Article Text

Abstract
OBJECTIVES To determine the neurosensory outcome at 14 years of age of a regional cohort of extremely low birthweight (ELBW) children, to contrast their prognosis with normal birthweight (NBW) controls, and to determine the predictive value of assessments earlier in childhood.
DESIGN Geographically determined cohort study.
SETTING The state of Victoria, Australia.
PATIENTS Consecutive ELBW survivors of birth weight 500–999 g (n = 88) born during 1979–1980, and 60 randomly selected contemporaneous NBW (birth weight > 2499 g) controls.
MAIN OUTCOME MEASURES Rates of neurosensory impairments and disabilities at 14 years of age, and earlier in childhood.
RESULTS Of 351 ELBW consecutive live births, 88 (25%) survived and 79 (90%) of the survivors were assessed at 14 years of age. Of the 79 ELBW children assessed, eight (10%) had cerebral palsy, five (6%) had bilateral blindness, four (5%) were deaf requiring hearing aids, and 36 (46%) had an intelligence quotient (IQ) < −1 SD compared with the mean for the NBW controls. Overall 11 (14%) ELBW children were severely disabled, 12 (15%) were moderately disabled, 20 (25%) were mildly disabled, and 36 (46%) had no disability. In contrast, only one (2%) of 42 NBW children assessed had a severe disability, six (14%) had a mild disability, and the remaining 35 (83%) were not disabled. Comparing psychological test scores for ELBW children with those for NBW controls, rather than test norms, avoided bias in the assessment of disability earlier in childhood. Relative to assessments earlier in childhood, the prediction of disability at 14 years of age was highly significant at each of 2, 5, and 8 years of age, but the accuracy progressively increased with age.
CONCLUSIONS ELBW children have substantially higher rates of neurosensory impairments and disabilities at 14 years of age than NBW controls. Comparison of ELBW children with NBW controls avoids bias in the assessment of disability. Early childhood assessments are highly predictive of disability at 14 years of age.
- impairment
- disability
- cerebral palsy
- low birth weight
Statistics from Altmetric.com
As survival rates improve dramatically for extremely low birthweight (ELBW, birth weight < 1000 g) children, their long term quality of life assumes even more importance. Of the outcomes that contribute to poor quality of life, neurosensory impairments and disabilities are among the most important. There are few studies that have reported on the comparative outcome for contemporaneous normal birthweight (NBW, birth weight > 2499 g) controls to provide a baseline for the rates of impairments and disabilities in ELBW children. Moreover, many studies have reported on neurosensory outcome early in childhood, on the assumption that what is found at that time will persist throughout the rest of the child's life. Yet, given the paucity of data on outcome later in childhood, this assumption remains to be proven.
The aim of this study was to determine the neurosensory outcome at 14 years of age of a regional cohort of ELBW children, to contrast their prognosis with NBW controls, and to determine the predictive value of assessments earlier in childhood.
Methods
The ELBW cohort comprised 88 consecutive survivors from 351 live born children with birth weights 500–999 g born in the state of Victoria in the calendar years 1979 and 1980. The outcome for these children earlier in childhood has been reported at 2,15,2 and 83 years of age. Since the 8 year assessment, one severely disabled child had died, leaving 88 survivors to 14 years of age. The 60 NBW controls comprised children with birth weights > 2499 g who were randomly selected from births during 1981–1982 in the Royal Women's Hospital, one of the three level III perinatal centres in Victoria, as described elsewhere.4 All children were born before exogenous surfactant was available. Survivors were all cared for in one of the four level III neonatal units that serve the state of Victoria, which has about 60 000 births annually. Other details of care around the time of birth for the ELBW cohort have been described elsewhere.1
