to understand the data they were shown and were shocked by the values measured in their homes despite being aware of the effects of SHS exposure. They appreciated the intervention taking place in their homes as it allowed them to have personalised data. Many mothers described how they had changed their smoking behaviours in their home and in particular were motivated to protect their own children as a result of the knowledge they had gained.
Conclusions Providing mothers who smoke with personalised results about the indoor air quality of their homes along with a motivational interview is feasible and has an effect on improving household air quality. Participants found the intervention understandable and acceptable. Taken overall, the results suggest that a future large-scale trial using measurements of indoor air quality as part of a complex intervention to reduce children's SHS exposure should be explored.
- Environmental tobacco smoke
- intervention
- children
- motivational interviewing
- particulate matter
- mothers
- harm reduction
- secondhand smoke
- primary healthcare
- exposure assessment
- nursing
- qualitative study
- cessation
- health services
- advertising and promotion
- young adults
Statistics from Altmetric.com
- Environmental tobacco smoke
- intervention
- children
- motivational interviewing
- particulate matter
- mothers
- harm reduction
- secondhand smoke
- primary healthcare
- exposure assessment
- nursing
- qualitative study
- cessation
- health services
- advertising and promotion
- young adults
Introduction
Reducing children's exposure to secondhand smoke (SHS) is a significant health priority.1 Exposure to SHS is an important cause of premature mortality and morbidity,2–4 and children are more vulnerable4–7 than adults to the health effects, such as acute respiratory infections, SIDS (sudden infant death syndrome) and slowing of lung growth.8 While evidence suggests that there has been an increase in the percentage of smoking parents adopting a smoke-free home from 16% in 1998 to almost half in 2008 in England and Wales,9 data from Scotland indicate that around 27% of children are still exposed to SHS in their homes10; this is particularly the case for children living in socioeconomically disadvantaged communities.4 ,11 Even though families across all levels of deprivation have shown increased restrictions towards reducing SHS exposure in their homes, homes with greater disadvantage tend to have fewer restrictions.12 Mothers in disadvantaged communities tend to have more restricted lives and are therefore impacted less by tobacco control interventions aimed at the broader population.13 There is a clear and significant challenge to the public health community on how to deliver reductions in both frequency and intensity of children's exposure to SHS in these communities, but a lack of confidence by health professionals is raising this issue.14 ,15
Interventions aimed at reducing children's exposure to SHS have included different theoretical approaches such as those based on behavioural change,16–18 self-efficacy19–21 or educational strategies22 ,23 and have explored a range of methods, including counselling strategies and biochemical feedback.18 ,20 ,24–27 These interventions have shown variable levels of effectiveness, although caution must be applied in interpreting effectiveness due to limitations, such as parental self-reporting of smoking behaviour and lack of objective measures of SHS exposure. The most effective interventions have been those based on longer and more involved contact with parents and carers,28 ,29 but there is a lack of empirical evidence for community and home-based interventions with healthy children.28 ,30 Thus, while there have been increased resources and activity in the UK aimed at reducing children's exposure to SHS in their homes, this is not evidence-based.31
The emphasis of this study was not about cessation but rather about changing smoking behaviours around children. One known effective motivational tool in aiding change in smoking behaviour is the use of instruments to measure carbon monoxide in exhaled breath,32 with some recent qualitative work suggesting that personalised biofeedback of children's exposure to SHS may be a key motivator to household smoking behaviour change33 Additionally, there is evidence from the occupational health literature that suggests that measurement and feedback of information on personal exposure to hazards can help change worker behaviour.34 We reasoned that feedback on air quality within the home setting could work as a powerful tool to change the perceptions and behaviours of smokers. One reliable method for assessing the levels of SHS exposure is by measuring PM2.5,35 airborne particles <2.5 μm in size. Cigarette smoke is the chief source of these particles when environmental levels of PM2.5 are low.36 For PM2.5, the US Environmental Protection Agency (EPA) outdoor air quality standards37 deem that average exposure at levels over 35 μg/m3 over a 24 h period is ‘unhealthy’ for sensitive groups, including children. Using personalised feedback of PM2.5 values in addition to other methods aimed at reducing children's SHS exposure has not previously been studied. The design of the REFRESH intervention, which is a feasibility study of an air quality feedback behavioural intervention, was based on the evidence that people can make changes in response to receiving personalised health-based data along with evidence suggesting some effectiveness in reducing SHS exposure through counselling and extended contact with parents. The intervention design builds on the learning of previous interventions and is based on the hypothesis that parents are likely to change their smoking behaviour if they receive non-judgemental advice from community health practitioners, coupled with information on air quality in their home.
