Article Text

Abstract
Aims: To study bed-sharing and cot-sleeping infants in the natural setting of their own home in order to identify differences in the thermal characteristics of the two sleep situations and their potential hazards.
Methods: Forty routine bed-sharing infants and 40 routine cot-sleeping infants aged 5–27 weeks were individually matched between groups for age and season. Overnight video and physiological data of bed-share infants and cot-sleeping infants were recorded in the infants’ own homes including rectal, shin, and ambient temperature.
Results: The mean rectal temperature two hours after sleep onset for bed-share infants was 36.79°C and for cot-sleeping infants, 36.75°C (difference 0.05°C, 95% CI −0.03 to 0.14). The rate of change thereafter was higher in the bed-share group than in the cot group (0.04°C v 0.03°C/h, difference 0.01, 0.00 to 0.02). Bed-share infants had a higher shin temperature at two hours (35.43 v 34.60°C, difference 0.83, 0.18 to 1.49) and a higher rate of change (0.04 v −0.10°C/h, difference 0.13, 0.08 to 0.19). Bed-sharing infants had more bedding. Face covering events were more common and bed-share infants woke and fed more frequently than cot infants (mean wake times/night: 4.6 v 2.5).
Conclusions: Bed-share infants experience warmer thermal conditions than those of cot-sleeping infants, but are able to maintain adequate thermoregulation to maintain a normal core temperature.
- bed-sharing
- co-sleeping
- SIDS
- thermoregulation
Statistics from Altmetric.com
Bed-sharing, the norm in many cultures, is becoming more common in Caucasian societies.1–3 Benefits include ease of breast feeding, reduced tiredness, having a more settled baby,4–7 increased breast feeding, and increased mother-baby interactions and arousals.8,9,10,11
Bed-sharing, though not a risk factor in itself, is reported to interact to increase the risk of SIDS with many factors, including: maternal smoking,12–17 alcohol or illicit drug consumption,13–17 maternal excessive weight,18 overtiredness, household overcrowding, excessive bedding,13 soft bedding,19 other bed-sharers,20 and younger infant age.13,17,18
The major postulated mechanisms regarding the risk associated with the combination of maternal smoking in pregnancy and bed-sharing include rebreathing, respiratory obstruction, and hyperthermia. Following in-utero exposure to cigarette smoke an infant may be less able to respond appropriately to any of these stresses.21–23
Hyperthermia due to excessive bedding and/or clothing and its possible contribution to SIDS has been widely studied.24–27 It has been suggested that death could result from central disruption of respiratory28 or arousal mechanisms associated with hyperthermia.29 It is unclear whether hyperthermia may pose a greater risk during bed-share sleep or not. Tuffnell and colleagues,30 in overnight home studies, found that bed-sharing infants had a significantly higher rectal temperature than infants sleeping alone. Sleep laboratory studies have not found this increase in rectal temperature (Sawczenko, personal communication),31 but an increase in peripheral, forehead, and within-bed temperatures32 and an increase in axillary temperature.33
The main aim of this study was to monitor infants sleeping with their parent(s) in their home to capture childcare practices in their natural physical environment and to identify the behavioural and physiological risks and/or benefits of bed-sharing compared to cot-sleeping. This paper reports on the thermal environment of these infants.
METHODS
Two groups of infants were studied: 40 bed-sharing infants and 40 cot-sleeping infants. Bed-sharing infants regularly slept in the parental bed for a minimum of five hours/night. Cot-sleeping infants regularly slept in a cot or bassinette in the parental bedroom at least five hours/night. Bed-sharing infants were recruited through postnatal organisations in Dunedin and through advertisements in local media. Cot-sleeping infants matched for age and season of study were recruited from the postnatal ward of the local maternity hospital. Infants were aged 0–6 months and were over 37 weeks gestation (except for two infants in each group that were 28 and 32 weeks gestation respectively). All infants were without prenatal or postnatal complications.
Protocol
The study was approved by the Southern Regional Health Authority Ethics Committee, New Zealand (protocol no. 97/04/036). Informed consent was obtained from the parent(s) of all infants studied. Infants were monitored over two consecutive nights in their own home in their usual sleep situation: bed-share or cot-sleep. The first night involved video recording only and the second night involved video and physiological recording. Information was collected on layers of over-bedding, under-bedding, and infant clothing used on the study night.
