Article Text

Abstract
Background The epidemiology of early-onset neonatal sepsis (EONS) varies over time, and requires regular surveillance.
Objective To analyse data on EONS in Australia and New Zealand.
Methods Retrospective analysis of data collected longitudinally from multiple neonatal units from 2002 to 2012.
Results Of 386 423 live births, 454 infants had EONS. The incidence rate of EONS was 1.20 per 1000 live births in 2002 and 0.83 in 2012, decreasing by 4% per year (95% CI 1% to 7%, p=0.007). Group B streptococcus (GBS) (37%) and Escherichia coli (25%) were the most prevalent organisms. The early-onset GBS (EOGBS) incidence rate was 0.43/1000 live births, with no evidence of change over time (p=0.3). Of EOGBS-infected babies, 62% were born at term compared with 8% with early-onset E. coli sepsis, p<0.0001. The mortality of E. coli early-onset sepsis (EOS) (25%) was higher than GBS (11%), but this difference in mortality was no longer significant after adjusting for gestation and birth weight. Mortality from EOS fell significantly over the study period (17% per year, 95% CI 10 to 24, p<0.0001).
Conclusions GBS was the most common cause of early sepsis, but the incidence was lower than prior to the introduction of intrapartum antibiotic prophylaxis, and remained steady over time. The mortality of early-onset E. coli sepsis was significantly higher than GBS sepsis, but this may have been because almost all babies with E. coli were born preterm, rather than a difference in virulence.
- group B streptococcus
- Escherichia coli
- mortality
- ESBL
- antibiotic resistance
Statistics from Altmetric.com
What is already known on this topic?
The aetiology of early-onset neonatal sepsis changes with intrapartum antibiotic use.
Group B streptococcus (GBS) and Escherichia coli are important causes in many countries.
Continuous surveillance allows rational empiric antibiotic use.
What this study adds?
The incidence of early-onset GBS sepsis remained low in our study population of neonatal units attached to maternity hospitals in Australia and New Zealand.
The rate of early-onset sepsis in Aboriginal infants was no longer higher than the rest of the Australian population.
The overall mortality from early sepsis fell over time.
Introduction
Neonatal sepsis is an important cause of morbidity and mortality worldwide. In 2015, infection accounted for 15% of the 2.7 million neonatal deaths globally or some 400 000 deaths.1 An estimated 150 000 babies die from sepsis on the first day after birth and 300 000 by the end of the first week.1 The vast majority of these neonatal deaths occur in low/middle-income countries.2–5 However, neonatal infection is also important in resource-rich countries, including Australia6–9 and New Zealand.10 11
Neonatologists draw an important distinction between early-onset and late-onset neonatal infections for clinical and preventative reasons. Early-onset neonatal infection is primarily due to organisms acquired from the maternal genital tract, usually by ascending amniotic infection or peripartum and less commonly by haematogenous spread. Late-onset neonatal infection can occur as a result of invasive procedures of nosocomial infection or of invasion by organisms acquired peri or post partum. Susceptibility to infection is compounded by relative immunological immaturity and the incidence of infection is inversely related to gestational age and birth weight (BW).12 While the definition of early-onset sepsis (EOS) used in the literature varies from 2 to 7 days, we have shown that the great majority of early-onset infections occur in the first 48 hours after birth.6 7
The organisms most commonly causing early-onset neonatal infection in resource-rich countries are group B streptococcus (GBS) and Escherichia coli. Both organisms can also cause late-onset neonatal infection. There is strong evidence that the incidence of early-onset GBS (EOGBS) infection can be reduced using intrapartum maternal antibiotic prophylaxis.13 The mothers for whom chemoprophylaxis could be targeted can be identified by maternal screening for GBS carriage (screening-based approach) or by identifying maternal risk factors for early-onset infection (risk factor-based approach). The USA currently favours a screening-based approach to identify the maximum number of cases,14 but the downside is that more women receive intravenous antibiotics. In Australia and New Zealand, both risk and routine culture GBS screening are listed as acceptable by the Royal Australia and New Zealand College of Obstetricians and Gynaecologists.15 New Zealand neonatologists reported that the rate of EOGBS infection declined from 0.5 per 1000 live births in 1998–1999 to 0.23/1000 in 2009–2011 using a risk-based approach.11 In Australia, screening protocols vary from hospital to hospital. An Australasian study found that the EOGBS sepsis rate fell from 1.43/1000 live births in 1993 to 0.25/1000 in 2001, mainly attributed to increased use of intrapartum antibiotics.7
The current paper provides updated data on early-onset infections in neonatal units in Australia and New Zealand from 2002 to 2012.