Methods
Recruitment
The study was carried out with 59 smoking mothers across Aberdeen City and Aberdeenshire from July 2010 through March 2011. Ethical approval was obtained from the North of Scotland Research Ethics Committee. Participants were recruited through 23 general practitioner (GP) practices through the Scottish Primary Care Research Network. Our recruitment process initially targeted GP practices in more socially deprived areas in Aberdeen City but extended to other areas within Aberdeen and Aberdeenshire. Records were screened to identify women aged between 18 and 52 years who were smokers. Records were also screened to identify children aged 1–5 years. Mothers and children were then matched by address to produce a list of potential participants, which was screened by the GP practice to remove any mothers it was deemed inappropriate to contact in the professional opinion of the GP. Letters of invitation to REFRESH and study information sheets were sent by the Scottish Primary Care Research Network to all remaining mothers on the list (n=1693). Mothers were asked to return a reply slip stating whether or not they were interested in taking part. This was the first point of contact between the researchers and participants using personally identifiable information. Mothers interested in participating (279 reply slips were received, of which 68 stated they were interested) were telephoned by a member of the research team who carried out a screening questionnaire. Eligibility criteria were mothers who smoked every day, had a child between 1 and 5 years and were fluent in English. If mothers had more than one child in this age group, then only the eldest eligible child was recruited for saliva collection. Mothers were excluded if they had an open coal, wood or peat fire or if they were planning to move from the area in the next 2 months. Once eligibility had been confirmed, the participants were randomised (n=59) to either the control group or the enhanced group. Randomisation was carried out using a web-based programme based on permuted blocks developed by the Centre for Healthcare Randomised Trials at the University of Aberdeen. The next available study ID was entered, which returned either A (control group) or B (enhanced group). Five of the participants who were randomised dropped out before consent was given.
Study design
The study involved four home visits whose format is outlined in figure 1. At visit 1, written informed consent was taken for all participants who were also asked to fill in a questionnaire, which covered demographics, opinions on the effects of SHS, their child's health and smoking restrictions in their home. Participants also completed a daily grid in which they indicated the time, location and number of cigarettes they smoked at home and whether any children were present. A saliva sample collection was attempted for each child using dental rolls cut to two-thirds of their normal size, with a 20 cm length of cotton tied to the middle of the roll. One of these was placed in the child's mouth to one side, leaving the cotton length outside the mouth to allow quick removal of the roll if necessary. The child was asked to chew on the roll until it no longer felt dry or for as long as they could manage. Measurements of the concentration of airborne particulate matter <2.5 μm in size (PM2.5) were made using a SidePak Personal Aerosol Monitor AM510 (TSI Inc, MN, USA). Measurements were logged every minute over a 24 h period in the room where the family said that they spent the most time, typically the living room. The Sidepak was placed at a level of between 1 and 1.5 m on a table or shelf with close access to a mains electricity plug while being positioned at least 1 m away from doors, windows or heat sources where possible.

Outline of study design. PM2.5, particulate matter <2.5 μm in diameter; SHS, secondhand smoke.
Twenty-four hours after visit 1, the researcher returned to collect the Sidepak device and deliver the motivational interview to participants. In motivational interviewing, clients' decisions about behaviour change are guided and supported.38 These principles were used to structure our motivational interview. The interview was designed as a dialogue between the researcher and the participant, with an emphasis on the participant generating their own responses in terms of identifying the pros and cons of any current and future smoking restrictions in the home, as well as how to overcome any difficulties they might face in changing their behaviour. The motivational interviews were audio recorded for both arms of the intervention. Both field researchers (IW and LMM) were trained in motivational interviewing techniques and were given a formatted script to follow when delivering the intervention to maintain consistency (figure 2). One researcher delivered all the control interventions (LMM), while the other (IW) delivered all the enhanced interventions to prevent the introduction of bias. A random 20% of the audio files were quality checked by a team member (DR) with skills in motivational interviewing to ensure consistency in delivery of the intervention. Enhanced participants were also given information about the PM2.5 levels measured in their homes over the previous 24 h, as well as guidance about how to interpret these readings in relation to health-based air quality standards. They were shown the graph of their minute-by-minute readings on a laptop and were also given a paper bar chart illustrating how their household average and peak concentrations compared with the health-based guidance for PM2.5. A hard copy of the minute-by-minute graph of their readings (example in figure 3) including a line indicating the health-based guidance was posted to enhanced participants immediately following visit 2. Control participants were not shown the graph on the laptop or the bar chart and did not receive the hard copy graph in the post until the completion of visit 4.