Physiological recordings
The infant was set up for the study during the hour before usual bedtime. This involved placement of ECG electrodes (modified lead II position), a pulse oximeter probe around the foot for measurement of heart rate and arterial oxygen saturation from the pulse oximeter (Nellcor N-200, Nellcor Hayward, CA, USA), and respibands around the chest and abdomen for measurement of respiratory pattern by inductive plethysmography (Respitrace model 150; Respitrace Co., NY, USA). A thermistor (EdenTec Corporation, Eden Prairie, MN, USA) was attached under the infant’s nares to monitor respiratory flow. Rectal and peripheral (shin) temperature were measured using semiconductor devices with a relative accuracy of 0.01°C. Temperature measurements were sampled at 1 Hz. Ambient temperature was recorded 30 cm from the ground.
Leads from sensors were secured together as a 4 metre “umbilical cord” arrangement connected to the recording apparatus. All physiological signals were relayed through the hardware/software system of a portable polygraphic system (BabyLog Link; Christchurch Hospital, NZ).
Video recordings
A small surveillance camera (Panasonic CEC-C38, Japan) and infrared light source allowed recordings on a time-lapse video recorder (Panasonic AG-TL700) of the infant’s position, movements, and parent/infant interactions.
Data analysis
Temperature data
Overnight temperature profiles for bed-share and cot-sleep infants were produced from BabyLog data records by calculating the mean rectal, shin, and ambient temperatures for each 30 minute epoch, commencing when the infant fell asleep in bed until final waking in the morning, including when the infant was awake or feeding. Figure 1 shows typical examples of temperature profiles from one infant.
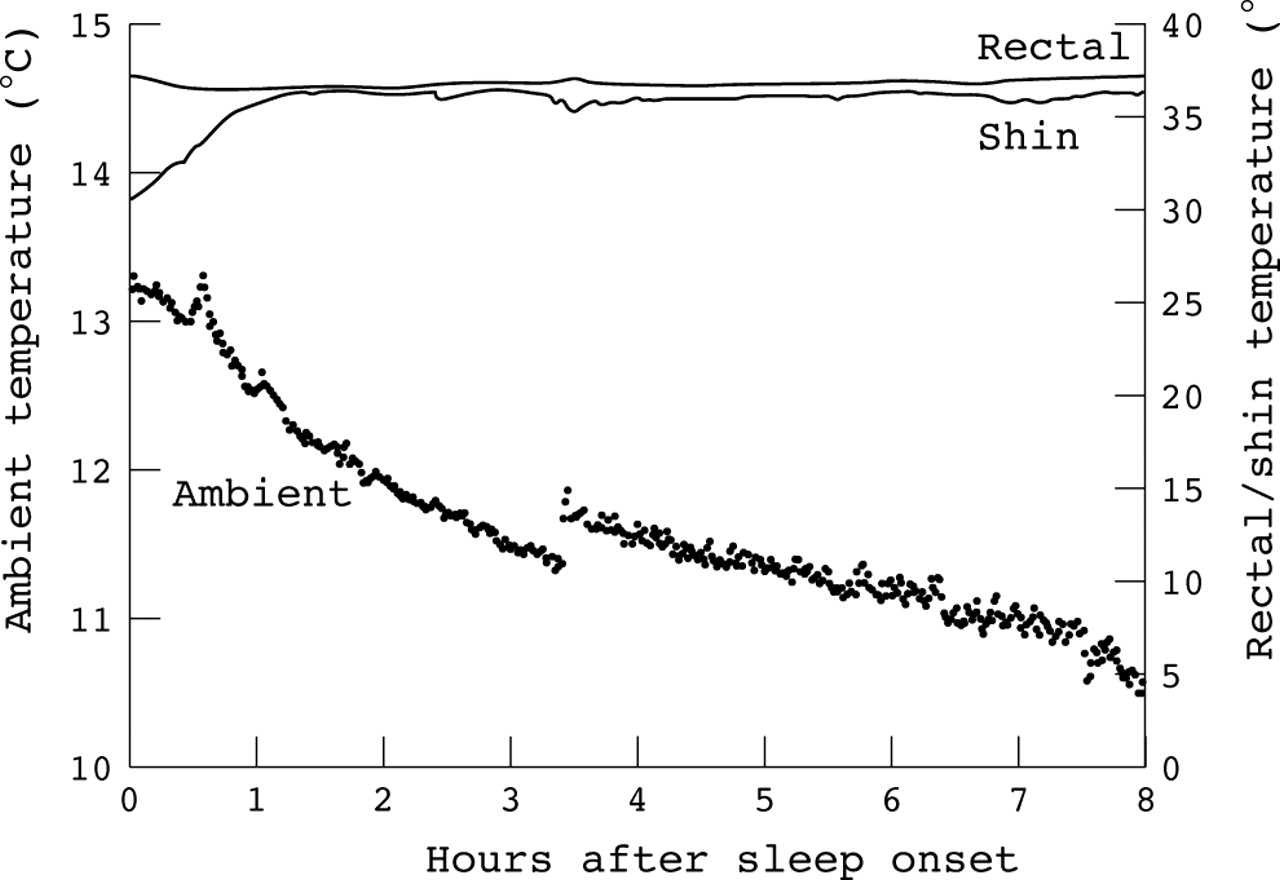
Profile of the rectal, shin, and ambient temperature averaged every minute during an overnight sleep study from one bed-sharing infant.
Off-line video data analysis incorporated C Video software (Envisionology, CA) to link the time counter from the video recorder with a key command on the computer enabling the start and end times for each behavioural event (for example, waking) to be logged into the database (File Maker Pro 2.0, Claris Corporation, USA). Sleep and awake periods were identified from the video. Sleep was defined as starting after the infant was settled for two minutes. Arousals lasting more than two minutes were described as “awake”. The infant’s sleep position, movements, episodes of face covering by blankets, and number of feeding sessions were observed from the video and logged on the database. Any separate feeding initiated within 30 minutes of the previous session was included in that session.
