Article Text

Abstract
Premature birth is not normal. Very preterm birth results from major disturbance of pregnancy at a time of rapid growth and development. This review looks at outcomes of premature birth at various stages of life with a view to developing and benchmarking perinatal services.
- CP, cerebral palsy
- IQ, intelligence quotient
- VLBW, very low birthweight
Statistics from Altmetric.com
Being born prematurely is not a normal event, despite its routine nature today. Very preterm birth results from a major disturbance of pregnancy at a time when the fetus should be growing rapidly, with all the body systems maturing rapidly and the brain developing at its fastest. It is perhaps surprising then when babies born after a greatly curtailed pregnancy develop into entirely normal adults, which is certainly possible.1,2 Sadly this is not true for all such births, and the issues of survival and disability remain important in developing and benchmarking perinatal services.
All neonatal intensive care services should run a follow up service and collate outcomes.3 Such clinics are rarely funded by health commissions but, increasingly in an era of early interventions, it is recognised that support and active management in this group may resolve or ameliorate potential later problems, being an important identifiable source of disability in the population. In this paper, I will review outcome data from various reports to 2 years of age, school age, and teenage/adult in the context of the clinician practising in the follow up clinic.
DEFINITIONS
Most studies are defined by birth weight, and the vast majority relate to birth ⩽ 1500 g or ⩽ 1000 g (very low birthweight (VLBW) or extremely low birthweight respectively). Although these identify very preterm children, these are far from consistent populations because of the impact of low weight for gestational age, which is managed with increasing aggressiveness by obstetricians in the hope of early delivery reducing perinatal death or neonatal complications and improving later outcome. The evidence for this is still wanting.4 It is thus better practice to define outcome by gestational age and then to study the effect of fetal growth restriction in these defined populations. Generally “very preterm” refers to babies born at 30 weeks or less and “extremely preterm” to babies born before 26 weeks gestation.
The definition of disability is currently undergoing major changes,5 but most papers define their rate of disability using aggregate groups comprising cerebral palsy (CP), poor cognitive performance (usually developmental quotient (DQ) or intelligence quotient (IQ) < 70), and severe visual or hearing impairment. Although the definitions may not be exactly comparable, each is only a point estimate. The problem of comparing data between different populations has been much discussed and may lead to incorrect conclusions. A standardised set of definitions has been published following professional consensus, and these are gaining acceptance in the United Kingdom as a means of producing consistent functional descriptions of outcomes at 2 years.6–8 Although these definitions of severe disability seem stringent, they have been arrived at with the view of identifying children who will have continuing severe disability, and their performance in this regard is awaited. Similar thought has been applied to CP, and a template for classification has now been published,9 to which reports should adhere. A consensus to define disability and other functional measures for later ages would be helpful.
There is some confusion over the need to correct chronological age for prematurity after birth. It is self evident that proper assessment of growth and development over the first year must take account of prematurity, and most authorities recommend that the correction is continued until 2 years of age. At this age, after birth at 28 weeks gestation, correction produces a 12% difference in terms of developmental age. This is an important clinical difference compared with the assessment based on chronological age. For more immature children, this correction could be continued longer than this, as the difference will be significant up until 3 years (24 weeks gestation: 11% difference). However, by the time a preterm child reaches nursery or school, the comparison is with peers of the same chronological age, and continuing to make these corrections is then really irrelevant to their situation and makes only a small and clinically insignificant difference to scores.