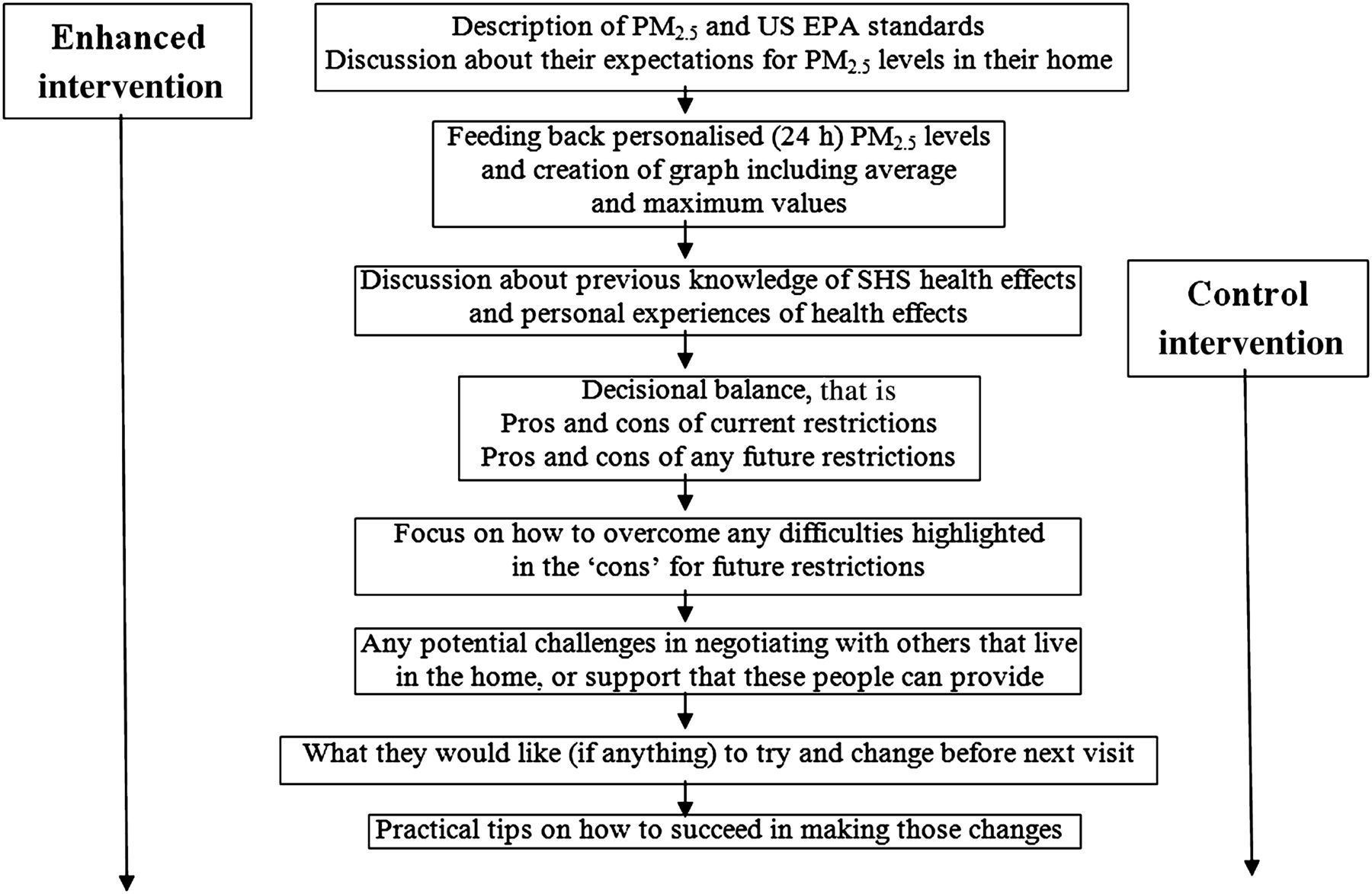
Flow chart detailing components of the motivational interview. PM2.5, particulate matter <2.5 μm in diameter; US EPA, United States Environmental Protection Agency; SHS, secondhand smoke.

