Article Text

Abstract
Outcome of full-term infants with neonatal encephalopathy of hypoxic-ischemic origin is often assessed in infancy or early childhood and data on outcome in childhood and adolescence is limited. MRI performed in the neonatal period has made a huge contribution to recognition of different patterns of injury. These different patterns of injury are related to the severity of later motor and cognitive disabilities.
Long-term follow-up shows that cognitive and memory difficulties may follow even in children without motor deficits. It is therefore recommended to perform follow-up assessment into childhood in children with and without adverse neurological outcome in early infancy.
Statistics from Altmetric.com
Neonatal encephalopathy (NE) occurs in 1–6/1000 live full-term births and carries a high risk for subsequent neurodevelopmental disabilities.1 Long-term outcome is known to depend on the severity of the neonatal condition.2 3 The term NE is now more often used than perinatal asphyxia (PA). This is because PA is difficult to define and in order to be reliable, needs access to several markers which are not always available, such as fetal heart rate tracings, umbilical cord gases and reliable Apgar scores. Individually, these markers have been shown to not correlate very well with subsequent outcome.4 5 NE is ‘a clinically defined syndrome of disturbed neurological function in the earliest days of life in the full-term infant, manifested by difficulty with initiating and maintaining respiration, depression of tone and reflexes, subnormal level of consciousness and often seizures’. The widely used three-level grading system of mild, moderate and severe encephalopathy, based on clinical symptoms and EEG, was developed by Sarnat and Sarnat.6 They based their encephalopathy score on an assessment in only 21 infants. The development of encephalopathy in full-term infants within hours to days after birth is now considered essential in order to be confident about an underlying perinatal insult, and NE is almost invariably associated with several of the markers mentioned above.7 NE can develop for reasons other than hypoxic-ischaemia, for example, metabolic disorders, therefore a combination of markers suggestive of the presence of PA as well as the development of NE is obligatory.
Most studies reported so far have focused on early neurodevelopmental outcome at 18–24 months, looking mainly at development of cerebral palsy (CP) or severe cognitive deficits.8 Outcome of infants with mild NE have been reported to be comparable to non-affected full-term infants,2 9 while those with severe NE will either die or invariably develop CP and cognitive deficits. Pin et al3 reviewed 13 empirical studies, meeting strict inclusion criteria and found adverse outcomes under 3 years in none of the infants with mild NE, 32% in those with moderate NE and almost 100% of those with severe NE. Very similar data were found in an earlier review by Dilenge, et al.10 The infants with moderate NE tend to have a more variable outcome and other techniques, such as neuroimaging techniques, in particular MRI and neurophysiological tests, especially amplitude integrated EEG (aEEG) and evoked responses are required to more accurately predict neurodevelopmental outcome.11 12
Only a few studies provide detailed assessment of longer term outcome.13,–,16 The American College of Obstetricians and Gynecologists task force on NE and CP made a statement that an acute intrapartum event (most often associated with a sentinel event) could only result in CP of the tetraplegic or dyskinetic type and could not result in isolated cognitive deficits.17 A recent review by Gonzalez and Miller18 provided sufficient data to illustrate that survivors of NE following PA are also at increased risk of cognitive deficits, even in the absence of motor deficits. Outcome studies performed so far, found cognitive functioning at school age to be normal in children with mild NE.13 14 The first study looking at long-term outcome at 5.5 and 8 years following NE, was performed by Robertson et al14 They found that non-disabled survivors of moderate NE were similar to controls with respect to receptive vocabulary and perceptual motor skills, but showed marked delays in reading, spelling and arithmetic. These children were more likely to be at least one grade behind controls or those with mild NE. A recent study by Marlow et al16 assessed 65 children with NE at 7 years of age. They classified infants as having moderate NE when they presented in the first week after birth with either seizures alone or any two of the following: abnormal consciousness; difficulty maintaining respiration (of presumed central origin); difficulty feeding (of presumed central origin); abnormal tone and reflexes, with all lasting for more than 24 h. The children with severe NE had to fulfil one or more of the following criteria: ventilation for more than 24 h; two or more anticonvulsant treatments required; comatose or stuporous. One should be aware of these definitions of moderate and severe NE, as the presence of requiring ventilation and two or more anticonvulsant drugs would be considered to be moderate NE by most clinicians. Some of their severe NE cases could therefore represent more severely affected moderate NE children. No neonatal neuroimaging or neurophysiological data, such as aEEG was available for these children. They reported that those with moderate NE were not different from controls with respect to general cognitive ability, but lower in language and sensorimotor domains, as well as narrative memory and sentence repetition. The children were more likely to require extra educational assessment, teaching provision and support, even though they did not have any overt neuromotor impairment. Among the more severely affected children, referred to as severe encephalopathy, memory for names, orientation and reported everyday memory function were also significantly poorer than for either comparison children or the moderate encephalopathy group.