Children were assessed at 14 years of age, corrected for prematurity where appropriate, by paediatricians and psychologists who were unaware of perinatal details of the children or of the results of assessments earlier in childhood. We have previously described the rationale for using age corrected for prematurity for psychological test scores in preterm cohorts.5 The paediatrician determined impairments such as cerebral palsy, blindness (visual acuity < 6/60 in both eyes), and sensorineural deafness requiring hearing aids. The psychological assessment included the Verbal Scale of the Wechsler Intelligence Scale for Children-3rd edition (WISC-III).6Children were considered to have an intellectual impairment if their verbal IQ was more than 1 SD below the mean (< −1 SD). The severity of disability imposed by any impairment was categorised as follows: severe, any of non-ambulatory cerebral palsy, blindness, an IQ < −3 SD, or if they were untestable by the WISC-III because of severe intellectual impairment; moderate, ambulatory cerebral palsy with considerable limitation of movement, sensorineural deafness requiring hearing aids, or an IQ score from −3 SD to < −2 SD; mild, ambulatory cerebral palsy with minimal limitation of movement, or an IQ from −2 SD to < −1 SD. The remaining children were considered non-disabled. The classification of disability at earlier assessments was recoded to match the classification at 14 years of age, as there were subtle differences in the classifications at 2, 5, or 8 years of age in our earlier reports. At age 2 years, developmental quotients based on the Mental Developmental Index (MDI) of the Bayley Scales of Infant Development7 had been used to classify disability rather than IQ scores. At 5 years of age, the psychological test had been the Wechsler Preschool and Primary Scale of Intelligence (WPPSI),8 and at 8 years it had been the Wechsler Intelligence Scale for Children–Revised (WISCR).9 To determine whether classification of disability should be based on the psychological test norms or the NBW controls, we recalculated disability rates using the mean of psychological test scores for the NBW controls at each age to establish the SD ranges. All psychological test scores were expressed as SD scores from both the mean from the manual (100 for all tests) and the mean of the NBW controls, as the SD ranges were not identical for all tests (SD 16 for the MDI, SD 15 for the other tests). A child with a psychological test score at the mean would have a test score of 0, a child above the mean would have a positive test score and a child below the mean would have a negative test score. SD scores can be converted back to developmental quotient (DQ)/IQ points by multiplying by the SD for the appropriate test.
Years of mothers' schooling were noted and social class was determined by the occupation of the main income earner in the family by the Daniel scale,10 in which a lower score indicates higher social class.
Data were edited and analysed using SPSS for Windows programs.11 Univariate analyses included χ2tests for dichotomous variables, and mean differences and 95% confidence intervals (CI) for normally distributed continuous variables. Differences in ordered proportions were contrasted by Mann-Whitney U test.12 Kappa statistics were computed to determine the predictive accuracy of assessments earlier in childhood, and the McNemar test assessed any bias in assessments between earlier ages and 14 years of age. The relation between psychological test scores earlier in childhood and those at 14 years of age was analysed by least squares linear regression. p < 0.05 was considered significant.
Results
Table 1 shows some of the perinatal characteristics of the two cohorts. As expected, the ELBW cohort was less mature and smaller at birth, and had more perinatal morbidity. Sociodemographic variables, including sex, years of maternal schooling, and social class, were similar in the two cohorts.
Perinatal and sociodemographic data in extremely low birthweight (ELBW) and normal birthweight (NBW) children
Of the 88 surviving ELBW children, 79 (90%) were assessed at 14 years of age, as were 42/60 (70%) of the NBW controls. Of the nine surviving ELBW children not assessed at 14 years of age, two were lost, one was inaccessible, two refused outright, and the other four refused but provided some information by telephone or mail. All nine had similar birth weights (886 g v 871 g respectively) and gestational ages (27.9 weeks v 27.0 weeks respectively) to the ELBW children who were assessed at 14 years of age. All had been assessed at 8 years of age, and all but one had also been assessed at 2 and 5 years of age; none had cerebral palsy, blindness, or deafness at any age. When last assessed at 8 years of age, three were not disabled, five were in the mild disability range, and one was in the severe range on IQ scores relative to the NBW controls. Of the 18 NBW children not assessed at 14 years of age, four were lost, two were inaccessible, 11 refused outright, and one refused but provided some information by telephone or mail.