Thickness of bedding and clothing were estimated using the layers of sheet, blankets and duvets, and itemised clothing, and applying average measured thicknesses of typical New Zealand bedding and clothing of these types (Wilson, personal communication). Effective “dry” thermal insulation was calculated for bedding and clothing of each infant using a predictive equation developed to estimate thermal resistance of flat multiple-layer combinations of materials.34
Statistical analysis
Although bed-share and cot-sleep infants were matched for age and season of study, data for both members of the pair were not always available. Data were therefore analysed as two groups, and a form of regression analysis, adjusted for infant age and season, was used to take the matching into account for all comparisons. Log transformations were used to calculate the geometric means (to provide a better measure of central tendency than arithmetic means) for the characteristics of the bedding. In this case the results were presented as ratios of the geometric means with 95% confidence intervals. Poisson or logistic regression was used to estimate the relative risk or odds ratio for the bed-sharing group for the variables based on counts or categories using the cot group as the reference group. A random coefficient model with a random effect for participant was used to analyse the temperature data. As the effect of time was different for bed-share and cot-sleep infants, the results are presented as temperature at 2 hours and change per hour from 2 to 8 hours after sleep onset, together with differences between groups and 95% CI.
RESULTS
Table 1 presents characteristics of the two groups of infants. Study groups were comparable with respect to gestational age, birth weight, sex ratio, and age and weight at study. All bed-share infants and 35/40 cot infants were breast fed. Of the 40 bed-share infants, 90% bed-shared every night, 22 slept with one adult (three with sibling included), and 18 with two adults (one with sibling included). Table 2 gives the characteristics of the mother; similar numbers were educated to tertiary level, and a small number in both groups were identifyied as Maori. Smoking was more common in the cot group (25%) compared to the bed-sharing group (7.5%). Maternal age was similar (bed-sharing: 28 years (SD 5.6) v cot-sleeping:30 (5.5), p = 0.14). Maternal alcohol consumption was minimal in both groups, ranging from rarely to 3 glasses of wine or beer per week, with 17/40 bed-sharers and 15/40 mothers of cot-sleepers reporting no alcohol consumption during or after pregnancy. Mothers reported ease of breast feeding, a more settled baby, a more natural practice, closeness, and security as reasons for bed-sharing.