Graph of 24 h PM2.5 readings indicating United States Environmental Protection Agency 24 h air quality guideline. Average PM2.5 for this participant = 85 μg/m3, maximum PM2.5 = 455 μg/m3. PM2.5, particulate matter <2.5 μm in diameter.
Follow-up visits were carried out on average 4.7 weeks (4.0–10.3 weeks) after visit 1. The first follow-up (visit 3) involved setting up the Sidepak device in the same location as at visit 1, as well as an attempt at child saliva collection if collection had been successful at initial visits. Participants also completed a short questionnaire asking about any changes they had made since visit 2 to their smoking, particularly around children. The following day (visit 4), all participants were shown their PM2.5 data. Enhanced participants were reminded of their initial readings and shown their final readings. Control participants were given information about PM2.5 and shown their readings from both time points.
Qualitative assessment of the enhanced intervention
At visit 4, semistructured interviews were undertaken with the 17 enhanced participants who had at least 1 min where household PM2.5 exceeded the US EPA unhealthy level at baseline. The interviews lasted 10–30 min. An interview topic guide was used to conduct each interview. Participants were asked questions exploring any changes they had experienced throughout the duration of the study. They were also asked about their understanding of the study and any perceived enablers and barriers to changes made as well as perceived benefits to themselves and others through having taken part. Participants were also asked to give any suggestions for improvement and if they thought an intervention of this type would be appropriate to develop as a community intervention tool.
Analysis
Statistical analysis
The PM2.5 and salivary cotinine data were log-transformed to normalise the distributions, and geometric means and geometric SDs were calculated for all measures. Where necessary, PM2.5 data were adjusted to take account of incomplete sampling times from one measurement time point. In the few instances where one of the two paired PM2.5 measurement periods was substantially less than 24 h, results from the longer period were edited to correspond with the shorter time period of the other measurement, eg, 9 am to 11 pm. An independent t test was used to compare results between interventions, and paired t tests were used for within intervention baseline to final comparisons. Independent t tests and χ2 tests were used to compare demographics of the two intervention groups. A measure of household deprivation was assigned based on the participant's postcode. The Scottish Index of Multiple Deprivation (SIMD) uses 31 indicators of health, wealth and access to resources that provides an indicator of area deprivation. We employed quintiles with SIMD 1 being the most deprived and 5 the least deprived. Standard statistical software was used (PASW V.18.0), and significance was assumed when p value was <0.05. Saliva samples were analysed by ABS labs (Cambridge, UK) for cotinine concentrations. The limit of detection for this analysis was 0.1 ng/ml.
Qualitative analysis
The audio recorded motivational interviews (visit 2) and semistructured interviews (visit 4) were transcribed for the enhanced participants and then analysed thematically, moving from initial descriptive codes to more conceptual analytic coding. Three authors (IW, DR and AA) were involved in the analysis, with at least two reading each transcript and agreeing on themes. A modified grounded theory approach was taken whereby themes were revised iteratively as the fieldwork and analysis progressed.39 The analytical procedure was supported by the use of NVivo V.9.0 to aid data retrieval and close analysis. Comparisons were made across interviews and within themes to explore analytical categories rigorously. Illustrative quotes provided in the Results section detail the age and SIMD of the participant and the visit from which the quote is taken.
Results
Study subjects
Recruitment rate was 3.5% (59 from 1693). Five subjects withdrew from the study prior to completing the first visit and so baseline (visits 1 and 2) data were collected for 54 participants. Six subjects were lost to follow-up and so final (visits 3 and 4) data were available for 48 participants. PM2.5 data were successfully collected in 53 of the 54 baseline visits and 47 of the 48 final visits (machine failure in each of these cases). A summary of the numbers of data available at each stage of the study is provided in figure 4. The average age for mothers at baseline was 30.0 years (range 19.7–45.7 years), with average child age of 3.5 years (range 1.2–5.7 years). There were no significant differences between participants in the two intervention groups at baseline. The six mothers who dropped out after visit 2 were younger than those who did not (24.6 vs 31.3 years, p=0.020), and five of these (83%) agreed with the statement ‘the dangers of inhaling other people's tobacco smoke are greatly exaggerated’ compared with 19% of participants who completed the study (p=0.013). Table 1 shows details of participants at baseline as characterised by home type and level of socioeconomic deprivation as measured by SIMD, which is based on postcode of residence reflecting material deprivation.40 Two participants returned unknown SIMD scores as they were living in newly built homes.