OUTCOMES OVER THE FIRST 2 YEARS
Given the resource implications and the poor relation between outcomes and perinatal care for some of the more subtle measures, most services will provide follow up for two years.6 At this age, most serious neurological and sensory disability is likely to be identified. At younger ages, it is believed that the diagnosis of disabling CP in particular may not be accurate,10 and the subject of transient neuroimpairment (dystonia) around 12 months of age has been well described.11
Cerebral palsy
The most commonly quoted outcome after very preterm birth is CP (table 1). It is more common as gestational age decreases and in boys. It is usually of the diplegic type, with increasing severity of disability distributed caudally, resulting from injury to the internal capsule (periventricular leucomalacia). Other distributions are identified, but less often and may relate to other focal brain injuries, such as cerebral venous infarction in association with large intraventricular haemorrhages, or to hydrocephalus. Because one would expect neurological signs to correlate with observable brain lesions, attempts to describe the relation of CP to observed brain injuries are common. However, using cerebral ultrasound, this relation is not absolute,12 and the precise distribution of injury needs to be taken into account.13,14 The practice of using cerebral ultrasound as a screening tool with three or four fixed assessments during the neonatal period, and the reporting of broad gradings may miss important prognostic information, and more frequent expert assessments may lead to better correlation.15 The use of magnetic resonance imaging techniques will undoubtedly enhance the understanding of the relation between acquired brain injury and disability.15 CP occurs in 8–10% of VLBW infants in most reviews, although some populations seem to be less vulnerable than others. In extremely preterm infants, the prevalence at 2 years is likely to be higher.16 There is no evidence that these overall rates are changing significantly, although as more immature children survive, there is evidence that there is an initial rise in birthweight specific prevalence of CP, followed by a levelling out as care reaches the optimum.17
Adverse neurocognitive outcomes observed after very preterm birth
Developmental outcome
Despite the perceived importance of CP, the most common disability at 2 years is developmental or cognitive impairment, which assumes greater significance in the school years. A range of developmental tests are available at 2 years, but few show good correlation with later formal measures of cognitive function. It is critically important to use recently standardised measures of cognitive function, as there is a well described secular upwards drift in IQ scores with time,18 and the use of old standards may underestimate the disability in this area.19 Similarly, it is also important to use contemporaneous comparison data from socially equivalent populations. Most studies now use the Bayley scales of infant development (BSID-2E) or the Griffiths scales, both of which have recent standardisations. We have recently validated an adapted parent report questionnaire20 against the Bayley scales at 2 years in 64 very preterm children.21 This has high correlation (r = 0.68) and good diagnostic utility (sensitivity 81%; specificity 81%) for a BSID-2E mental development index (MDI) of < 70 and is probably as accurate as repeating the developmental assessment with another observer. This may prove a useful tool in the routine follow up of preterm populations or for use in multicentre trials, in which follow up is critical but very expensive.
When reporting developmental or other continuous outcomes, it is critical to include the whole population, as the mean scores will be affected by the exclusion of children who function below the lower limit of the test. For example, with the age banding used in the 2½ year assessment as part of the EPICure study of 283 children of 25 weeks gestational age or less,16 33 children (11.7%) had scores lower than 50. Without this group, the mean (SD) BSID-2E MDI of these was 82 (12) or 1 SD below the standardisation mean. Nominally assigning a score of 40 to the excluded children brought this down to 77 (18). Reports should also include appropriate categorisation of outcome. In the EPICure study, 19% had scores below −3SDs (profound developmental impairment) and 11% between −2 and −3SDs (severe developmental impairment), and a further 20% had mild impairment (scores 70–84), leaving 50% of the population unimpaired. As gestation increases beyond 26 weeks, the proportion who are impaired decreases, but generally, even after correcting for prematurity, the means in various studies remain impaired by at least 0.5SD.
Other severe disabilities
The prevalence of severe impairments of hearing or vision remains reassuringly low, although less severe problems are not uncommon. Neonatal screening is well established for both, and for retinopathy of prematurity, laser coagulation provides a valuable intervention with good ocular results. In the EPICure study, 15% of children received laser therapy or cryotherapy in the neonatal period, but only 3% were blind at follow up.