Methods
We analysed retrospectively data on neonatal infections collected prospectively by Australia and New Zealand neonatal units participating in the Australasian Study Group for Neonatal Infections (ASGNI). The ASGNI commenced surveillance in 1991 in seven neonatal units, and by 1997 collected data from 14 Australian and two New Zealand units. It currently collects data from 11 Australian neonatal units and four units from New Zealand.6 7 The number of contributing units varied with time. The study has local and regional Ethics Committee approval.
The current study analyses data collected prospectively from 1 January 2002 to 31 December 2012 inclusive. Data collected include BW and gestational age, postnatal age at the time of onset of sepsis, the results of blood and/or cerebrospinal fluid (CSF) cultures, underlying diagnoses and outcome of infection (survival or death). The race of the subject was recorded (Maori, Aboriginal, neither Aboriginal nor Maori and unknown).
Neonatal infection was defined as the pure growth of at least one potentially pathogenic organism (bacterium or fungus) from the blood and/or CSF. If the organism cultured was a potential contaminant, we asked clinicians only to notify if the baby was clinically septic and had supportive laboratory evidence of sepsis (one or more of low or high white cell count or abnormal immature:total (I:T) white cell ratio, low platelets or raised serum C-reactive protein) according to predefined criteria.6–8 Clinicians were asked to decide if each episode met the criteria and asked not to report possible contaminants (eg, coagulase negative staphylococci, CONS) if there was no supportive clinical or laboratory evidence.6–8
Neonatal sepsis was defined to include all babies on the neonatal unit with sepsis regardless of postnatal age. EOS was defined as sepsis occurring in the first 48 hours after delivery. Meningitis was defined as a clinical presentation consistent with meningitis and either a positive culture of bacteria from CSF or a positive blood culture in association with an abnormal CSF white cell count (>100×106/L).6–8
The incidence rate of EOS was reported from neonatal units attached to maternity hospitals, and was calculated as the number of inborn EOS cases per 1000 liveborn babies. Outborn babies were excluded. Deaths were reported as being directly related to infection, possibly related to infection or unrelated to infection, but in the final analysis we included only those deaths directly related to sepsis. GBS colonisation status and use of intrapartum antibiotic prophylaxis were not recorded.
Data on the sensitivity of Gram-negative bacilli to cefotaxime and gentamicin were not collected in the initial stages of the study, but were requested in later years.
Statistical analysis was performed using SAS V.9.3. Poisson regression analysis was used to model the incidence rate over time. Associations between mortality, gestational age and BW were explored using Χ2 tests and logistic regression. We made no adjustment for multiple statistical comparisons.