Specific memory impairment has been the topic of recent studies, initially noting a specific and severe impairment of episodic memory (context-rich memory for events) with relative preservation of semantic memory (context-free memory for facts).19 Since then, others have found problems in verbal learning and/or recall14 20 21 and in visual recall20 in school-aged children and adolescents with moderate NE. These findings stress the importance of detailed examination of the developmental impact of NE on memory function. The known associations between the hippocampal structures and memory function22,–,25 suggest that children with NE could be at risk of developing problems in this specific domain of cognitive functioning.
Patterns of brain abnormalities on MRI predict outcome in early childhood
The increased use of neuroimaging techniques and MRI in particular, has been a tremendous help in timing of brain injury and recognising the pattern of injury.11 26 Performing MRI within the first 2 weeks after birth, Cowan et al26 were able to show that more than 90% of affected newborns had evidence of perinatally acquired lesions on their MRI, with a very low rate of established antenatal brain injury. The use of diffusion-weighted imaging (DWI) has also greatly improved our ability to time the onset of brain lesions. A reduced apparent diffusion coefficient can be calculated, showing reduced values (restricted diffusion) during the first few days after the insult, with pseudonormalisation by the end of the first week.27
Comparable to studies in a primate model,28 two main patterns of injury can be distinguished with MRI in the full-term neonate:
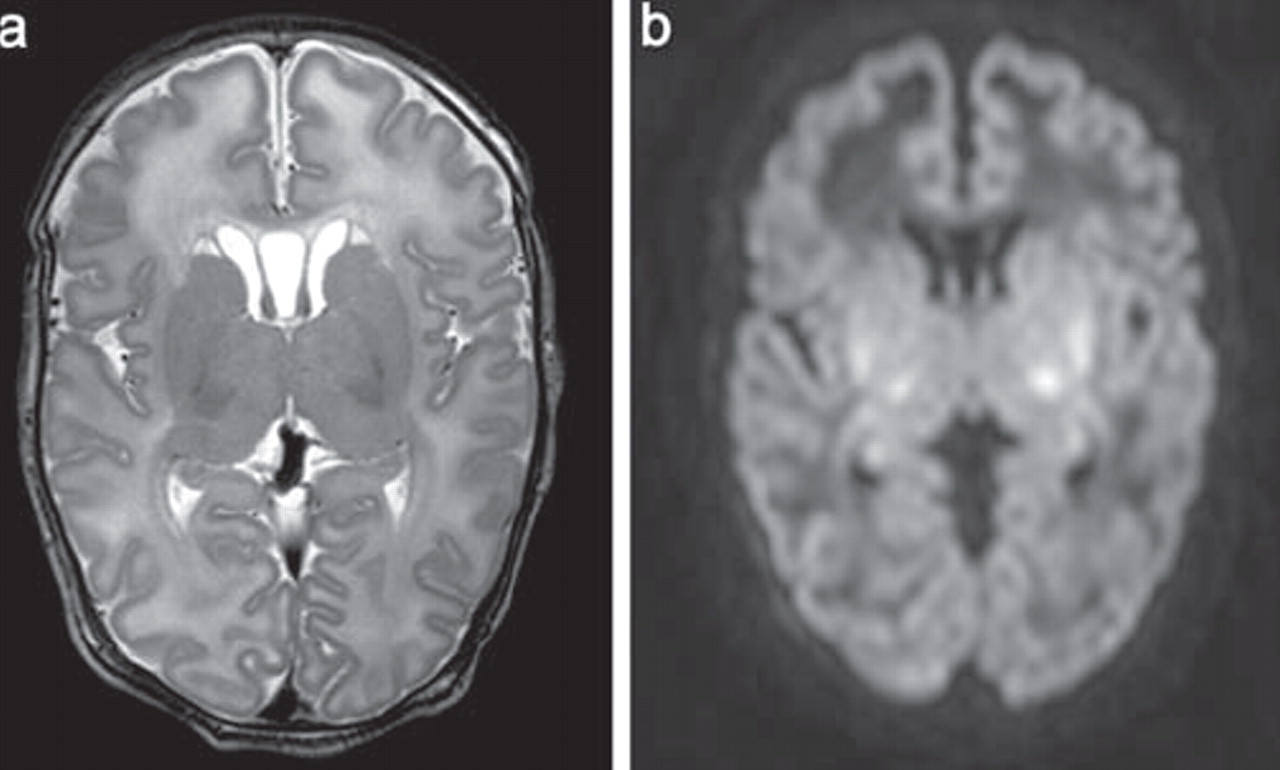
A basal-ganglia-thalamus pattern (BGT) predominantly affecting bilaterally the central grey nuclei and perirolandic cortex. Associated involvement of the hippocampus and brain stem is not uncommon (figure 1). This pattern of injury is most often seen following an acute sentinel event29 and is also referred as a pattern following ‘acute near total asphyxia’.30 Using conventional MRI, it was shown by Rutherford et al31 that absence of a normal-high signal intensity of the posterior limb of the internal capsule is highly predictive of severe adverse sequelae. More accurate information about timing of injury can sometimes be obtained when measuring the apparent diffusion coefficients, but due to evolution over time, this was mainly helpful in the most severely affected infants, who had an MRI performed within the first few days after birth.32 The children with the BGT pattern of injury are often so severely disabled that they will not be included in long-term follow-up studies. Ability to sit by 2 years of age and walk by 5 years of age occurred in five of the