Flow chart indicating the numbers of subjects at each stage of the study/data collection. PM2.5, particulate matter <2.5 μm in diameter.
Distribution (n) of accommodation and SIMD of participants by intervention
Measurements of PM2.5 and salivary cotinine
PM2.5 data were successfully collected in 53 of the 54 homes at baseline and 47 of the 48 at the final measurement time. At baseline, the average sampling time was 23:06 h (13:03 h to 24:27 h); at final it was 22:33 h (10:42 h to 26:33 h). The geometric mean values for the measurements of average PM2.5, maximum PM2.5, percentage of sampling time over 35 μg/m3 and salivary cotinine on all measurements taken at baseline and final are presented in table 2. Greater detail on the distribution of the baseline PM and salivary cotinine data is presented elsewhere.41 There were no statistically significant differences at baseline between control and enhanced data. Across all measures, both control and enhanced participants made reductions. There was a greater reduction achieved from the enhanced intervention and a significant difference (p<0.05) for the enhanced group between baseline and final values for the maximum PM2.5 (p=0.006) and for the percentage of time over 35 μg/m3 (p=0.017); the fall in average PM2.5 approached significance (p=0.056). The reduction in salivary cotinine was not significant.
Geometric means (GM) and geometric SD (GSD) on adjusted PM2.5 data and salivary cotinine for control and enhanced interventions
Paired PM2.5 data (ie, where data were available for a home at both baseline and follow-up) were available from 26 of the control and from 20 of the enhanced homes. Figure 5 provides paired PM2.5 data for each participant for 24 h average (A), maximum (B) and percentage of time above the 35 μg/m3 threshold (C) at both baseline and final measurement subdivided by intervention type. These data are presented on a log-log scale with points above the ‘no change’ line indicating an increase in exposure postintervention, while points below this line demonstrate a decrease in exposure. For all three measures, more points show decreases in exposure compared with increases with enhanced intervention participants particularly likely to demonstrate improvement in PM2.5 measures.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Log scale scatter plots of baseline and final data for average PM2.5 (A), maximum PM2.5 (B) and percentage of time over 35 μg/m3 (C). PM2.5, particulate matter <2.5 μm in diameter.
Paired data for 33 samples of children's salivary cotinine data were also available. The geometric means for percentage change for the three measures of PM2.5 and salivary cotinine on the paired data are presented in table 3. For all measures, there was a greater per cent change for the enhanced intervention than for the control intervention, although these were not statistically significant. When comparing change between the control and enhanced groups on all measures, none of these values were statistically significant (table 3).
Geometric means for percentage change in paired measures of PM2.5 and salivary cotinine
Qualitative findings
Feasibility, acceptability and understanding of the intervention
By reviewing the transcripts of the motivational interviews (visit 2) of the enhanced intervention participants who completed the entire study (21) and their visit 4 semistructured interviews (17), we were able to develop a picture of smoking mothers' experiences of the intervention. Findings from the transcripts indicated that mothers found the intervention as a whole acceptable and were also able to understand the data they were shown. The acceptability of the intervention was highlighted by their willingness to engage with all aspects of the intervention and eagerness to share their experiences with others, including family, friends and colleagues (box 1). Participants described their experience as providing them with information which they could then use to make informed decisions about reducing their children's exposure to SHS (box 1).
Acceptability and understanding of the intervention
Acceptability of the intervention
I showed them. I showed them the chart, you know, the graph. I showed them how high it was, and some of them was like—you're joking? And I was like no, that's why I'm in the kitchen. I says—so if that's what's going about in the air, can you imagine what's inside the kids. And they were quite happy enough to go in the kitchen. (32, SIMD 1, visit 4)
Basically it isn't a lecture. You're not trying to put me off smoking if you like; you're just giving me the evidence to make up my own mind. (35, SIMD 5, visit 4)
So my idea is that you've came here to highlight what we didnae (didn't) really know and then it's up to us, like you've said from day one, you're not here to preach or tell us what to do. You're here to give us results and then say, here you go, it's up to us to decide what we're going to do about it. (45, SIMD 4, visit 4)
Knowledge gained around SHS exposure
It's given me more knowledge and understanding about secondhand smoke and about how much it actually travels and how long it lasted for as well. So it has increased my knowledge and I can use that for what's best for (my child) as well. (25, SIMD 2, visit 4)
Because what we've found out there, like I say, we wouldn't have known. Like I say I wouldn't have known even those levels. You just assume that because you smoke outside, everything's fine. (34, SIMD 5, visit 4)
I just wouldn't have thought it would be that. Because I don't sit here and smoke, I didn't think it would be that at all. (23, SIMD 1, visit 2)
For me you were showing how to give my family a healthier life and how high the levels actually are. Cause I'm guessing that a lot of people don't know. Unless it's sitting there in front of you on a graph, you don't. (23, SIMD 1, visit 4)
While most participants did have some previous knowledge about the health effects related to SHS exposure, they valued the additional information that was provided during the intervention visits, particularly information about how long SHS can remain in the air and how far it can travel through the home after extinguishing a cigarette (box 1).