Results
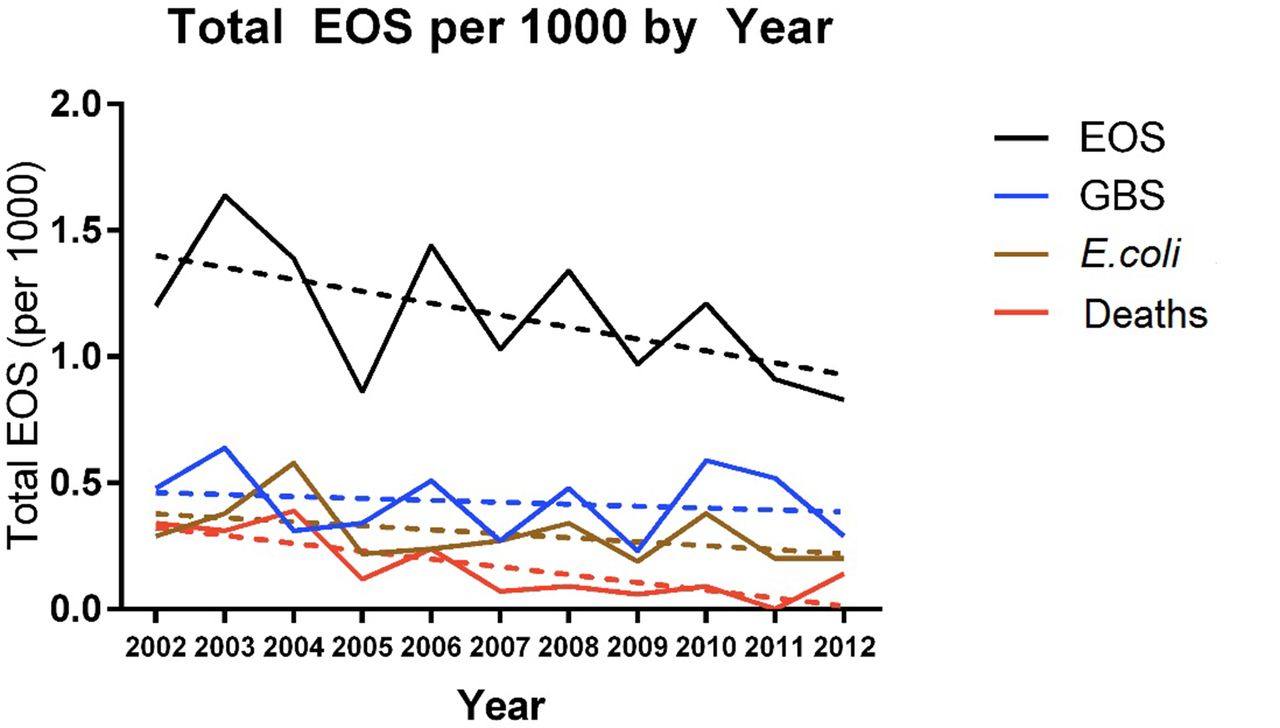
During the surveillance period (January 2002 to December 2012), a total of 386 423 babies were delivered in study hospitals. Of these, 321 201 were in Australia, representing 10.4% of the 3 079 088 babies born nationally,16 and 65 222 were in New Zealand or 9.8% of the 662 574 live births.17 Data on infants with sepsis were submitted from 15 centres: 454 babies had culture positive EOS (table 1). The overall incidence of EOS was 1.17 per 1000 live births. There was a decline in overall incidence of EOS from 1.20/1000 live births in 2002 to 0.83/1000 live births in 2012, decreasing by 3.9% per year (95% CI 1.1% to 6.7%, p=0.007), see figure 1. There were more male (57%) than female (43%) infants with early sepsis.
