Article Text

Abstract
Aims Numerous studies have identified shortcomings in the management of children at risk of severe acute allergic reactions (anaphylaxis). The Science and Research Department at the Royal College of Paediatrics and Child Health (RCPCH) was commissioned by the Department of Health to develop competence based national care pathways for children with allergies. Anaphylaxis is the first completed pathway.
Methods The anaphylaxis pathway was developed by a multidisciplinary working group, reviewed by a broad group of stakeholders and approved by the Allergy Care Pathways Project Board and the RCPCH Clinical Standards Committee.
Results Pathway development is described under five headings: evidence review, mapping, external review, core knowledge documents and key recommendations. The full pathway can be downloaded from www.rcpch.ac.uk/allergy/anaphylaxis. This document describes the entry points and the ideal pathway of care from self-care through to follow-up. The five key recommendations focus on: (1) prompt administration of adrenaline by intramuscular injection; (2) referral to specialists with competence in paediatric allergies; (3) risk analysis; (4) provision of a self-management plan; and (5) suggested creation of a national anaphylaxis death register.
Conclusions We present the first national care pathway for anaphylaxis, which is based on a critique of published evidence, expert consensus and multi-stakeholder input including patient representation via the Anaphylaxis Campaign. The Project Board urges health professionals to work together across networks to improve care for children at risk of anaphylaxis, in particular during the period after an acute reaction. Additionally, the Project Board strongly recommends the funding of a national anaphylaxis register.
Statistics from Altmetric.com
Introduction
The community need for and purpose of care pathways for children with allergies is described elsewhere. We here present the first pathway for children at risk of anaphylaxis.
Anaphylaxis is a severe, life-threatening and systemic hypersensitivity reaction characterised by rapidly developing life-threatening respiratory and/or circulation problems; it is usually associated with skin and mucosal changes.1 2 The incidence rate is estimated to be between 80 and 210 episodes per million person-years3 and varies by age, gender, geography and socio-economic position.4 Time trend data suggest that the incidence of anaphylaxis has increased over recent decades and this appears in particular to be due to real increases in allergies to foods in infants, children and young people; however, greater awareness, recognition, reporting and recording are other possible explanations.4,–,10
The most common trigger for anaphylaxis in childhood is food, followed by drug allergy. Anaphylaxis due to other triggers such as insect venom or exercise is rare6 11; it may also occur spontaneously (idiopathic). The most frequent food triggers in childhood are peanut and tree nuts, cow's milk, hen's egg, fish and shellfish.12 13 The overall case fatality ratio is estimated to be less than 1% in the majority of case series, or in population terms between 1 and 5.5 fatal episodes of anaphylaxis per million population per year.3
As a potentially fatal condition, anaphylaxis can have a profound impact on quality of life, and this may extend way beyond the acute phase of the illness.14 Although still often thought of mainly as an acute disorder, anaphylaxis should really be considered a long-term condition.15 The impact on quality of life of affected families should not be under-estimated. The quality of care for such families by medical professionals is variable at present, and there is a correspondingly low level of knowledge of anaphylaxis and its management.16
Children at risk of anaphylaxis require a comprehensive care package comprising correct identification of the trigger, avoidance advice, provision of and training in the use of emergency medication, and training of school personnel and all other carers.17 In this pathway, we aim to describe an optimal standard of care, achievable by health professionals trained to an appropriate degree of competency. We do not distinguish between different levels of care (eg, secondary or tertiary allergy clinic) when recommending who caries out each task, but instead describe the minimum competences required to effectively deliver each section of the pathway.
Methods
The full methodology is described separately in this supplement.18
Results
The results of the pathway development are presented under five headings: evidence review, mapping, external review, core knowledge documents and key recommendations. The full pathway can be downloaded from http://www.rcpch.ac.uk/allergy/anaphylaxis.