seven children who showed involvement restricted to the nucleus lentiformis and ventro-lateral thalamus, while none of the 10 children with more extensive injury, including injury to the perirolandic cortex and hippocampus were able to reach these goals.33 Himmelmann et al34 studied 48 children at a mean age of 9 years (range 4–13 years) with dyskinetic CP mostly due to BGT injury and found that most children had Gross Motor Function Classification System levels of level IV, n=10 and level V, n=28. The rate of learning disability (n=35) and epilepsy (n=30) increased with the severity of the motor disability.
The watershed predominant pattern of injury (WS) is the other pattern of injury which is also referred to as a pattern seen following ‘prolonged partial asphyxia’. The vascular WS zones (anterior-middle cerebral artery and posterior-middle cerebral artery) are involved, affecting white matter and in more severely affected infants also the overlying cortex (figure 2). The lesions can be unilateral or bilateral, posterior and/or anterior. Although loss of the cortical ribbon, and therefore the grey-white matter differentiation can be seen on conventional MRI, DWI highlights the abnormalities and is especially helpful in making an early diagnosis.35 A repeat MRI may show cystic evolution, but more often atrophy and gliotic changes will be recognised.36 It is also more common after hypotension, infection and hypoglycaemia, all of which may be associated with a more protracted course.37 As (severe) motor impairment is uncommon in this group of infants, they are not uncommonly considered to have an early normal outcome, when seen at 12–18 months and are then discharged from further follow-up. However, suboptimal head growth, behavioural problems and delay in language are common.38 39 Several studies have now, however, shown that these children ‘grow into their deficits’ and it is this group in particular that needs follow-up well into early childhood. Miller et al40 were first able to recognise cognitive deficits associated with the WS pattern of injury at 30 months, while the problems were largely overlooked, when seen at 12 months. More recently they also showed a correlation with verbal IQ at 4 years of age.39

MRI on day 5. (A) T2 weighted spin echo sequence showing a large cavum septum pellucidum and supendymal pseudocysts as incidental findings. The white matter has a high signal intensity, especially anteriorly and the basal ganglia are swollen and the thalami are of lower signal intensity. (B) Diffusion weighted imaging shows low SI in the anterior white matter and areas of restricted diffusion in the ventrolateral thalami and lentiform nuclei bilaterally. Restricted diffusion is also seen at the level of the hippocampi.