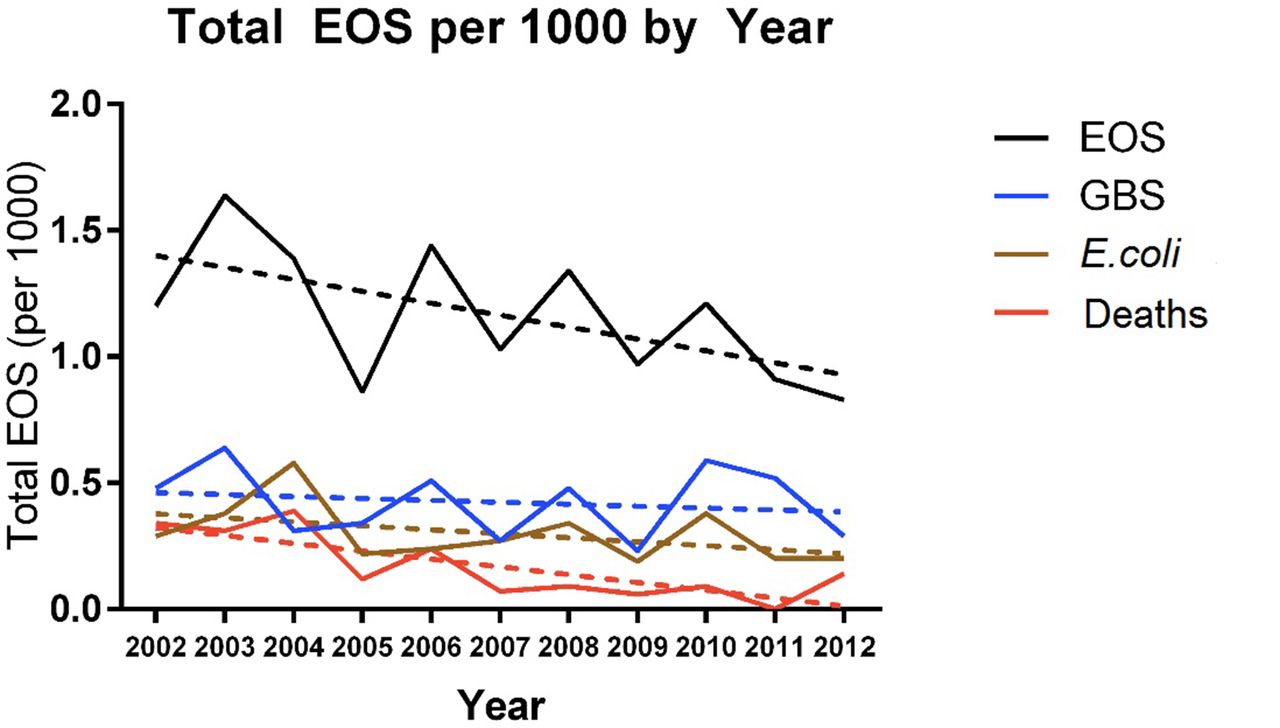
Incidence of early-onset sepsis (EOS) in Australasia, 2002–2012. Solid lines show observed rates per 1000 live births and dashed lines show predicted rates per 1000 live births from Poisson regression. GBS, group B streptococcus.
Demographics and outcome of early infections by birth weight and gestational age
Sixty-six (15%) of 454 infants died from EOS. There was strong evidence of decreasing incidence of death from early sepsis over time, from 0.34/1000 live births in 2002 to 0.14/1000 live births in 2012 (decreasing by 17% per year, 95% CI 9.9% to 24%, p<0.0001). Of the 454 babies, 47/161 (29%) with BW <1500 g died and 19/293 (6%) of those with BW ≥1500 g died. Overall, the mortality rate was highest in babies weighing <1000 g at birth and lowest among babies weighing >2 kg. The mean (SD) gestational age was 28 (5) weeks in neonates who died compared with 34 (6) weeks in neonates who survived or died from unrelated causes. The incidence of meningitis was 0.14/1000 live births.
Of the 454 cases of EOS, 290 (64%) were caused by Gram-positive organisms, 161 (35%) by Gram-negative organisms and the remaining cases by Candida sp (n=3). The most frequent EOS pathogen was GBS (37%), followed by E. coli (25%). The pattern of organisms was different for preterm (figure 2A) and term infants (figure 2B).