Infant group characteristics
Maternal group characteristics
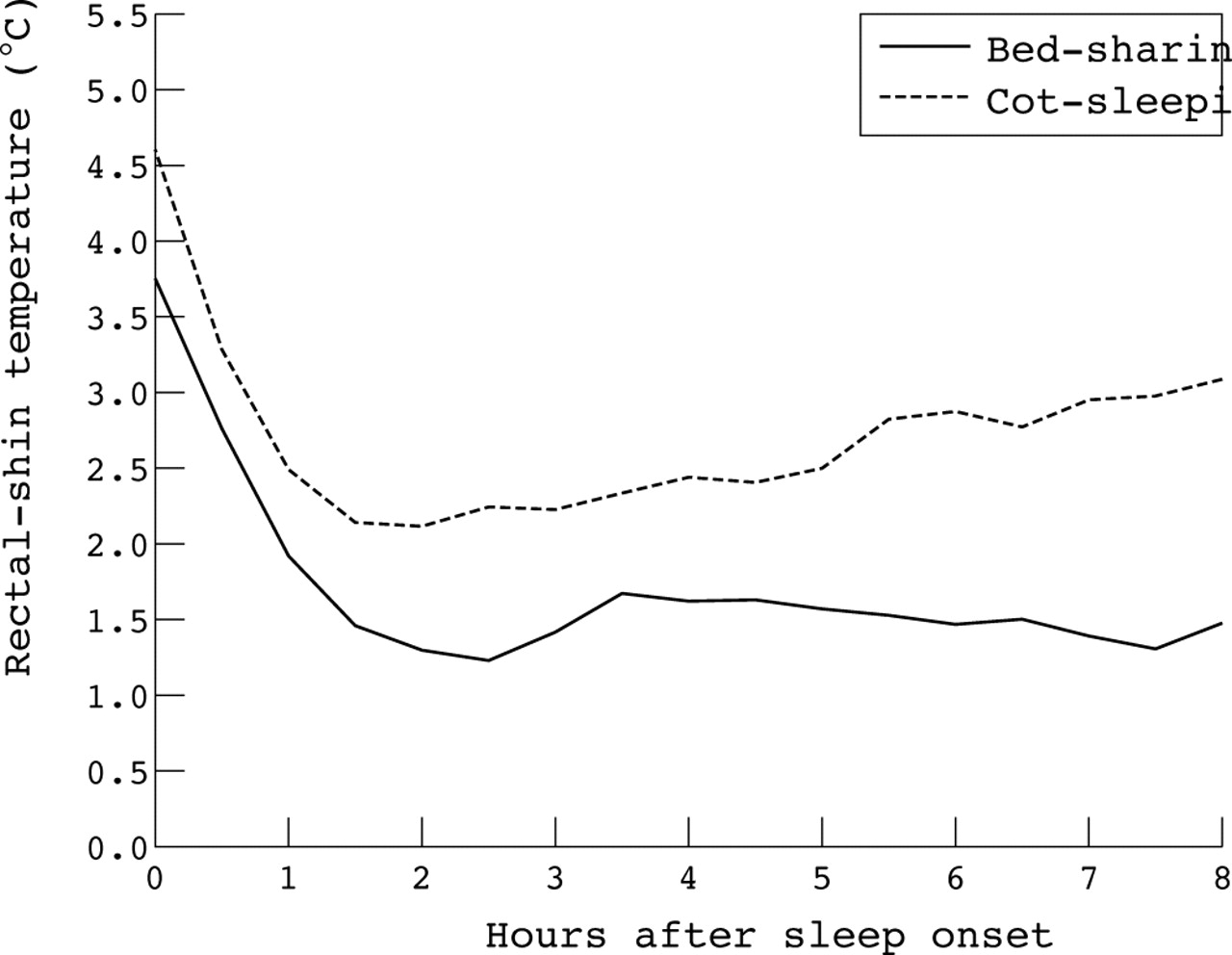
Some parents did not allow infant rectal temperature measurement (12/40 bed-share and 12/40 cot-sleeping), resulting in a smaller subgroup for rectal temperature analysis. Overnight rectal temperature profiles for the two groups, shown in fig 2, illustrate the mean for each 30 minute epoch. Rectal temperature fell to a nadir during the first two hours of sleep followed by a gradual rise throughout the night. Figure 3 shows that overnight shin temperatures of bed-share infants were higher than cot infants from 2 hours after sleep onset. The differences between rectal and shin temperatures are shown in fig 4 as an indication of temperature control responses. Analyses of the differences in overnight temperatures are shown in table 3. The mean rectal temperature at 2 hours after sleep onset for bed-share infants was 36.79°C and for cot-sleeping infants, 36.75°C. Thereafter, temperature increased at a significantly higher rate in bed-share infants (0.04°C/h) than cot-sleeping infants (0.03°C/h). Bed-share infants had a higher shin temperature than cot-sleeping infants at 2 hours (35.43 v 34.60°C) and a higher rate of change thereafter (0.04 v −0.10°C/h). Bed-share infants had a significantly smaller rectal-shin temperature difference than cot infants at 2 hours. Thereafter there was no change in the rectal-shin difference in the bed-share group, but an increase in the cot-sleep group. Ambient temperature for the bed-share group was significantly cooler than for the cot group.
Summary of the mean temperature data two hours after sleep onset, including the mean rate of change thereafter (to eight hours after sleep onset)

Overnight mean rectal temperature calculated for 30 minute epochs in the bed-share and cot-sleeping infants.

Overnight mean shin temperature calculated for 30 minute epochs in the bed-share and cot-sleeping infants.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Overnight mean rectal-shin temperature difference calculated for 30 minute epochs in the bed-share and cot-sleeping infants.
Table 4 shows the estimated effective thickness for bedding and clothing for the two groups of infants. Bed-sharing infants had significantly thicker bedding and hence more thermal insulation than cot-sleeping infants. The thermal insulation of the clothing was not significantly different between groups.
Thermal insulation and heat transfer characteristics of the bedding and clothing of infants
