Article Text

Abstract
Objectives To determine whether the introduction of the capsular group B meningococcal vaccine (4CMenB) in the UK has increased presentations of infants to emergency departments with adverse events following immunisation (AEFI).
Participants, design and setting A retrospective review of hospital records of infants aged 1–6 months presenting to Oxford University Hospitals NHS Trust’s emergency departments from September 2013 to August 2016 with discharge diagnoses of vaccine reactions or non-specific conditions. Immunisation history was checked by reference to centralised immunisation records.
Main outcome measures Presentation classifications were ‘probable vaccine reaction’ (ie, symptoms within 48 hours of immunisation; no alternative cause found), ‘possible vaccine reaction’ (symptoms within 48 hours of immunisation with a possible alternative cause) or ‘not related’ (clear alternative diagnosis or not immunised within previous 48 hours).
Results Prior to 4CMenB introduction (2013–15), an annual average of 12 infants presented with probable or possible AEFIs, increasing to 38 infants in the year following 4CMenB introduction (2015/2016). Rates of AEFIs per 1000 immunisation episodes increased post-4CMenB introduction from 1.03 to 3.4 (p<0.001) at 2 months and from 0.14 to 1.13 (p=0.005) at 4 months. At 3 months, when 4CMenB is not given, no increase was seen (p=0.380). 4CMenB introduction was also associated with increased AEFI-related hospital admissions, invasive investigations and intravenous antibiotic use.
Conclusions The increase in emergency department attendances, investigations and antibiotic use for AEFIs following 4CMenB immunisation may influence the cost-effectiveness of the 4CMenB immunisation campaign.
- immunisation
- general paediatrics
- 4cmenb
- fever
- aefi
Statistics from Altmetric.com
What is already known on this topic?
The capsular group B meningococcal vaccine (4CMenB) vaccine has been known to have postimmunisation fever rates of approximately 61%.
There have been no studies assessing the numbers of infants presenting to Accident and Emergency (A&E) departments with fever due to the 4CMenB vaccine as compared with routine vaccinations.
What this study adds?
This project has shown an increase in the number of children presenting to A&E departments, admitted to hospital, receiving investigations and intravenous antibiotics due to adverse events following immunisation post-4CMenB introduction.
This uncertainty in management highlights the need to develop guidelines for these infants when they present to A&E to minimise increased healthcare consumption.
Introduction
The capsular group B meningococcal vaccine (4CMenB) was introduced into the routine UK immunisation schedule at 2, 4 and 12 months of age in September 2015, with a catch up campaign for all infants born after 1 May 2015. Immunisation coverage of over 90% was achieved, and the vaccine has demonstrated an effectiveness of 83% against capsular group B meningococcal disease.1
The vaccine is known to be relatively reactogenic, with 61% of infants developing a fever above 38°C when receiving a dose of 4CMenB administered concomitantly with routine vaccinations.2 While not harmful in itself, this fever is associated with temporary distress in the child and can be concerning to parents, potentially resulting in them seeking medical assessment in emergency departments. Clinicians assessing these infants may then initiate invasive investigations or intravenous antibiotics given the low threshold for these interventions in febrile infants under 3 months of age.3
In light of this, and given evidence that rates of post-4CMenB fever are reduced by prophylactic paracetamol peri-immunisation, Public Health England have recommended the routine use of paracetamol at the time of immunisation and in the subsequent 24 hours.4
Nevertheless, the potential remains for the introduction of 4CMenB to lead to increased numbers of infants presenting to emergency departments with adverse events following immunisation (AEFIs), and we, therefore, evaluated these presentations and their management in the pre-/post-4CMenB era.
Materials and methods
This retrospective study was conducted as a service evaluation at Oxford University Hospitals NHS Trust, which provides emergency paediatric care for all of Oxfordshire through the Accident and Emergency (A&E) departments at the John Radcliffe Hospital (a tertiary hospital) and at the Horton Hospital (a district general hospital). The discharge summaries of all infants aged 1–6 months presenting to these A&E departments between 1 September 2013 and 31 August 2016 were reviewed to detect potential AEFIs; a period 2 years before and 1 year after the introduction of the 4CMenB vaccine (Bexsero, GSK, Italy) on 1 September 2015. This vaccine was introduced in a 2, 4 and 12-month schedule for babies born on or after 1 July 2015, accompanied by a limited ‘catch up campaign’ for children presenting for their 3-month or 4-month immunisations who were born after 1 May 2015. Other routine immunisations administered in the UK at 2, 3 and 4 months of age are detailed in online supplementary table 1.5
Discharge diagnoses of all infants aged 1–6 months presenting to A and E were analysed to detect AEFIs, either through a discharge diagnosis of postimmunisation reactions or with non-specific presentations or diagnoses (eg, fever, irritability, rash, seizures, floppiness or being acutely unwell). If this assessment was supported by review of the electronic medical notes then the immunisation histories of these children were determined using the Oxfordshire Child Health Computer database to identify administration of any vaccines within the 48 hours prior to presentation. Children with a clear alternative diagnosis were not assessed further.
