Article Text

Abstract
Introduction: Several autopsy protocols have been suggested for investigating sudden unexpected deaths in infancy (SUDI). The aim of this study is to provide data on the utility of such post-mortem investigations from a large paediatric autopsy series to inform future policy.
Methods: Retrospective analysis of >1500 consecutive post-mortem examinations carried out by specialist paediatric pathologists at a single centre during a 10-year period according to a common autopsy protocol that included the use of detailed ancillary investigations. SUDI was defined as the sudden unexpected death of an infant aged from 7 to 365 days. All data capture and cause of death classification were carried out according to defined criteria.
Results: Of 1516 paediatric post-mortem examinations, 546 presented as SUDI. In 202 infants (37%), death was explained by the autopsy findings. The other 344 cases (63%) remained unexplained. Of the explained deaths, over half (58%) were infective, most commonly due to pneumonia (22%). The component of the post-mortem examination that primarily determined the final cause of death was histological examination in 92 infants (46%), macroscopic examination in 61 (30%), microbiological investigations in 38 (19%) and clinical history in 10 (5%).
Conclusion: This constitutes the largest single-institution autopsy study of SUDI. Ten years on from the Confidential Enquiry into Stillbirths and Deaths in Infancy (CESDI) SUDI studies, the ascertainment of a cause of death at autopsy has improved. However, with almost two thirds of SUDI remaining unexplained, alternative and/or additional diagnostic techniques are required to improve detection rates of identifiable causes of death at autopsy.
Statistics from Altmetric.com
Sudden unexpected death in infancy, defined as the sudden and unexpected death of an infant aged less than 1 year, constitutes the most common cause of post-neonatal death in the first year of life.1 In 2005, there were 268 unexplained infant deaths in England and Wales, an incidence of 0ṡ41 deaths per 1000 live births.2 SUDI comprises a heterogeneous group, including deaths in which a careful review of the death scene and a meticulous post-mortem examination will disclose a cause of death, and those which will remain unexplained even after such examination, including a review of the circumstances of death and a detailed autopsy with various ancillary investigations.3 In these latter cases, the death may be classified as sudden infant death syndrome (SIDS or “cot-death”) if the infant died during sleep.4 In England and Wales, all SUDI cases are investigated on behalf of Her Majesty’s Coroner (HMC), which includes the carrying out of a post-mortem examination by a designated pathologist. Several autopsy protocols for this indication have been suggested, all of which include a range of ancillary investigations. Currently, in the United Kingdom, it is suggested that such autopsies are performed by specialist paediatric pathologists according to a protocol set up by an expert panel.5 However, such guidelines are primarily based on expert opinion rather than directly derived from published evidence.
The largest previous study based in the United Kingdom reviewing post-mortem investigations of SUDI was conducted more than 10 years ago and formed part of a larger study that was primarily designed to collect epidemiological data relating to deaths in this age group.3 The study, which became known as the Confidential Enquiry into Stillbirths and Deaths in Infancy (CESDI) SUDI studies, included post-mortem pathological findings from many different centres; the majority of autopsies had not been carried out by paediatric pathologists, and many of the post-mortem examinations lacked important ancillary investigations. The aim of the present study is to provide current data on the post-mortem investigations of SUDI from a large series of paediatric post-mortem examinations, all performed during a 10-year period by paediatric pathologists at a single specialist centre according to a common protocol to determine the proportion of cases for which a definite cause of death can be identified using such protocols, and to provide data regarding the relative roles of the various ancillary investigations in determining the cause of death in order to inform future policy.
METHODS
Great Ormond Street Hospital for Children, London, United Kingdom, is a specialist tertiary referral centre for the investigation and treatment of a range of paediatric disorders. The Department of Pathology undertakes post-mortem examinations of paediatric deaths on behalf of HMC from London and the surrounding areas. In addition, forensic paediatric autopsies, in which there is the possibility of an associated criminal act, are also performed at the centre via HMC and the police. As part of a large retrospective analysis of >1500 consecutively performed post-mortem examinations over a 10-year period (1996 to 2005 inclusive), a comprehensive review of all SUDI autopsies was carried out. For the purposes of this study, SUDI was defined as the death of an infant aged from 7 to 365 days that was sudden and unexpected. The entire database, including all post-mortem examinations performed during the study period, was searched to identify cases in which the indication for autopsy was SUDI. The records of each case were reviewed and data recorded in a specially designed, secure database in which cases were identified by study number only. The study was approved by the local research ethics committee (LREC).