MRI on day 3 (A,B) and at 22 months (C) in an infant with WS injury. (A) T2 weighted spin echo sequence image showing loss of the cortical ribbon mainly in the left frontal and right parieto-occipital region. (B) Apparent diffusion coefficient map also showing involvement of the right anterior watershed region as well as the right optic radiation. (C) Inversion recovery sequence showing sequelae in the right occipital region. Outcome at 3 years is within the normal range (DQ 90).
In addition to the above described two main patterns of brain injury, lesions restricted to the periventricular white matter, not dissimilar from the so-called punctate white matter lesions in the preterm infant can also be distinguished as a separate pattern of injury, although less common (figure 3). Li et al41 pointed out that infants with this type of injury are significantly less mature and they were noted to have milder encephalopathy and fewer clinical seizures relative to other newborns in the cohort with the two more common patterns of injury. Finally perinatal arterial ischemic stroke and perinatal haemorrhagic stroke can occur but these lesions are usually not related to PA42 43 and are therefore outside the scope of this review.

{kind=link}
{kind=link}
{kind=link}
MRI on day 7 in an infant with punctate white matter lesions. (A) T2 weighted spin echo sequence image showing multiple Punctate white matter lesions (PWML) predominantly on the right side. (B) Apparent diffusion coefficient map showing the PWML as areas of restricted diffusion. Outcome at 3 years was within the normal range (DQ 96).
Although not widely used at present, magnetic resonance spectroscopy is especially helpful when an MRI is performed on day 1, when changes on conventional MRI are often restricted to cerebral edema, and at a time when changes in the posterior limb of the internal capsule are not yet visible and DWI changes may still become more extensive.44 There is no agreement about the best ratios to predict outcome. Roelants-Van Rijn et al45 concluded that low N-acetylaspartate/choline and high lactate/N-acetylaspartate ratios best predicted a poor outcome in neonates with cerebral hypoxia-ischemia with echo times of 272 and 136 ms having a better predictive value than echo times of 31 ms. A recent meta-analysis including 32 studies and 860 babies, found the diagnostic odds ratio to be highest for lactate/N-acetylaspartate (82.1 (21.3, 316.9)), followed by Lac/creatine (25.4 (7.1, 91.8)) and N-acetylaspartate /creatine (4.31 (1.4, 13.8)).46 Magnetic resonance spectroscopy can be a useful early magnetic resonance biomarker and is put forward as a surrogate end point in clinical trials.46
Few studies have correlated neonatal MRI and outcome in early childhood. Belet et al47 described that normal neonatal MRI findings were associated with a normal neurological outcome (negative predictive value: 100%) and abnormal MRI findings had the highest predictive value in predicting an abnormal outcome at the age of 4 months and 4 years (positive predictive value: 100%). Barnett et al15 studied 68 full-term infants with NE at 5–6 years of age. Of the 53 surviving infants, 19 developed CP while the remaining 34 were considered normal at 2 years of age. When seen at school-age, eight children showed minor neurological dysfunction and/or perceptual motor difficulties, one had only cognitive impairment and 25 were considered normal. While 83% of those with a normal outcome had a normal neonatal MRI or an MRI with discrete white matter lesions, 80% of those with minor neurological dysfunction and/or perceptual-motor difficulties had mild or moderate basal ganglia lesions or more marked white matter lesions.
Long-term outcome in later childhood and adolescence
Data on long-term outcome are scarce and often lack sophisticated neonatal neuroimaging data or other early biomarkers, such as neurophysiology (including aEEG and evoked potentials). Data that are available tend to include children, where asphyxia was based on Apgar scores or often incomplete Sarnat criteria. In a recent study Lindström et al48 looked at 15–19-year-old children with moderate encephalopathy in the neonatal period and found that the majority of children had cognitive deficits (81%). The children were considered to be eligible for the study, based on an Apgar score <7 at 5 min and meeting clinical criteria for moderate NE. Of 56 eligible children, 13 did not agree to participate. Of the 43 children who did participate, 13 (30%) had CP, 22 (51%) had cognitive dysfunctions without CP and only 8 (19%) had no obvious impairments. A previous study, using diffusion tensor imaging, showed long-term white matter disturbances which are not repaired by adolescence with moderate HIE in a small group of eight teenagers.49
A hospital-based cohort of 164 full-term infants with NE following PA, admitted to our level three Neonatal Intensive Care Unit of the Wilhelmina Children's Hospital in Utrecht between 1993 and 1997, was studied in detail at 9–10 years of age. In the neonatal period 46 children (28.0%) died including all children with severe NE. All survivors were seen in the follow-up clinic up to 18 months of age and those with an abnormal neurological outcome were seen until 5 years of age. Of the 118 survivors, 80 were finally examined at 9–10 years of age. Of the children not examined, six were too severely affected to participate, seven (mild NE 5, moderate NE 2) could not be traced and the parents of 25 children (mild NE 13, moderate NE 11) refused to participate mainly due to MRI being part of the protocol.