Trends in disability
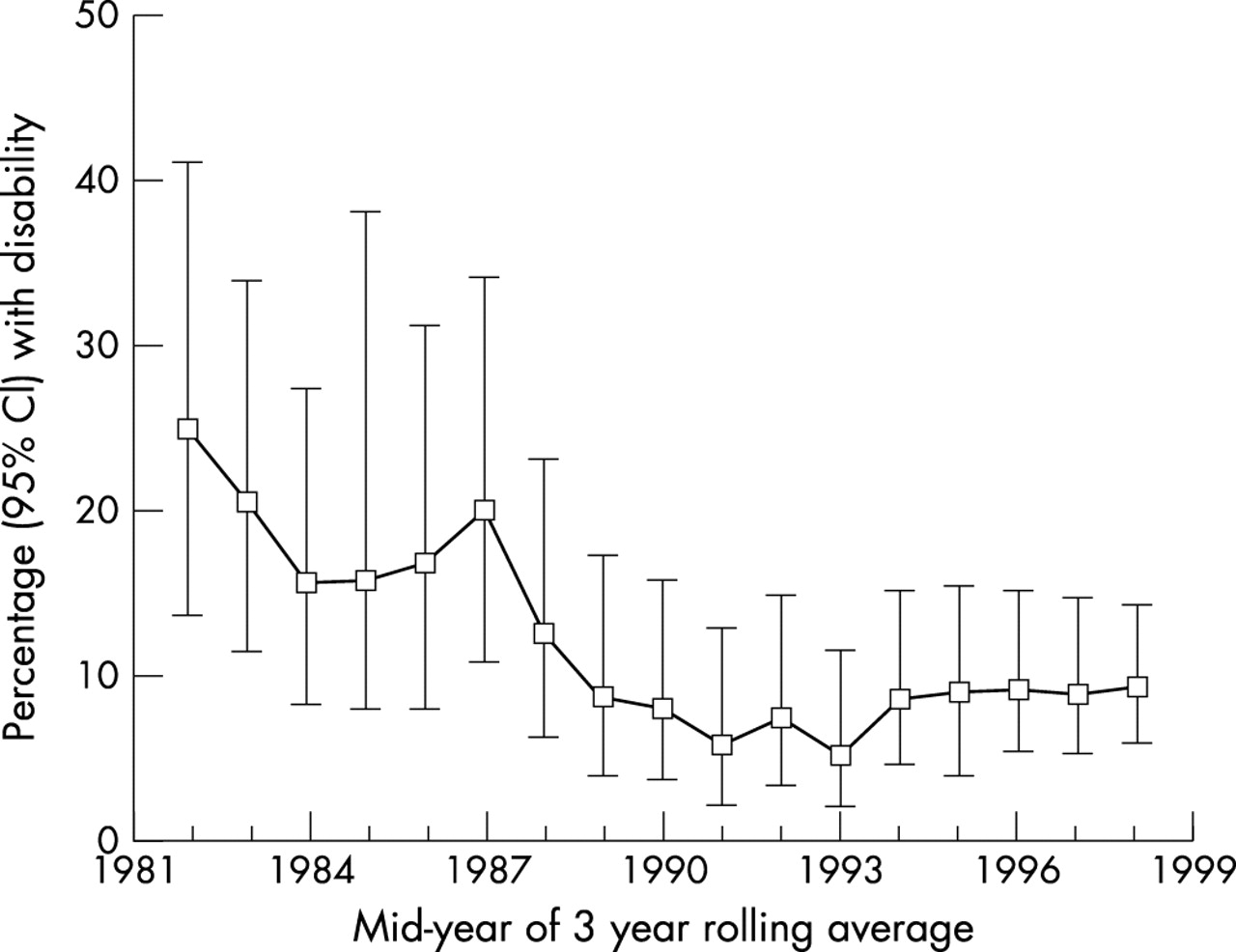
Working out what has happened to disability rates over time has proved difficult. Figure 1 shows the range of estimates in reports of CP in populations of babies weighing less than 1001 g at birth. Figure 2 shows similar estimates for babies of 26 weeks gestation or less. No clear trends are seen. In contrast, the Nottingham Passport to Health scheme has provided hospital based follow up since 1981, using identical follow up practices. The number of babies cared for has risen considerably over that time, but the numbers with severe disability fell from 25% to 5% from 1981 to 1994, after which there was a small rise to 8–9% in succeeding years (fig 3). Although these data show improvements from the early days of modern neonatal intensive care in Nottingham, there seems to be a minimum of 8–10% which is consistent across reports from other centres. Figures based on gestational age, such as EPICure, show less certain trends than most studies based on birth weight.


{kind=link}
{kind=link}
{kind=link}
Disability rates for children of birth weight ⩽ 1000 g cared for by the Nottingham Neonatal Service between 1981 and 1999 as three year rolling averages, with 95% confidence intervals (CI) for each estimate (E Knight Jones, N Marlow, Nottingham Neonatal Service Passport to Health Scheme, unpublished data).