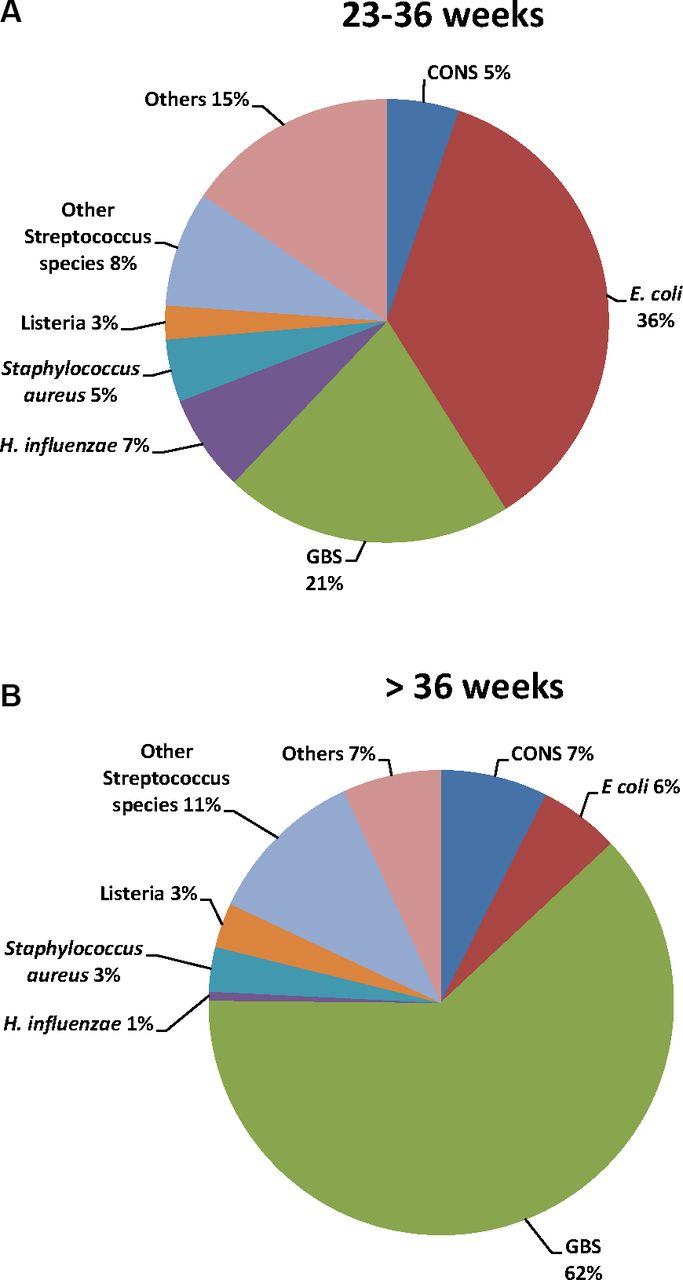
Organisms causing early-onset sepsis in infants born at gestation. (A) 23–36 weeks. (B) >36 weeks. CONS, coagulase negative staphylococci; GBS, group B streptococcus.
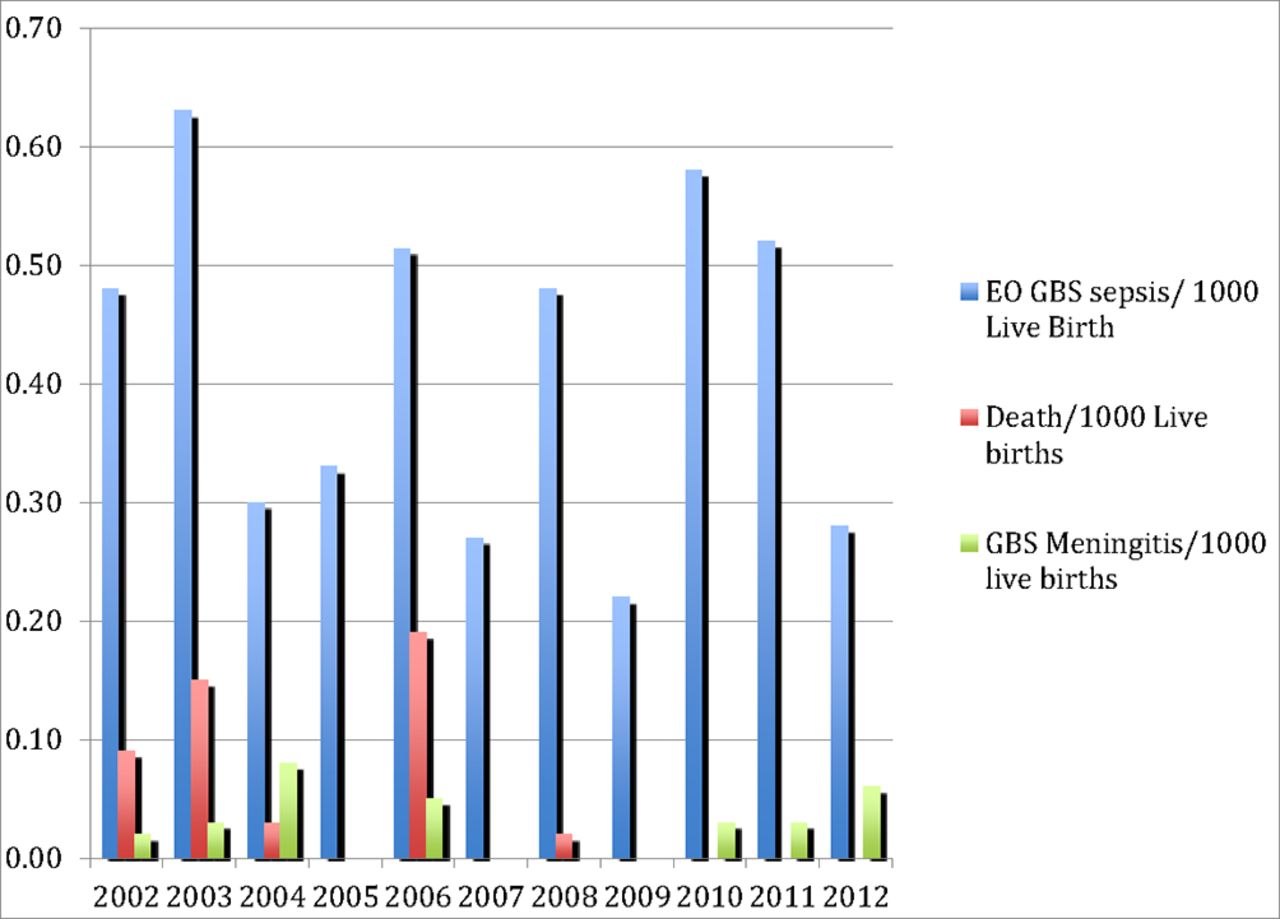
There were 166 cases of EOGBS sepsis, an incidence of 0.43 per 1000 live births, and 19 (11%) died (table 2). The incidence rate of EOGBS infection fluctuated from year to year, but there was no statistical evidence for any trend over time (decreasing by 2.4% per year, 95% CI −2.4% to 7.0%, p=0.32), see figure 3. The mean BW for EOGBS sepsis was 2815 g (SD 1169 g; range 585–5610 g). The mean (SD) gestational age was 36 weeks (5), range 23–41 weeks. Among infants with EOGBS sepsis, 62% were born at term (≥37 weeks) and 38% preterm. Seventeen (10%) of 166 infants with EOGBS had meningitis.
Organisms isolated from blood and/or cerebrospinal fluid of infants with early sepsis

Distribution of early-onset (EO) group B streptococcus (GBS) sepsis, meningitis and deaths, 2002–2012.
There were 114 cases of early-onset E. coli sepsis (figure 4), an incidence of 0.30 per 1000 live births. The incidence of E. coli sepsis did not vary significantly over time (decreasing by 4.5% per year, 95% CI −1.3% to 9.9%, p=0.12). Among neonates with early E. coli sepsis, 92% were born preterm (table 1). The mean (SD) gestational age was 30 (5) weeks, range 26–32 weeks. The mean BW was 1560 g (SD 866 g; range 515–4540 g). The case fatality rate from early E. coli sepsis was 25% (28 of 114). Nineteen (17%) of 114 infants with E. coli had meningitis. The mortality from early-onset E. coli infection was 35% for infants weighing <1500 g (22 of 63) at birth and 12% (6 of 51) for infants weighing ≥1500 g (p=0.005).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of early-onset Escherichia coli sepsis, meningitis and deaths, 2002–2012.