Evidence review
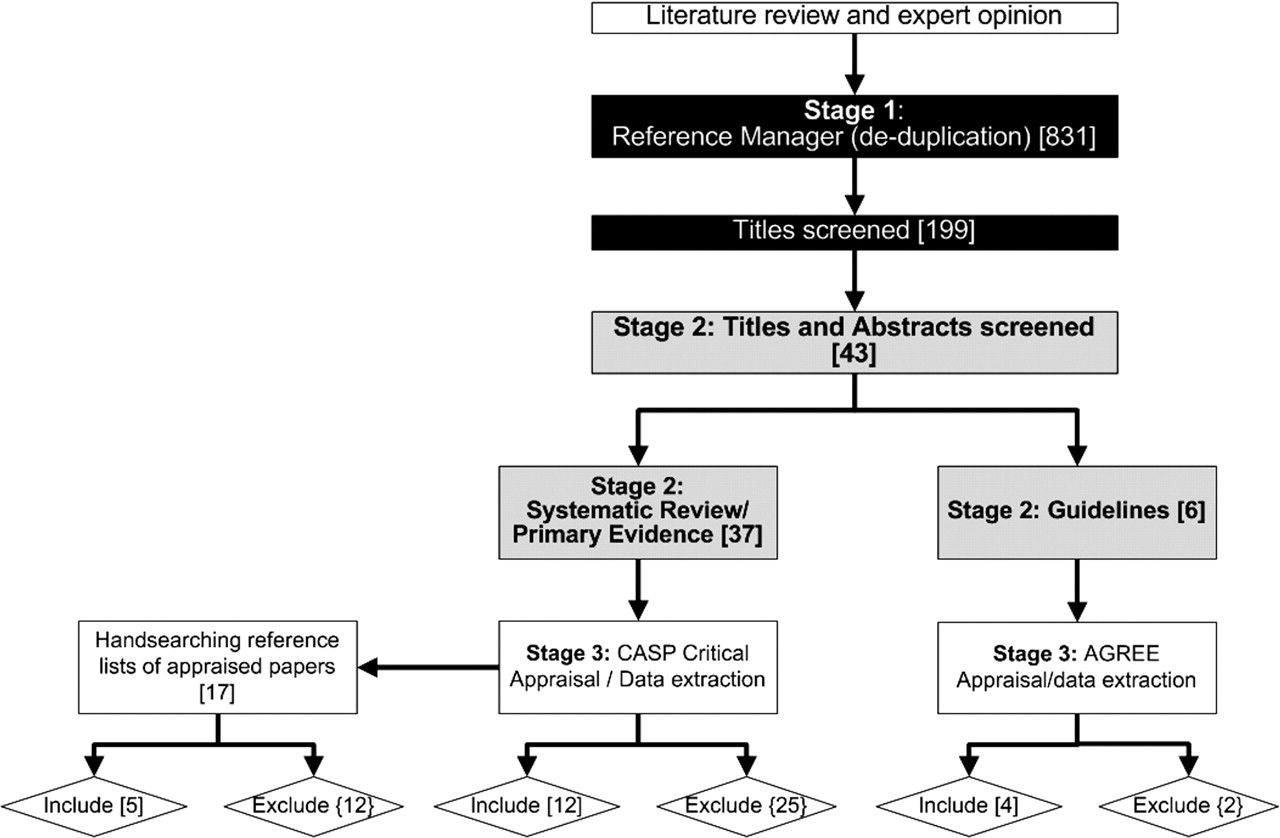
A total of 831 titles and abstracts were screened by the Project Manager and the Anaphylaxis Working Group (AWG) Chair (figure 1). Thirty-seven systematic reviews and/or primary papers and seven guidelines were identified for appraisal; hand-searching the reference lists of appraised papers identified a further 17 papers. The critical appraisal resulted in the inclusion of 17 systematic reviews and/or primary papers and five clinical practice guidelines.
{kind=link}
Anaphylaxis care pathway: methodology of evidence review.
The evidence review did not identify any randomised controlled trials to support the diagnosis and/or management of anaphylaxis. Most of the appraised evidence was methodologically weak (eg, case series, observational studies); in particular, methodologies in published documents were often unclear. Authors were contacted for additional information in some instances, but the methodology remained substandard in all cases. The evidence review also found that while the use of adrenaline (epinephrine) injectors is the frontline treatment for anaphylaxis,19,–,23 the injectors are often underused, if at all, by patients and their families.16 24 25 Understanding information needs26 and providing good education to patients, their families and schools was highlighted as a key way to improve management.21 27 While the nomenclature varied, there was evidence that the use of written management plans improved outcomes.17 28,–,31 The clinical guidance clearly showed the value of mast cell tryptase measurement in diagnosis21 and the use of skin prick tests and food challenges for confirming food allergies22 32,–,34 and conducting a risk assessment.35 The value of good history taking22 and referral to a specialist allergy clinic was also highlighted in the research.17 21 36 A full evidence table can be obtained from http://www.rcpch.ac.uk/allergy.
Mapping
The national care pathway for anaphyalxis can be downloaded at www.rcpch.ac.uk/allergy/anaphylaxis. This pathway was developed around the competences required to diagnose and optimally manage anaphylaxis.
There is no universally agreed definition for anaphylaxis. For the purposes of this pathway, the AWG has modified agreed UK21 and European definitions2 and defined anaphylaxis as a severe, life-threatening, generalised or systemic hypersensitivity reaction which is likely when both of the following criteria are met:
Sudden onset and rapid progression of symptoms
Life-threatening airway and/or breathing and/or circulation problems.