The contribution of preterm birth to population disability rates has often been discussed with the implication that increasing survival at extremely low gestations simply increases the burden of disability in the population as a whole. This is a difficult line to travel down, as the arguments are extremely tenuous and to a large extent depend on the balance between non-disabled and disabled survivors; this in turn depends on the ethical framework of the society in which we practice. For example, in cohorts born in the mid-1980s, the near universal initiation of intensive care in the United States compared with the selective policy practiced in the Netherlands resulted in 24.1 additional survivors and 7.2 additional cases of CP for each 100 live births.34 The increasing contribution of changes in low birthweight survival on the prevalence of CP was shown most clearly by Pharoah and colleagues,17 who used the Mersey Regional CP Register to show increases in birthweight specific prevalence of CP as survival in each category improved; prevalence then stabilised in parallel with survival. Hagberg and colleagues35 have sequentially reported the changes in epidemiology of CP in Sweden. No dramatic changes have been described, and in the birth years 1991–4, the live birth prevalence for CP continued a trend to decrease slightly. Gestational age specific prevalence increased marginally in extremely and very preterm births, but continued to decrease in moderately preterm births and decreased slightly in term births.
The recent changes in consent and data protection in the United Kingdom pose a real threat to the continuance of registers for CP and other perinatal conditions. The data that are held in these registers are critical to understanding population trends; we must support the continuation of these important epidemiological tools.
SCHOOL AGE OUTCOMES
That service based follow up stops at 2 years of age for most services reflects resources and not the extent of problems facing the ex-preterm child. For a long time it has been clear that educational, psychological, and behavioural problems are prevalent during the school years.
Cognition
Bhutta and colleagues36 identified 16 studies of ex-preterm children followed beyond 5 years of age and subjected them to a systematic review. In terms of cognitive outcomes, the ages of assessment ranged from 5 to 14 years. The weighted mean difference in scores was 10.85 (95% CI 9.23 to 12.47); this was unaffected by age, the country of origin, or the type of base population. Inclusion of severely disabled children by the allocation of nominal very low scores was associated with greater differences, as would be expected. In the preterm group, there appeared to be an association between mean scores and gestational age or birth weight. No allowance for the specific test was possible. In the Bavarian VLBW study,37 there appeared to be a linear relation between mean IQ and gestational age, which rose to an inflection point at about 32 weeks, after which IQ scores were not related to gestational age.
These important cognitive differences are reflected in school performance, with greater need for educational support and higher prevalence of measures of school failure in children who have no severe disabilities.38 In two European studies using similar definitions of school failure at 8–9 years of age, 19–22% of VLBW children were in special education, a further 22–26% had been held back one year, and 11–15% received special help in regular school.39,40 There is little evidence of a consistent pattern of educational failure across the various studies. Despite suggestions that there are specific learning problems in ex-preterm children,41 most of the learning difficulties seem to be related to low overall IQ.42 Nonetheless, the potential need for extra educational support should be pointed out to schools so that early assessment and intervention can occur. Such assessment must be comprehensive, including visual-motor and visual-perceptive abilities, complex language performance, and attentional skills in addition to conventional academic abilities.43
Although the literature concentrates on very preterm or VLBW populations, Huddy and colleagues44 found that up to a third of 117 children born at 32–35 weeks gestation had special educational needs. Furthermore 20–25% of children with CP weighed 1500–2500 g at birth, and encephalopathic symptoms may occur in a considerable proportion.45 Clearly, as 5% of the population is born preterm, and effective early educational intervention has been shown to have persisting benefit only for this group of children,46 educational resources should be concentrated on them in the early years.
Behaviour
Behavioural and other psychological outcomes seem to be equally problematic. Bhutta and colleagues36 identified 16 studies of behavioural outcome between 5 and 14 years of age, which mainly comprised parent report measures of behaviour. There was inconsistency as to whether there was reported excess of externalising or internalising behaviours in the preterm group compared with controls, but all confirmed the excess of attention deficit hyperactivity disorder. When formally defined criteria for its diagnosis were used (six studies), meta-analysis indicates a relative risk of 2.64 (95% CI 1.85 to 3.78) for the disorder among preterm children. One study has compared behaviour of extremely low birthweight children across four countries (Germany, the Netherlands, Canada, United States) using the child behaviour checklist.47 Total problem scores were only higher in European countries, but scale scores for social, thought, and attention difficulty were 0.5–1.2SD higher in extremely low birthweight children than in others. In these studies, internalising and externalising items were not significantly different from controls.