All post-mortem examinations were performed by specialist paediatric pathologists at a single centre. In all cases, clinical information regarding the circumstances of death was provided by HMC or the investigating police. A local autopsy protocol was followed that included the use of detailed ancillary investigations, which was modified slightly during the 10-year period, and comprised a full macroscopic post-mortem examination in addition to post-mortem radiology, histological examination, bacteriological and virological investigations, and metabolic studies, as well as other analyses, such as biochemical or toxicological investigations, in selected cases. To ensure consistency for data analysis and interpretation, all data extraction, data entry and data classification was carried out by a single paediatric pathologist according to clearly defined criteria (available on request). In particular, for the purposes of this classification, diagnosis of “septicaemia” was based on the identification of pathogenic organisms known to be associated with septicaemia in the absence of an identifiable focus of infection during life, from blood, CSF or spleen culture samples, and following discussion of all cases with a paediatric microbiologist with experience in the interpretation of such autopsy samples. For each case, the basic demographic features, autopsy findings, results of all ancillary investigations and final cause of death were recorded and reviewed. Cases were classified into those with identifiable causes of death (the “explained SUDI” group) and those in whom a definite cause of death could not be found (the “unexplained SUDI” group). Statistical methods used included the comparison of proportion and χ2 tests for gender and season, respectively, and differences in distributions between groups were analysed using the Mann–Whitney U test.
RESULTS
During the 10-year study period, a total of 1516 paediatric post-mortem examinations were performed in the centre, including 546 autopsies of infants aged from 7 to 365 days presenting as SUDI. Of these, 98% (537 autopsies) were carried out by one of five paediatric pathologists and more than two thirds of autopsies were performed by one of two pathologists. In 202 infants (37%), an identifiable cause of death was diagnosed following a detailed post-mortem examination (the “explained SUDI” group). In the other 344 cases (63%), the cause of death remained unexplained despite extensive post-mortem investigations (the “unexplained SUDI” group). The majority of the unexplained deaths (81%) were recorded to have occurred during sleep, thus satisfying the criteria for sudden infant death syndrome (SIDS); importantly, however, the unexplained SUDI group also incorporates a small number of unexplained deaths that would be best classified as “undetermined”, including such deaths that were associated with non-lethal injuries suspicious of non-accidental injury but in which these injuries did not directly contribute to the death of the infant.