Table 2 shows the results for psychological test scores at each age for ELBW and NBW children. NBW children had substantially higher test scores than ELBW children at each age, and the mean differences between the groups were of similar size at each age. Moreover, the NBW children had significantly higher psychological test scores than the expected mean of 100 for each test at age 2 (higher mean difference in MDI 5.8, 95% CI 1.1 to 10.6), age 5 (higher mean difference in WPPSI 13.8, 95% CI 9.1 to 18.6), and age 8 (higher mean difference in WISC-R 9.6, 95% CI 5.3 to 14.1), but not age 14 (higher mean difference in WISC-III, Verbal Scale 3.2, 95% CI −1.2 to 7.5).
Psychological test scores in those able to be tested at each age for extremely low birthweight (ELBW) and normal birthweight (NBW) children
The rates of all neurosensory impairments (cerebral palsy, bilateral blindness, deafness, and intellectual impairment) at 14 years of age were substantially higher in ELBW children than NBW controls, but not all differences were statistically significant (table 3). Of the eight ELBW children with cerebral palsy, one had mild diplegia, four had quadriplegia (one mild, one moderate, and two severe), one had mild ataxia, and two had mixed spastic cerebral palsy (one mild and one moderate). The one NBW child with cerebral palsy had severe quadriplegia. The overall rate of neurosensory disability imposed by the impairments was significantly higher in ELBW children than NBW controls (table 4; Mann-Whitney U test, Z = 4.0, p < 0.0001).
Comparison of neurosensory impairments at 14 years of age in extremely low birthweight (ELBW) and normal birthweight (NBW) children
Comparison of neurosensory disabilities at 14 years of age in extremely low birthweight (ELBW) and normal birthweight (NBW) children
For ELBW children assessed at all ages (n = 73), rates of blindness, deafness, and developmental/intellectual impairment were similar over time (table 5). However, cerebral palsy was more commonly diagnosed at 2 years of age than later in childhood. Cerebral palsy was diagnosed in the same children from age 5 years onwards. However, five children with mild cerebral palsy at 2 years of age no longer had cerebral palsy at any later age, and one child not diagnosed with cerebral palsy at 2 years had mild cerebral palsy at all later ages. The children seen at all ages with severe cerebral palsy remained constant at all ages, but there was some minor change in the classification of disability caused by the cerebral palsy after 2 years of age (table5).
Neurosensory impairments at ages 2, 5, 8, and 14 years in extremely low birthweight (ELBW) children assessed at all ages (n=73)
Of the six ELBW children assessed at 14 years but not at all other ages, none were blind or deaf. Two children had cerebral palsy at 14, one moderate and one mild, but both were severely disabled on the basis of a low IQ score relative to the NBW controls. The four remaining children had no cerebral palsy; three were mildly disabled and the remaining child was moderately disabled on IQ scores.
For ELBW children assessed at all ages, relative to assessments earlier in childhood and based on cut off scores for psychological tests from the respective test norms, the prediction of disability at 14 years of age was highly significant at 2, 5, and 8 years of age, and the accuracy progressively increased with age (table 6). However, the rate of disability at 14 years of age was significantly underestimated at 5 years of age. Relative to assessments earlier in childhood and based on cut off scores for psychological tests from the NBW children, the prediction of disability at 14 years of age was highly significant at 2, 5, and 8 years of age, and again the accuracy progressively increased with age (table 7). There was, however, no longer any significant underestimate or overestimate of disability at any age.
Comparisons of assessment of disability earlier in childhood with that at 14 years of age
Comparisons of assessment of disability earlier in childhood with that at 14 years of age
Using the NBW controls as the basis for comparison, the reasons for changes in classification between earlier assessments and 14 years of age were predominantly because of changes in psychological test scores, rather than in other impairments. Compared with results at 14 years of age, disability was overestimated at 2 years of age in 18 children and underestimated in 13 children, all on psychological test scores. Four children also had mild cerebral palsy at 2 years of age that disappeared by 14 years of age. Disability was overestimated at 5 years of age in 11 children, all on psychological test scores, and underestimated in 15 children, in 14 on psychological test scores and in one with mild cerebral palsy at 5 years of age assessed as moderate at 14 years of age. Disability was overestimated at 8 years of age in 13 children and underestimated in nine children, all on psychological test scores.