The children (mild NE, n=34; moderate NE, n=46) included in this study were invited to the hospital for neurodevelopmental assessment, including general motor functioning (Movement Assesment Battery for Children (ABC) test), general intellectual functioning (Wechsler Intelligence Scale for Children III Dutch version), extensive behavioural and memory testing and an MRI scan. Thirty-three children had both a neonatal and childhood MRI and there was a good correlation for site and pattern of injury between the two scans.50 Children with moderate/severe lesions on the neonatal or childhood MRI (BGT/WS or focal infarction) had significantly more often a total impairment score on the Movement ABC test ≤p15, and a score of ≤85 on the Wechsler Intelligence Scale for Children III. They more often developed CP and more often attended special education. In a subgroup (n=61) of the same cohort and in 47 controls the area of the corpus callosum (CC) was measured and related to the Movement ABC test score.51 Children with moderate NE had significantly smaller middle and posterior parts and total areas of the CC. Children with mild NE and moderate NE scored significantly worse on the Movement ABC test than controls. The poorer motor skills in children with NE could be partly explained by a smaller size of the CC.
In the same cohort we were able to show that both mild and moderate NE have a negative effect on daily life behavioural functioning at the age of 9–10 years.52 Behavioural problems were assessed using the Child Behaviour Checklist, Teacher's Report Form, Diagnostic Interview Schedule for Children IV and the Children's Social Behavior Questionnaire. At the level of daily life behavioral functioning, overall, both children with mild NE and moderate NE were judged by their teachers as showing more problematic behavior than comparison children, but the difference was significant only for children with moderate NE. There were no significant differences between the groups in the prevalence of attention deficit hyperactivity disorder classifications according to the Diagnostic Interview Schedule for Children IV criteria. In contrast, scores on the Teacher's Report Form F indicated higher levels of attention problems in children with moderate NE than in the comparison group. One other previous study reported an elevated rate of Autism Spectrum Disorders in children with moderate and severe NE with heterogeneous aetiology.53
We finally found, in addition to a global effect of NE on general intellectual functioning in both mild and moderate NE, specific negative effects on memory, associated with the degree of NE. Compromised maintenance and retrieval of information in verbal, visuospatial and verbal associative long-term memory, and speed of working memory processes were related to moderate NE, while mild NE was related to normal short term and working memory functions, and slightly weakened verbal learning capacity.54
Conclusions
It has become increasingly clear that childhood survivors of NE, in the absence of CP, are at increased risk of cognitive, behavioural and memory problems. Although most children with mild NE studied so far were not found to significantly differ from controls, we found them to be performing in between the controls and those with moderate NE, suggesting a gradual effect. Longitudinal monitoring of educational and behavioural development is therefore recommended in both children with mild and moderate NE. This also applies to the infants who participated in the recent multicentre trials using hypothermia. The protective effect of hypothermia can only be fully appreciated when these children will be followed into childhood. We can only hope that in the future there will be more population based case–control studies of NE, starting in the neonatal period with sophisticated neuroimaging and neurophysiology and continuing into childhood and adolescence with detailed neurodevelopmental assessment.
Acknowledgments
We appreciate all the researchers whose work has been discussed in this review—in particular we thank Dr Floris Groenendaal, Drs Mariëlle van Handel, Leon van Sonneville and Hanna Swaab for their particular contributions.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.
-
Patient consent Parental consent obtained.
-
Ethics approval This study was conducted with the approval of the University Medical Centre Utrecht.