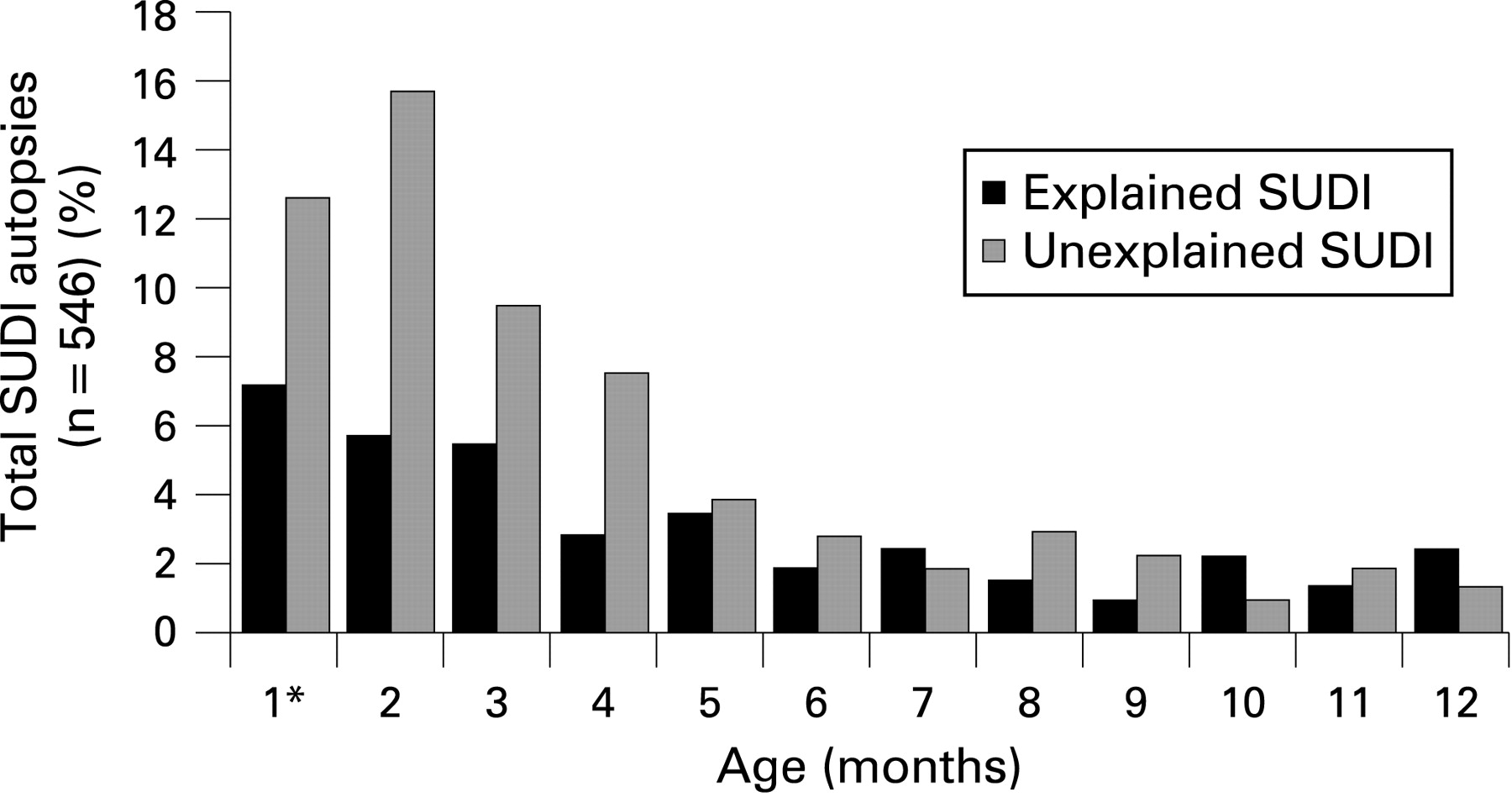
Most deaths occurred in the first three months of life (median age 76 days, interquartile range 38 to 161 days, fig 1), but the explained SUDI group (median age 92.5 days) was significantly older than the unexplained SUDI group (median age 66 days, Mann–Whitney U test p = 0.004). There was no significant seasonal variation ( χ2 0.87, p = 0.8), but overall there were more boys (56%) than girls (44%, p = 0.0002, proportion difference 11.4%, 95% CI 5.4% to 17.2%).
Of the 344 unexplained deaths, 11 (3%) showed no abnormal findings at autopsy at all, while in the majority (240 cases, 70%) the autopsy revealed minor non-specific abnormalities, such as petechiae of the lungs, heart and/or thymus, pulmonary congestion or varying degrees of intra-alveolar haemorrhage, but these pathological findings were insufficient to explain or significantly contribute to death. In the remaining 93 cases (27%), pathological changes were detected at autopsy that at most may have contributed to death, but that were not sufficiently severe to have caused death; these included cases with evidence of aspiration without an associated inflammatory reaction in the lungs and thus likely to represent an agonal event, cases with mild bronchiolitis, cases with culture-negative small adrenal haemorrhage and cases with evidence of hypoxic-ischaemic brain injury as a consequence of post-resuscitation survival following the initial collapse.
Of the 202 explained deaths, the majority (118 cases, 58%) were due to an infective process, most commonly pneumonia (44 cases, 22%), while the commoner non-infective causes of death included congenital malformations (14 cases, 7%) and deaths due to accidental (12 cases, 6%) and non-accidental injuries (20 cases, 10%; see table 1 and fig 2). Of the 118 infective deaths, the majority were due to bacterial infections (80%), with 21 deaths due to presumed viral infections and three deaths caused by Pneumocystis jirovecii (carinii) respiratory infections (fig 3). Not surprisingly, deaths due to unsuspected congenital abnormalities occurred at a significantly younger age (median age 15.5 days) than deaths due to infections (median age 95.5 days, Mann–Whitney U test p<0.0001).