The mortality of early-onset E. coli sepsis was higher than for GBS (25% vs 11%, OR=2.5, 95% CI 1.3 to 4.8, p≤0.0001). However, when adjusted for gestational age and BW, this difference in mortality was not maintained (OR=1.2, 95% CI 0.6 to 2.5, p=0.6). The mortality was significantly greater for male (13.3%) than for female (2.6%) infants with GBS sepsis (p=0.001), but there was no gender difference for E. coli or for overall sepsis.
Nineteen babies with EOS were Aboriginal. This is 4.2% of the total EOS cohort of 454 babies, or 4.5% of the 424 babies where Aboriginal status was recorded. Of the 166 babies with EOGBS sepsis, 10 (6%) were Aboriginal. This is not statistically different from the rate of Aboriginal births in Australia: from 2002 to 2012 inclusive 158 166 (5.1%) of 3 079 088 births were recorded as being of Aboriginal and Torres Strait Islander parents (χ2=0.2, p>0.6).16
Sensitivities were reported on 42 (26%) of 166 Gram-negative bacilli. Of these, 41 (97.6%) were sensitive to both cefotaxime and gentamicin, and one organism was sensitive to gentamicin but resistant to cefotaxime.
Discussion
GBS is one of the most common organisms causing early-onset neonatal sepsis in Australasia and globally. A 2012 meta-analysis of 74 studies worldwide showed an overall incidence rate of EOGBS infection of 0.43 per 1000 live births (95% CI 0.37 to 0.49) and a case fatality of 12.3% (6.2%–18.3%).18 ASGNI has previously shown a steady decline in the incidence of EOGBS in Australasia from a peak of 1.43/1000 live births in 1993 to 0.25/1000 in 2001 with an overall rate of 0.67/1000 over 10 years.7 The highly significant fall in incidence was temporally and probably causally associated with increasing use of intrapartum antibiotic prophylaxis.7 Since then, a small Australian study showed an incidence of EOGBS sepsis of 0.38/1000 live births from 2005 to 2008.19 We found that the incidence of EOGBS sepsis from 2002 to 2012 was 0.43/1000 live births and, although it fluctuated from 0.23 to 0.64/1000, it did not vary significantly over time. These data are consistent with global18 and national figures,12 18 although the incidence could be reduced further if the government decided to introduce universal maternal GBS screening.15 18 20
The organisms causing EOS in our study are largely comparable to those in other Western countries.21–25 Some North American studies have reported CONS as an important cause of early sepsis,21 22 but we suspect many reported cases were blood culture contaminants. Our strict definition of EOS, requiring both clinical and supportive laboratory evidence of infection as well as positive cultures, excluded many Australasian babies who had positive blood cultures with CONS. The spectrum of organisms we found causing early sepsis for term compared with preterm infants was covered well by the current empiric antibiotics for suspected early sepsis which was ampicillin or penicillin plus gentamicin in every centre. Furthermore, we found no gentamicin resistance in any of the 42 recent Gram-negative bacilli tested, although we acknowledge this was less than a quarter of all such isolates. This contrasts with many countries in Asia26–29 and Africa30 where Gram-negative bacilli are often multiresistant.
We found a fall in incidence of all early-onset infections, but were unable to identify reduction of incidence of a single organism to explain the fall. The most likely explanation is a fall in incidence of GBS and other penicillin-sensitive organisms which when combined reaches statistical significance. Intrapartum antibiotic prophylaxis to prevent GBS may reduce the incidence of early-onset infection with other penicillin or ampicillin-sensitive organisms, as we described previously.7 However, we do not have data on compliance with intrapartum prophylaxis to support our hypothesis.
In our cohort, 14.5% of the neonates with EOS died compared with 16% in a recent large North American study.22 However, selection of the populations studied was different and mortality increases with decreasing gestational age,13 24 which is important to consider when comparing mortality data. In our study, the mortality from EOS decreased over time, presumably due to better technology and improved care, and this difference in mortality was highly statistically significant. Mortality was highest in extremely low birthweight infants <1000 g, as in other countries.2–4
Comparable to other industrialised countries, 62% of infants with EOGBS sepsis were born at term,7 12 14 23 24 but only 8% of infants with early-onset E. coli sepsis. The mortality from early-onset E. coli sepsis (25%) was significantly higher than for GBS (11%), but the difference in mortality was no longer significant after adjusting for gestation. The often reported higher mortality of early-onset E. coli infection compared with GBS, sometimes attributed to a difference in organism virulence, may be due to differences in gestation.