Table 5 summarises further characteristics of the two groups on the night of study that could affect infant temperature. Most bed-share infants slept on their side, while cot infants most commonly slept supine. Only two infants, both cot sleepers, slept prone for the majority of the night. Face covering with overbedding was significantly more common in the bed-share group, with episodes identified from 29 bed-share and five cot infants. During the night, bed-share infants woke significantly more frequently (mean times/night: 4.6 v 2.5) and fed more frequently, although the total time awake was not significantly different between groups. The number of movements per hour was similar between groups.
Characteristics of the infants on the study night
DISCUSSION
This study clearly shows differences in the thermal environment between bed-share and cot-sleep infants sleeping in the parental bedroom. While the difference in rectal temperature between groups at two hours after sleep onset was not significant, the rate of increase in rectal temperature in the bed-share group was slightly higher than that of the cot-sleep group, leading to an increased temperature difference in the latter part of the night. Tuffnell and colleagues30 reported a mean overnight rectal temperature difference of 0.1°C from a retrospective case-control home study of 34 bed-share and 34 cot-sleeping infants (not necessarily in the parents’ bedroom but matched for age, ambient temperature, and estimated thermal insulation from bedding and clothing). In our study, the model predicted a similar rectal temperature difference after approximately eight hours sleep. Sawczenko (personal communication) and Ball31 did not find a significant difference in mean overnight rectal temperature between bed-share and cot-sleep groups where infants shared the parental bedroom in the sleep laboratory. Rectal temperature reflects the outcome of thermoregulatory control. A trend towards a higher rectal temperature found in healthy infants may indicate a potential difficulty for infants with impaired control.
In our study, bed-sharing infants exhibited higher shin temperatures than cot infants; these continued to increase overnight, thus maintaining a consistent rectal-shin temperature difference in the bed-share group. Decreasing shin temperatures in the cot group lead to an increase in rectal-shin difference overnight. Shin temperature reflects the peripheral vasodilatory response to the thermal environment, an indicator of thermoregulatory activity of the infant to maintain a constant core temperature. Bed-share infants had more thermal insulation, largely because of greater use of duvets and perhaps a reduced ability to lose heat due to the proximity of their mother,35 thus requiring more vasodilatation to maintain core temperature. Ambient temperature appeared not to contribute to the higher shin temperature, as this was significantly higher for cot infants, despite matching for season.