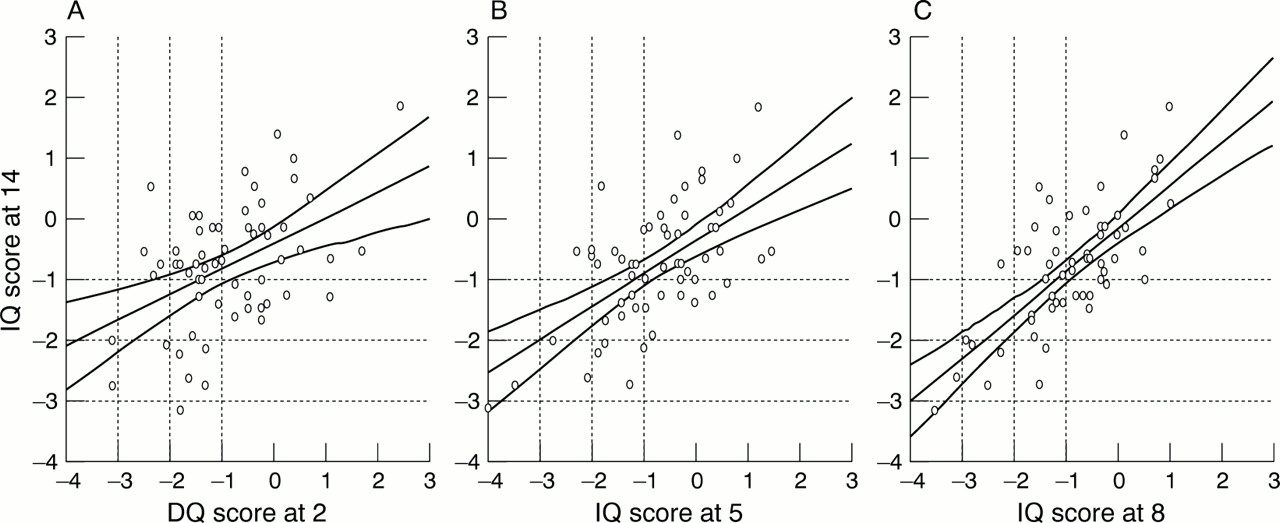
Figure 1 shows the relations between psychological test scores in ELBW children at ages 2, 5, and 8 years and those at 14 years of age, and also the variability between ages. The statistical significance of the linear relation between psychological test scores earlier in childhood and those at 14 years of age increased with age, as evidenced by the increasing percentage of variance explained by the linear relation with age.

{kind=link}
Intelligence quotient (IQ) at 14 and psychological test scores at 2, 5, and 8 (only those with data at all ages included; no nominal IQs or developmental quotients (DQs) included; n = 61). Percentage of variance explained by the linear relation was 20.7 in (A), 34.1 in (B), and 51.3 in (C). Dotted lines indicate SD cut off points.
Discussion
There have been criticisms regarding the quality of follow up studies.13 ,14 Some of the problems include small sample sizes and large losses to follow up, with attrition rates greater than 25% reported.15-17 Subjects more difficult to follow often have more disability, and studies with low follow up rates will underestimate disability rates.14 ,16-18 In our study, 90% of 88 ELBW survivors were followed up at 14 years of age, which is a high follow up rate, particularly considering the duration.
There are other strengths of this study of the prognosis of ELBW infants, apart from the high follow up rate. The ELBW cohort was geographically based. Outcome was determined at 14 years of age, enabling a more certain estimate of neurosensory morbidity than studies of outcome earlier in childhood. There were contemporaneous NBW controls which allowed a basis for comparison of the outcome measures with ELBW children. Few other studies have been as rigorous in determining the prognosis for ELBW children.
The overall rate of neurosensory disability was significantly elevated in ELBW survivors in our study, consistent with other studies showing major neurosensory disabilities in up to 20% of school aged ELBW survivors.18-20 In other studies, rates of impairment have been reported to be higher in the ELBW groups than in those with birth weights of 1000–1500 g,21 ,22 a birthweight group that we did not study.