Parent report measures are usually used to determine these measures. These parent perceptions should be supplemented by more objective teacher report measures, or composite measures that identify where parent and teacher agree, as criteria referencing behavioural descriptions are clearly difficult for parents. Similarly, the quoted prevalence of a disorder must be related to standardised definitions, such as the Diagnostic and statistical manual of mental disorders 4th edition (DSM-IV), to facilitate interstudy comparison, something that is rarely reported. Botting and colleagues48 reported a study of VLBW teenagers in which a battery of parent report scales were supplemented by a direct interview using the child and adolescent psychiatric assessment (CAPA). This carefully conducted study identified attention deficit disorder from DSM-IV criteria in 28% of children at mainstream school and, in contrast with the usual association with conduct disorders, found an association with internalised symptoms of anxiety and depression.
Understanding the underlying processes by which the ex-preterm child fails to achieve has proved difficult. Clearly, attention deficit is a candidate unifying mechanism. Studies of late magnetic resonance images in relation to outcome have not shown good correlation between brain injuries or regional measures of size.49,50 There is, however, evidence that the very preterm brain at term is less complex in terms of its cortical development, and this is reflected in measures of regional brain volumes in later childhood; compared with conventional measures of acquired brain injury, hippocampal and caudate nucleus volumes seem to be better associated with subtle measures of outcome, such as cognitive and attentional measures.51,52 The pervasive insult provided by preterm birth and subsequent development outside the womb clearly has major effects on brain organisation and development, which await elucidation.
Other problems
Although I have concentrated on neuropsychological outcomes, the surviving preterm child is at risk of a range of other deficits ranging from motor difficulties (clumsiness),11 visual impairments (an excess of squints, refractive errors, stereo vision, and contrast sensitivity),53 growth disorders,54–56 and respiratory problems.47 The contribution of these problems to behavioural and cognitive disorders is difficult to determine, although often they coexist. Similarly the influence of perinatal illness, excluding brain injuries, on later outcomes is very difficult to assess. Studies of children with chronic lung disease, for example, have obtained conflicting findings in terms of later neurocognitive outcomes. It is unlikely that, once other population differences such as gestation and brain imaging results have been accounted for, neonatal respiratory disease significantly influences later psychological outcomes. The role of postnatal steroids in long term disability has received much attention. Early use of steroids, often in long courses, is associated with considerable neurodisability.58 The results of studies into shorter courses, started later and at lower doses, are still not convincing either way, and further research is required before their use is completely abandoned.
TEENAGE/ADULT OUTCOMES
In a study of functional outcomes in 10–14 year old children from Cleveland in the United States, 86% of the group of < 750 g birth weight were found to have some functional limitation (growth disorders (49%), mental or emotional problems (58%), restrictions on physical activity (32%), and visual impairment (31%)), 75% used aids such as medication or spectacles, and 66% accessed non-routine services.59 In contrast, in a study from Hamilton Ontario, the health related quality of life of extremely low birthweight children was considerably better than expected; although the scores were significantly lower than for term peers, the proportion scoring in the normal range (> 0.95) was similar in both groups.60
Hack and colleagues1 have also reported adult outcomes for a VLBW cohort. In my view, this should be mandatory reading for all involved in the care of preterm infants, as it sets the outcome in terms of actual integration into society. Although it is clear that the risks of the conditions described above do not disappear during adolescence, the differences from term children do not increase, and a large proportion have academic achievements at least equivalent to their peers. Although fewer go on to higher education, the VLBW population are less likely to engage in risk taking behaviour, suggesting that their social integration is not substantially impaired, contradicting the predictions from older studies of sociopathic behaviour.61
IMPLICATIONS FOR PRACTICE
Care after discharge is a critical part of the neonatal intensive care service, for a range of reasons. As neonatologists, we have a duty to examine the outcome of children managed within our practice. Only by having first hand knowledge of these outcomes can we be properly informed when we approach parents for counselling. Benchmarked data allow us to consider our performance relative to other services and to our own over time (figs 1 and 3 respectively). There is a need to provide continuity and support for parents, who are known to be less securely attached to their VLBW child and for whom informed support for health decisions such as immunisation and feeding practices is invaluable. Most important of all, the early identification of disability and impairment in the child is vital. This is best accomplished by the neonatologist until the risk of the child developing severe disability is past. Then stage managed transfer to community supervision is necessary to ensure that the very preterm child is supported in the important preschool years and into early school life. Careful developmental assessment and early intervention for evolving impairments by a doctor aware of the potential sequelae of prematurity are critical to optimal development for the individual child.