Bed-sharing infants were less likely to sleep in the supine position, which is associated with lower overnight rectal temperature than the side or prone position36 and a lower peripheral (foot) temperature.37 In the supine position infants are also more likely to uncover arms and hands36 and this, along with exposure of the face, are key factors in an infant’s ability to dissipate heat.38
Infant rectal temperature rises with waking,28,32 and the decrease on returning to sleep is less than at sleep onset.28 Wailoo et al have shown that rectal temperature remains raised for an hour if the infant feeds during this awake period.39 Bed-share infants have a higher axillary temperature than cot-sleep infants in quiet sleep, associated only with the infants’ frequency of transient arousals with movement.33 The increased shin temperature in the bed-share group may be in part due to increased waking and feeding. However, movements per hour in our study were the same in both groups.
Face covering occurred more often in the bed-share group. Carpenter and colleagues17 report the risk of SIDS associated with being found head covered as an odds ratio of 12.5 (95% CI 6.47 to 24.1) and for evidence of sweating as 2.69 (1.75 to 4.14). As face covered infants become increasingly hot, evaporative heat loss40 and heat loss through bedding become more important. Mathematical modelling suggests that progressive hyperthermia rapidly becomes lethal in infants entrapped by bedclothes.38 Blair and colleagues41 found head covering to be the strongest predictor for SIDS in cot-sleeping infants (OR 18.5) but not bed-share infants. Identification of the position at death is less reliable during bed-sharing due to possible disruption by co-sleepers. The risk associated with head covering during sleep is not clear.
“First night effect” may influence behavioural and physiological recordings,42 although recent publications suggest not.43,44 We compared behavioural data on two consecutive nights from 10 infants, selected randomly, and found no significant difference on key behavioural indices such as sleep-time, number of infant movements/hour, feeds, and sleep position. To minimise “first night effect” we recorded physiological data and analysed behavioural data on the second night.
Although we measured rectal temperature from a small number of infants, some conclusions can be made. Infants were all healthy and despite warmer micro-environments, bed-share infants maintained normal rectal temperatures. Healthy infants, therefore, do not seem to be at increased risk of overheating when bed-sharing. Wailoo and colleagues27 reported that cot-sleeping infants, overwrapped for environmental conditions, maintained normal core temperatures overnight. Infants with high risk factors for SIDS, such as maternal smoking during pregnancy, may have poorly developed thermoregulatory control, placing them at an increased risk of SIDS when exposed to warmer micro-environments present in bed-sharing. Tuffnell45 reported that bottle-fed infants of smoking mothers had higher overnight mean rectal temperatures. We had insufficient smokers’ infants to investigate effects of smoking on thermoregulation. The low number of smokers among the bed-sharers, the high rate of breast feeding and maternal tertiary education, and the active choice to bed-share suggest our sample did not cover the full spectrum of bed-sharers where identified risks associated with bed-sharing are prevalent. Further to this, an association between bed-sharing and breast feeding that has been reported1,46,47 has not been found among inner city, low income families in the USA.48
It appears that bed-sharing infants at low risk of SIDS were in a significantly warmer environment (bedding plus being close to an adult), were more likely to wake and feed, and more likely to become face covered—a potentially significant heat stress. Cot-sleeping infants, on the other hand, were in a heat conservation mode. In this study all infants maintained a normal core temperature. Future studies targeting infants at high risk of SIDS are needed to identify how risk factors might impact on infant and parental behaviour and on vulnerable infant physiology during bed-sharing.
Acknowledgments
This study was supported by a grant from the Health Research Council of New Zealand. The authors would like to thank: Charissa Makowharemahihi and Amanda Phillips for research assistance, Sheila Williams for statistical advice, Christine Rimene for advice on cultural aspects, Cheryl Wilson for data on thickness and thermal insulation of typical single layer New Zealand bedding and infant clothing, and the families that participated in the study.
REFERENCES
Linked Articles
- Perspectives