ASGNI has shown previously that Aboriginal infants have a higher rate of early-onset neonatal infection than non-Aboriginal infants.6 7 From 1991–1993, the incidence of EOGBS infection in Aboriginal infants was 5.2 per 1000 live births compared with 2.0 in non-Aboriginal Australians and from 1991 to 1997, the OR for Aboriginal babies developing EOGBS compared with non-Aboriginal babies was 4.3 (95% CI 2.9 to 6.2).7 Encouragingly, in the current study the rate of GBS infection was no higher in Aboriginal than non-Aboriginal infants. This finding should be interpreted with caution: it is based on small numbers and only refers to Aboriginal children born in an urban setting, a small proportion of all Aboriginal births, which are more often rural. Nevertheless, ‘closing the gap’ between the health of Aboriginal and non-Aboriginal Australians is an aspiration which is being achieved slowly at best, so our data are grounds for cautious optimism.
Our study has a number of limitations. We collected data on only 10% of all live births in Australia and New Zealand, and only from centres in major cities. We do not know if these data are representative of what happens in smaller urban and rural centres. Nevertheless, because we have collected data using the same methods since 1991, we are able to compare trends with modest confidence that the data reflect meaningful changes. We defined EOS as infection occurring within 48 hours of birth. We have shown before that including infections occurring in the first 7 days adds very few infections with organisms such as GBS and E. coli, but increases the number of infections with CONS and other organisms more likely to have been acquired nosocomially.6 7 We have not presented data on infections occurring from 3 to 7 days, which we will report elsewhere, but including these would not materially alter our conclusions. We used a rigorous but debatable definition for sepsis which required clinicians to decide whether or not to report infections with positive blood or CSF cultures and, where possible contaminants were concerned, needing both clinical and laboratory evidence in support. We believe that less rigorous definitions result in data which are more likely to include contaminants and hence less robust.
In conclusion, the continuing relatively low rate of EOGBS infection is encouraging, although it is sufficiently high to exclude complacency. Other studies will be needed to examine optimal intrapartum antibiotic use. Other encouraging features were an apparent closing of the gap between the rates in Aboriginal and non-Aboriginal infants and the absence of resistant Gram-negative bacilli.
References
Footnotes
Contributors TS analysed the collected data and wrote the manuscript. EHB did all the statistical analyses and reviewed and helped finalise the manuscript. DI conceived the study, collected all the data, and reviewed and helped finalise the manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval Royal Alexandra Hospital Ethics Board and regional ethics boards.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The database containing deidentified neonatal data on infections and antibiotic use is available on request to bona fide researchers.
Collaborators The Australasian Study Group for Neonatal Infections consists of: C Barfield (Monash Medical Centre, Melbourne Australia); D Bourchier (Waikato, New Zealand); G Bury, P Dargaville (Hobart Hospital, Tasmania, Australia); D Cartwright (Royal Women’s Hospital, Brisbane, Australia); A Daley, P McDougall, J Royle (The Royal Children’s Hospital, Melbourne, Australia); B Darlow (Christchurch, New Zealand); S Fraser, J Holberton (Mercy Hospital, Melbourne, Australia); L Gilbert, MD FRACP FRCPA (Westmead Hospital, Sydney, Australia); K Grimwood, MD FRACP (Wellington, New Zealand); The late D Henderson-Smart, H Jeffery (King George V Hospital, Sydney, Australia); R Halliday, D Isaacs (The Children’s Hospital at Westmead, Sydney, Australia); R Kohan (King Edward Memorial Hospital, Perth, Australia); A McPhee (Women’s and Children’s Hospital, Adelaide, Australia); R Messer (Cairns Base Hospital, Cairns, Australia); D Tudehope, D Knight (Mater Hospital, Brisbane, Australia).