Skin and/or mucosal changes (flushing, urticaria, angio-oedema) can also occur, but are absent in a significant proportion of cases.
The competences required underpinning the various elements are described in appendix 1. These competences have not been assigned to specific health professionals or settings in order to encourage flexibility in service delivery. However, it is envisaged that the provision of optimal care at all levels will require close liaison between different health professional groups including doctors, nurses and dieticians. All specialists should have paediatric training in line with the principles outlined in the Children's National Service Framework.37
For the purposes of the pathway, ‘children’ is an inclusive term that refers to infants, children and young people (0–18 years). A specialist allergy clinic is defined by the competences laid out in this document.
While the pathway is linear, it is important to recognise the entry points can occur anywhere along the pathway and that the pathway children follow may not be linear.
External review
A total of 26 out of 36 (72%) invited organisations responded, providing 187 comments.
Core knowledge documents
The working group identified three key guidelines (core knowledge documents) that support the clinical knowledge required to deliver this pathway. They are:
▶ The Resuscitation Council UK (Resus UK) guideline on the emergency medical treatment of anaphylactic reactions21
▶ The European Academy of Allergy and Clinical Immunology guideline on the management of anaphylaxis in childhood35
▶ The Guidelines in Emergency Medicine Network guideline for the management of acute allergic reaction.23
Key recommendations
The AWG acknowledges that pathways do not normally contain key recommendations but the AWG felt it was necessary to make five key recommendations regarding the treatment and management of children with anaphylaxis (box 1).
Box 1 Recommendations
Prompt administration of adrenaline by intramuscular injection is the cornerstone of therapy in both the hospital and the community.
Infants, children and young people at risk of anaphylaxis should be referred to clinics with specialist competence in paediatric allergies.
Risk analysis should be performed for all patients with suspected anaphylaxis.
Provision of a self-management plan may reduce the frequency and severity of further reactions and is a recommended part of anaphylaxis management.
All deaths from suspected anaphylaxis should be recorded on a register, ideally a national anaphylaxis death register.
Discussion
The goals of this project are described elsewhere. The formal searching and critiquing of the literature is a real strength in developing this care pathway and to our knowledge this is the first time that this has been undertaken in relation to allergy care. While the quality of evidence identified was weak, this was to an extent mitigated by the involvement of a multidisciplinary team to develop the pathway. However, there are clinical data to show the effectiveness of allergen avoidance and management plans, but more is needed. In response to the paucity of data, the AWG has developed some research recommendations; these are currently the subject of a Delphi consensus and will be published on the RCPCH website in the final report.
Additionally, the Project Board strongly supports the funding of a national anaphylaxis death register. Each local area would be responsible for registering deaths in a local register and should funding be obtained, these registers could be fed into a national register. The cause of the fatal reaction should be established through analysis of post-mortem blood samples and gastric washings. The former should be assayed for tryptase and food allergens and the latter for common allergenic proteins. Additional information on circumstances could be gathered later from relatives. This strategy has been very effective elsewhere in improving understanding.20 38 39 A register has previously been supported by the Office for National Statistics, the Home Office, the Food Standards Agency and the Anaphylaxis Campaign but is currently unfunded and urgently requires ongoing financial support. A national register would be an important step forward in identifying the cause of unnecessary and avoidable deaths from anaphylaxis.
Acknowledgments
We thank Dr Adam Fox, Dr Gillian Vance and Ms Linda Haines who were all present at the initial Anaphylaxis Working Group meeting; Ms Hilary Whitworth, a PhD student at the University of Southampton, who provided assistance for the evidence review; the RCPCH Allergy Care Pathways Project Board who provided guidance and assistance; and the RCPCH Clinical Standards team for their hard work on the approval process, in particular Ms Katie Jones.
References
Footnotes
-
Funding This project was funded by the Department of Health.
-
Competing interests AC has carried out consultancy work for Schering Plough. ME is employed by Anaphylaxis UK. AS is involved in ongoing work funded by the government and charitable donors in relation to allergic disorders which include anaphylaxis, and has carried out consultancy work for Phadia, ALK and Schering Plough. JW has carried out consultancy work for Novartis, Danone, Airsonette, Merck, Allergy Therapeutics, Phadia Research, GSK, AstraZeneca, Merck, Allergy Therapeutics and ALK.
-
Copyright licence statement The pathways and associated competences remain the copyright of the Royal College of Paediatrics and Child Health.
-
Provenance and peer review Not commissioned; not externally peer reviewed.