Motivators and mechanisms of change
The mothers tended to express their reaction to measured PM2.5 levels as shock (box 2). Participants felt that they had been smoking in their home in a way that was protecting their children from SHS exposure and were very surprised at the levels recorded in their homes. It was very important for these mothers that the data they were shown were personal (box 2). They knew where we placed the instrument and also where and when they smoked, so they could relate the results directly to what they experienced on a daily basis in their own homes.
Motivators and mechanisms of change
Reactions to PM2.5 data
Seeing the results made a big difference. It was like a shock because I didn't realise. Like I don't sit here and smoke in front of (my child), I do it in the kitchen, but for the readings to be high like that when I'm not like anywhere near it, if you know what I mean, it's like a shock factor to realise what it can do. So I think that's the best thing that like helped me. (23, SIMD 1, visit 4)
It was just a shock to how much you can get off a cigarette with just lighting it and thinking, how many times have I smoked in the kitchen and how much it just stays there for ages after. And I thought, oh my god you know, I'm making them breathe that in. (41, SIMD 3, visit 4)
Tonight when he comes in I'll just discuss it with him and I'll show him the graph which I'm sure he'll be quite shocked at himself. He just wants the best for our son too. (37, SIMD 2, visit 2)
(I will) Pin this up to the wall and keep this handy and I'm sure if I showed anyone that coming into this house they would have a shock as well. (23, SIMD 1, visit 2)
Importance of personalised data
You know the layout of the house, you know obviously the distance from the back door to my living room and so on but sitting in a community centre talking about it you just wouldn't feel like it was, you know, it wouldn't have any impact. (28, SIMD 5, visit 4)
I think it's good to see it because it shows you, like it actually shows you the proof sort of thing, if you know what I mean. That was the thing that really changed my mind. (23, SIMD 1, visit 4)
It does make you aware even though you are already. But having it in front of you makes it real. (35, SIMD 5, visit 4)
To be done in your own house is more recognisable than to be told in a community centre or a church or even a doctor's surgery. For it to be done in your own home and for you to know that the level of smoke is so high and you're putting your children at risk of asthma, emphysema, all kinds of things, it's quite shocking. (37, SIMD 2, visit 4)
Many mothers expressed the view that personalised data made the concept of the dangers of SHS more real to them than if they had simply heard or read about it (box 2). The most important result was that after having experienced the intervention, gained the knowledge about SHS exposure and felt the shock and surprise in relation to their personal PM2.5 levels, the mothers appeared very motivated to change their smoking behaviours in their homes. This was expressed during discussion in the motivational interviews. Their motivation was often contextualised in relation to protecting the health of their children, with their own health as secondary (box 3).
Children's health as motivator to change
But at the end of the day I would just have to stick to it because it's (my child's) health that it's coming down to. I've made my decision for myself to smoke but it's not fair that I'm putting my smoke on him, my health problems on him. I just have to keep thinking, it's not for me, it's for (my child). (23, SIMD 1, visit 2)
My kids, I just used to think about my kids. Say well, I'm nae deein (not doing) this for me, I'm deein (doing) it for the sake of them. (32, SIMD 1, visit 4)
Just remember that it's for the best for (my child) and just remember that it's important for him that we're doing it, because it's not fair that our kind of habit, that we're kind of exposing him to this. And we thought that we were doing everything right and unfortunately we're still kind of putting him at risk. So kind of reminding ourselves of that. (25, SIMD 2, visit 2)
For me I think, my son's health, that's my priority. So I would like to think that all mothers would think like that, that their kids come first no matter what. My bad habits shouldn't be put onto (my child). Because I can't stop smoking doesn't mean he has to suffer. (23, SIMD 1, visit 4)
Participant views on the intervention
Overall, the mothers who took part were very positive about the whole experience, even those that did not make any changes. When asked at visit 4 if the intervention should be developed into a community health initiative, most mothers suggested that it was a good idea and something that could make a difference (box 4). Mothers were also asked specifically whether they thought health visitors would be well placed to deliver the intervention. While most were positive about health visitors' involvement, some mothers expressed the view that this could be problematic if the intervention was delivered as a lecture rather than a discussion.