In the explained SUDI group, the component of the examination that primarily determined the final cause of death was the macroscopic examination at autopsy in 61 cases (30% of explained SUDI, 11% of all 546 SUDI), the histological examination in 92 (46% of explained SUDI, 17% of all 546 SUDI), microbiological investigations, including culture and/or PCR, in 38 cases (19% of explained SUDI, 7% of all 546 SUDI) and the clinical history in 10 (5% of explained SUDI, 2% of all 546 SUDI). Toxicological analyses were performed in only selected cases and revealed the cause of death in only one infant, which was due to accidental heroin poisoning (fig 4). Radiology showed fractures in 34 cases, but, while these findings significantly contributed to the final diagnosis in many of these infants, the presence of fractures detected radiologically did not primarily determine the cause of death in these cases. Tandem mass spectrometry was performed on post-mortem blood and/or bile samples in 171 cases (31%), but in this series of infants aged 1 week to 1 year, no fatty acid oxidation defects were detected on acylcarnitine profiling.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
This is the largest single-institution autopsy study of SUDI in which all post-mortem examinations were performed by specialist paediatric pathologists according to a common protocol that included a range of different ancillary investigations. The findings of this study demonstrate that, firstly, even when all post-mortem examinations are performed by specialist paediatric pathologists, and despite following the currently suggested autopsy guidelines for SUDI,5 an identifiable specific cause of death can only be established in around one third of SUDI cases. Secondly, of the identifiable causes, the commonest demonstrable aetiological group is infection-related. Thirdly, of all components of the post-mortem investigation, routine histological sampling is the investigation that provides the greatest proportion of additional information to establish a cause of death.
The age distribution of the infant deaths in this study is similar to previously reported studies.6–8 Most studies have shown a peak frequency for SIDS between two and four months of age3 6; however, our data show a high proportion of unexplained deaths in the first month of life, which in this study excludes the first six days of life, one possible explanation for this being selection bias by HMC by preferentially referring younger infants to our centre for autopsy. In the present study, the median age for unexplained SUDI was significantly lower than that for explained SUDI, but for both explained and unexplained deaths, the majority of deaths occurred in the first four months of life, confirming that early infancy represents an intrinsically vulnerable time period in susceptible infants. There was no relationship between the frequency of SUDI and seasonality in the present study, which is in agreement with several previous reports,3 6 although it has previously been suggested that the incidence of SUDI is greater during the winter months.9 In keeping with other published data,1 there were more boys than girls in the present study in both the explained and unexplained SUDI groups. Of particular interest, however, is the comparison of proportions of explained SUDI between the present study and the CESDI study3; in the latter, a cause of death was found on review in 80 of the 450 SUDI from across multiple centres between 1993 and 1996 (18%), which is significantly less than our study, in which a cause of death was determined in 37% (comparison of proportion test, p<0.0001, proportion difference 19.2%, 95% CI 13.8% to 24.5%). While some of these differences could potentially be explained by different diagnostic thresholds in assigning a cause of death to a pathological process between the two studies, we believe that this difference is more likely explained by the wider pathologists’ experience and changes in the ancillary investigative protocol in the present study, in which all post-mortems were performed by a small number of specialist paediatric pathologists, all of whom used a common protocol that included the consistent use of a range of specialist investigations. In contrast to our study, a recent German multicentre study6 reported an identifiable cause of death in only 11% of 455 SUDI; although that study excluded deaths due to inflicted injuries, the reason for the relatively low ascertainment of a cause of death remains unclear and may again be related to use of multiple and/or non-paediatric centres. However, perhaps more importantly, despite following current autopsy guidelines for the investigation of SUDI5 in the present study, almost two thirds of SUDI remained unexplained, suggesting that we have reached a plateau in the proportion of explainable cases of SUDI using current post-mortem investigative protocols, and that, to further improve the detection rate of identifiable causes, alternative or additional diagnostic techniques are required.