Five children diagnosed with cerebral palsy at 2 years of age no longer had cerebral palsy at later ages, and one child with mild cerebral palsy at all later ages was not diagnosed at 2 years of age. Even though the change in the diagnosis of cerebral palsy was not statistically significant within our study, our findings are consistent with others describing a tendency for overdiagnosis of cerebral palsy in preterm children rather than underdiagnosis early in childhood.23 ,24 This highlights the difficulty in making the diagnosis of cerebral palsy before 5 years of age.25In other children the diagnosis of cerebral palsy was stable over time, although there were some changes in the classification of severity. Given the somewhat subjective nature of the classification of the severity of cerebral palsy, this is not unexpected. Diagnoses of blindness and deafness were stable in children seen at all ages. Overall, the early childhood assessments were highly predictive of neurosensory outcome at 14 years of age, but the accuracy improved substantially with increasing age.
Changes in psychological test scores between ages were the predominant reason for a change in classification of disability over time. This is hardly surprising as psychological test scores were divided at certain points to classify disability, and children could be above the cut off point at one age and below the cut off point at another age. The improved accuracy of the prediction of disability at 14 years of age from assessments earlier in childhood was related to the diminished variability of psychological test scores over time, as shown in fig 1. Others have described a similar accuracy of psychological tests earlier in childhood with psychological tests at 12 or more years of age.26 ,27
Cognitive problems have been reported in other follow up studies of ELBW children to adolescence; Saigal et al 27 reported that 17% had an IQ < −2 SD below the mean, consistent with the rate of 20% (16/79) in our ELBW cohort. The relatively consistent relation between earlier assessments at 2, 5, and 8 years of age and cognitive assessment at 14 years of age in our study has also been shown in other studies of preterm survivors.27 ,28 On the other hand, reports of a fall in IQ from earlier ages to adolescence have been published,26but probably resulted from changes in the assessment tool used, leading to lower subsequent scores.29 Indeed, Bottinget al 26 reported differences in IQ scores at 6 (using the WPPSI) and 12 years of age (using the WISC-III) in both their preterm and control children of similar magnitude to our study between 5 and 14 years of age with the same psychological tests.
Although overall accuracy was not improved by using the NBW controls rather than test norms as the basis for comparison, we consider it more important to avoid bias than just to improve overall accuracy. We would have significantly underdiagnosed cognitive problems at 5 years of age in our cohort if we had relied solely on psychological test norms to classify children, rather than results from contemporaneous NBW controls. Gross et al 30reported a similar elevation of psychological test scores for the MDI on the Bayley Scales7 of control children relative to the published norms. In their study, the control group had a mean MDI of 115 at 2 years of age compared with 106 in the NBW controls in our study. As in our study, they reported less cognitive delay in their preterm cohort when psychological tests were compared with test norms than when compared with the controls.
Cognitive problems have obvious implications for academic performance. Reports of academic achievement in ELBW survivors indicate that they do less well as a group, particularly in mathematics.27 ,31It is important to recognise the higher rate of academic problems in ELBW children to ensure that they are diagnosed and special assistance provided.
There is always a compromise between increasing length of follow up and diminished relevance to contemporary ELBW infants in newborn nurseries. On the one hand, the longer the period of follow up, the more certain are the diagnoses of neurosensory impairments and disabilities. On the other hand, the less relevant the rates become because perinatal care and survival rates have changed dramatically in the interim. However, the estimates of neurosensory impairments and disabilities observed in our cohort still provide the best estimate for what infants in nurseries today will be like at 14 years of age, until superseded by more contemporary cohorts.
Acknowledgments
This work was funded in part by the Department of Health and Community Services, Victoria.
Participants in the Victorian Infant Collaborative Study Group: convenor: Lex W Doyle, paediatrician; collaborators (in alphabetical order): Catherine Callanan, research nurse (the Royal Women's Hospital); Elizabeth Carse, paediatrician (Monash Medical Centre); Daniel Casalaz, paediatrician; Margaret P Charlton, psychologist (Monash Medical Centre); Geoffrey Ford, paediatrician (the Royal Women's Hospital); Marie Hayes, research nurse (Monash Medical Centre); Elaine Kelly, psychologist (the Royal Women's Hospital, the Mercy Hospital for Women); Anne Rickards, psychologist (the Royal Women's Hospital); Andrew Watkins, paediatrician (the Mercy Hospital for Women); Victor Yu, paediatrician (Monash Medical Centre).