Participant views on the intervention
So I think it does help, you only see little things on tv like how bad this stuff is, but to have somebody there to say well what changes can you make, or how about if you do it this way, so it does help. (23, SIMD 1, visit 4)
I think when other people see that it will give them the incentive, if not to stop then to smoke out the window or go outside. I think health visitors should be given the opportunity to offer people this kind of information. (37, SIMD 2, visit 4)
It's helped me out and I think it would be useful for a lot of other people as well. Especially people with newborns and stuff. Like you said, I think if health visitors used it, it would shock a lot of mums to be or new mums and they wouldn't be in the position I'm in because they would've stopped a long time ago with information like that. (23, SIMD 1, visit 4)
Discussion
National campaigns and the introduction of smoke-free legislation in public places across the UK have raised public awareness about the harmful effects of SHS exposure.1 The private domain is now the main location of exposure to SHS for children,42 but reducing exposure in this domain is more difficult to influence. Previous work in the USA has shown that feedback of information on airborne nicotine levels may be useful in changing smoking behaviour of parents who smoke,27 while a recent study has looked at the use of air-filtration systems to reduce children's exposure at home.43 Our study developed a novel intervention using real-time minute-by-minute data on air quality aimed at reducing children's exposure to SHS in their home and explored its feasibility, utility and acceptability. The results indicate that showing smoking mothers the real-time air quality data from their homes in addition to a motivational interview including standard advice on how to reduce children's exposure to SHS in the home may be a useful tool in helping some mothers change household smoking behaviours.
Strengths and limitations of the study
There are a number of potential weaknesses in our study. The sample was small, limiting the delivery of statistically robust results and not all measures of exposure were collected from all participants with salivary cotinine particularly difficult to measure in younger children. However, our data show a promising trend whereby enhanced participants appeared to make greater changes than those who received the control intervention, and we were able to demonstrate improvements in air quality, which were associated with a trend for reduced salivary cotinine concentrations for children. Additionally, the qualitative findings provide insight into the feasibility, utility and acceptability of delivering the intervention to mothers in their own home, though we acknowledge that by not interviewing the control mothers at the end of the trial we may have introduced some bias in our qualitative results. The clinical implications on child health when improving indoor air quality remain to be determined.
We acknowledge that there is the possibility that families modified their smoking behaviour for only a short time around the follow-up visit and that this may have been differential between the control and enhanced intervention groups. However, we note that the children's salivary cotinine values, likely to reflect exposure over a longer time than the 24 h air sampling, did show greater reductions in the enhanced group compared with the control group, although this difference was not statistically significant due to the size of our study. The qualitative data also tends to support that mothers complied with the study protocol and did not engage in tactics to influence the air quality measurements. It is likely that we recruited a more motivated group than if we had a representative sample of smoking mothers, but the changes made were not produced equally across both arms of the intervention reflecting evidence of an intervention type effect despite probable differences in initial levels of motivation. The magnitude of effect may be different in different demographic groups, but we were unable to explore this possibility due to low numbers of subjects in this pilot study. The 1-month follow-up does not enable us to say anything about the sustainability of the changes made, but in the qualitative interviews, some mothers expressed the view that their success in reducing exposure levels had led them to consider future changes they might make, including quitting smoking.
Smoking mothers is a population of individuals that is difficult to reach.44 Although only a small group of women, 3% of those invited, agreed to take part if the intervention was delivered by midwives or health visitors, there may be a greater chance of recruitment, as in the work by Tappin et al (2000)45 where 75% of pregnant smokers approached took part in a home-based motivational interviewing intervention delivered by midwives. While the current literature presents a lack of evidence base for effective home-based interventions with healthy children in the UK,29 we were able to demonstrate an effect on indoor air quality. Although our sample size was small compared with other interventions, it was a feasibility study. Despite this, we were able to demonstrate a large effect on PM2.5 and any apparent lack of effect on salivary cotinine was likely due to sample size and potential exposure by the children to alternative sources of SHS exposure. Furthermore, all measurement of SHS exposure was objective, both at baseline and at final, instead of through self-reported change.