Histological examination remains the single most useful investigation in the determination of the cause of death in SUDI, allowing a cause of death to be identified in 46% of the explained SUDI group, which is in keeping with the findings of the CESDI study.3 A recent study found that review of the circumstances of death (42%), followed by macroscopic and histological examination (44% and 40%, respectively) were the three most important post-mortem investigations for the detection of identifiable causes of death, and that in two thirds of cases, more than two investigative components are required at autopsy to determine the cause of death.8 Furthermore, in the present study, the majority of infection-related diagnoses were identified primarily by histological sampling rather than microbiological analyses, although the latter accounted for almost 20% of diagnoses that would otherwise have been missed had routine microbiological sampling not been performed. However, there are several investigations suggested in the current autopsy protocol5 that appear less useful as a routine screening tool for determining the cause of death in unselected cases. In particular, although routine oil-red-O staining of composite frozen sections of cardiac and skeletal muscle, liver and kidney was carried out, together with tandem mass spectrometry of blood and/or bile in selected cases, there were no deaths due to fatty acid oxidation disorders in this series of SUDI aged from 1 week to 1 year, although previous studies have reported such metabolic diseases as causes of death in this patient group. Combining the data from the current and previous studies (table 2), there are six reported deaths due to metabolic disorders from a total of 2054 cases presenting as SUDI, representing 0.3% (95% CI 0.1% to 0.6%) of SUDI cases. In such cases, it is expected that there would be abnormal fat accumulation in liver, renal tubules and muscle, and hence histological screening with retention of additional samples may be a more cost efficient protocol for the identification of such rare cases rather than routine tandem mass spectrometric analysis and/or routine fibroblast culture assays.
In the present series, infection was the commonest aetiological group for the cause of death in the explained SUDI group and this supports the concept that a significant number of currently unexplained SUDI deaths may be infection related, either in the form of infection with organisms undetectable using standard methodologies or as a consequence of abnormal systemic or local immune responses in association with otherwise subclinical infections.9 11 Post-mortem microbiology is carried out in all SUDI cases but its interpretation in the post-mortem setting may be problematic and at present is based on empirical guidelines, which may, at least in part, explain the observed differences in the prevalence of infective deaths in other SUDI studies (table 2); other possible explanations for these variations include sampling issues and subjective interpretation of histological findings. Further studies may allow identification of the abnormal host immune response in such cases rather than attempting to isolate the organism(s) responsible for the exaggerated response.
In conclusion, 10 years on from the CESDI study, the ascertainment of a cause of death in SUDI appears to have improved significantly owing to such post-mortems being performed in specialist centres by paediatric pathologists with the consistent use of a range of ancillary investigations. These data support the recommendation that SUDI autopsies be conducted by appropriately trained (paediatric) pathologists in centres that have a specialist interest and expertise in the investigation of such deaths. The precise mechanisms by which this is achieved will vary according to national structures and guidelines, but the continued establishment and development of such specialist services across managed pathology networks is both consistent with current trends in the provision of pathology services in the UK and supports the development of common investigative protocols. This approach would also facilitate future analysis of pooled data from multiple centres, which may further improve our understanding of underlying pathophysiological mechanisms of these infant deaths. Currently, despite using recommended United Kingdom autopsy guidelines,5 which are similar to those advocated in the internationally recommended post-mortem protocol for the investigation of SIDS,12 almost two thirds of SUDI deaths remain unexplained, clearly highlighting the need for identifying alternative and/or additional diagnostic techniques to further improve the detection rate of identifiable causes of death at autopsy. These methods may include approaches such as immunohistochemical assessment and tissue-specific gene expression studies for markers of the inflammatory response to infection or detection of bacterial superantigens in tissues. With a paucity of published evidence on the utility of such investigations at post-mortem, there is clearly an urgent need for further focused research to assess the application of such novel post-mortem techniques in this context.
What is already known on this topic
-
Infection represents the commonest cause of explained SUDI.
-
Histological examination is an important component of the post-mortem examination to establish a cause of death in SUDI.
What this study adds
-
Ascertainment of a cause of death at autopsy is significantly improved if SUDI post-mortem examinations are performed according to the currently recommended autopsy protocol by paediatric pathologists using a range of ancillary investigations.
-
However, almost two thirds of SUDI will presently remain unexplained even if current autopsy guidelines are followed, highlighting the need for identifying alternative diagnostic techniques to further improve the detection rate of identifiable causes of SUDI at autopsy.
-
Histological examination remains the single most useful investigation in the determination of the cause of death in SUDI, revealing the cause of death in almost 20% of all SUDI that would otherwise be missed if histological sampling is not routinely performed.
Acknowledgments
This study was supported by a grant from The Foundation for the Study of Infant Deaths (FSID).
REFERENCES
Footnotes
-
Competing interests: None declared.
-
Ethics approval: The study was approved by the local research ethics committee (LREC).