Particular strengths of this work were that we were able to take measurements of salivary cotinine in children younger than 6 years, and to obtain both air quality and saliva measurements at two time points over a 1-month period, giving longitudinal representation of the levels of SHS exposure in homes of smoking mothers with young children. However, we only measured the air quality using static sampling devices in one room of the house and did not measure the children's movements during sampling time, so we cannot know for sure to what extent their personal exposure to SHS was from their home or from other environments, such as a grandparent's home.
The intervention used PM2.5 rather than nicotine as a marker for SHS. We acknowledge that PM2.5 is not as specific to SHS as nicotine and that other sources (outdoor air pollution from diesel engines, candle burning, etc) exist. However, we feel that the advantages of being able to measure log PM2.5 concentrations every minute (something not possible for nicotine) and being able to refer measured levels to health-based guidance on air quality were particular strengths in our approach compared with other studies.27 At the inception of our study, we decided to use the US EPA guidelines on PM2.5 air pollution relating to 35 μg/m3. However, during the time of the study, the WHO published guidelines46 suggesting that outdoor air concentrations of PM2.5 should not exceed 25 μg/m3 averaged over a 24 h period and that these standards can also be applied to indoor settings. This gives us confidence in the advice relating to PM2.5 exposure we shared with mothers, despite a lack of knowledge about the implications of improving indoor air quality on children's health. Another strength was that despite receiving potentially difficult information, the mothers with whom we spoke were positive about their experiences, and we were able to thoroughly explore these experiences with the enhanced group. We did not explore the experiences of the control group; however, the enhanced group received the intervention as it would be delivered by health professionals so we needed to understand their perspective as representative of how the intervention would be received by the community.
Conclusions
This study has shown that lay people can engage with science and can understand quite complex exposure data when it is presented in a number of clear formats. Mothers were able to understand their personal exposure data within the context of health-based exposure guidelines, and this was used to share with others about potential dangers of SHS exposure. A health-based benchmark or guidance value for the SHS marker being measured is an important facet of any communication strategy. Additionally, it was shown that personalised data, even if shocking, can be empowering when followed by immediate support for change. In our study, average 24 h PM2.5 exposure across all homes was 22 μg/m3. Our observation that in almost all participating households, indoor air PM2.5 approached a threshold considered unhealthy, suggesting a need to reduce indoor air PM2.5 in many households across the UK, and that many people would benefit from such an intervention. It is not clear who would be best placed to deliver an intervention of this type in the community. A future large-scale trial with longer follow-up, ideally over 12 months, would be needed to further assess the most effective delivery of the intervention and to determine if the promising impact found in this study can be replicated with a larger representative sample of smoking mothers.
What is already known on this subject
-
Exposure to SHS is an important cause of morbidity in children, who are most often exposed to SHS in their homes, particularly in disadvantaged areas.
-
Many homes do have some form of restriction regarding smoking behaviour.
-
Extended contact with parents and the use of motivational interviewing have been promising in reducing children's exposure to SHS, but evidence of effective interventions in the home is limited.
-
Showing workers information about the hazards they are exposed to influences behaviour changes to reduce that exposure.
What this study adds
-
Combining motivational interviewing with personalised feedback about objective SHS measurement in the home appears promising in reducing children's SHS exposure.
-
Knowledge about PM2.5 and SHS exposure among smoking mothers of young children is limited.
-
Increasing mothers' awareness of the risks related to these can cause shock, but providing personalised data with immediate support to find solutions to their envisaged barriers is empowering in supporting them in reducing SHS in their homes.
Acknowledgments
We are grateful to all the GPs and study participants who took part in this study and to Amanda Cardy who conducted all searches for participant recruitment through the Scottish Primary Care Research Network. Laura MacCalman at the Institute of Occupational Medicine provided advice on the statistical analysis.
References
Footnotes
-
Funding This work was supported by the Big Lottery Fund, grant number RGT/1/010332728.
-
Competing interests None.
-
Ethical approval The study complied with the code of practice on ethical standards for non-commercial research with the North of Scotland Research Ethics Committees and NHS Grampian Research and Development Office.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement We are currently analysing and seeking to publish both qualitative and quantitative data from other parts of this study and so are not in a position to share the remaining data collected from the REFRESH study. Anonymised quantitative data directly linked to that presented in this study will be made available on request.