Children identified as having potential AEFIs in this manner were classified as having presentations that were ‘probably related to immunisation’ (symptom onset within 48 hours of immunisation, no alternative focus found), ‘possibly related to immunisation’ (symptom onset was within 48 hours of immunisation, possible alternative focus found) or ‘not related to immunisation’ (symptoms were not within 48 hours of immunisation or a definite alternative focus was found). Classification of a ‘serious’ AEFI was conducted according to WHO criteria and included inpatient hospitalisation.6
The electronic records of all infants classified as having a probable or possible reaction were independently reviewed by a second investigator and any discrepancies (including classifying events as probable or possible) resolved by re-evaluating clinical notes, pathology results and rechecking immunisation histories from the Primary Care Child Health database.
Further clinical details of children classified as having a ‘probable’ or ‘possible’ vaccine reaction were obtained, including the performance of invasive investigations, admission to the ward or Clinical Decision Unit (CDU, a 24-hour observation facility) and use of intravenous antibiotics. Numbers of infants with ‘probable’ and ‘possible’ vaccine reactions were combined for subsequent analyses to ensure all AEFI’s were included in the analyses.
The number of infants aged 1–6 months presenting with urinary tract infections (UTIs; identified by review of discharge summaries and confirmed by a positive urine microscopy or culture) were also determined and used as a condition that was unrelated to immunisation and could control for potential confounders such as changes in population numbers, referral patterns or health-seeking behaviour.
Patient involvement
As this was a retrospective observational study, patients were not involved in the design or outcome of the study.
Statistical analysis
Infants presenting to A&E before 1 September 2015 (the date of 4CMenB introduction) were classified as belonging to the ‘pre-4CMenB’ era, while those from this date onwards were ‘post-4CMenB.’
The numbers of probable or possible AEFIs at the 2, 3 and 4-month immunisation episodes were divided by the number of immunisations given across Oxfordshire at these ages (obtained from the Oxfordshire Child Health computer database) to determine the rates of AEFIs per 1000 doses of the vaccine. In the pre-4CMenB era, the denominator used was the number of Diphtheria, Tetanus, acellular Pertussis, Inactivated Polio Vaccine, Haemophilus influenzae type b (DTaP-IPV-Hib) vaccines administered at 2, 3 and 4 months; in the post-4CMenB era, it was the number of doses of 4CMenB (2 months), DTaP-IPV-Hib (3 months) and 4CMenB (4 months). Confirmation that an AEFI occurring at 2, 3 and 4 months of age represented an association with the first, second and third scheduled immunisation was made by reference to the child health computer database.
For each of the 2, 3 and 4-month immunisation episodes, as well as the combined 2 and 4-month episodes, the χ2 test was used to assess the association between 4CMenB era and presentation with possible or probable AEFI. Results are presented as ORs and 95% CIs with corresponding p values.
The rates of the clinical interventions (ward and CDU admissions, blood tests, lumbar punctures and intravenous antibiotics) were calculated per 1000 doses of vaccine for the 3-month and combined 2-month and 4-month immunisation episodes. For each intervention, the association with 4CMenB era was tested using the χ2 test and results are reported as ORs.
Children receiving 4CMenB at 3 months of age in the ‘catch-up’ campaign were analysed separately and excluded from the analysis of AEFIs across the age range of 1–6 months to better represent likely AEFIs seen in an ongoing ‘routine’ immunisation schedule. In instances where expected numbers were too small for the χ2 test to be valid, Fisher’s Exact test was used. For all analyses, a p value of <0.05 was considered significant. All data were analysed using the Statistical Package for the Social Sciences (SPSS) V.22.
Results
Presentations to A&E
Over a 3-year period, 5209 infants aged 1–6 months presented to the John Radcliffe (n=4626) and Horton hospitals (n=583) with potential AEFIs (online supplementary figure 1). A total of 62 probable or possible AEFIs were identified (figure 1), all of which had their immunisation histories confirmed using the Primary Care Child Health database. The mean annual incidence of AEFI presentations prior to 4CMenB introduction was 12 per year compared with 38 in the year post-4CMenB introduction (24 out of 3342 presentations pre-4CMenB, 38/1867 presentations post-4CMenB, p<0.0001). In contrast, the numbers of presentations with UTIs in this age group remained stable (26.5 per year in the pre-4CMenB era and 24 in the year post-4CMenB). In contrast, there was no statistically significant difference in the number of UTIs between the pre-4CMenB and post-4CMenB eras (53/3342 and 28/1867, respectively, p=0.81)
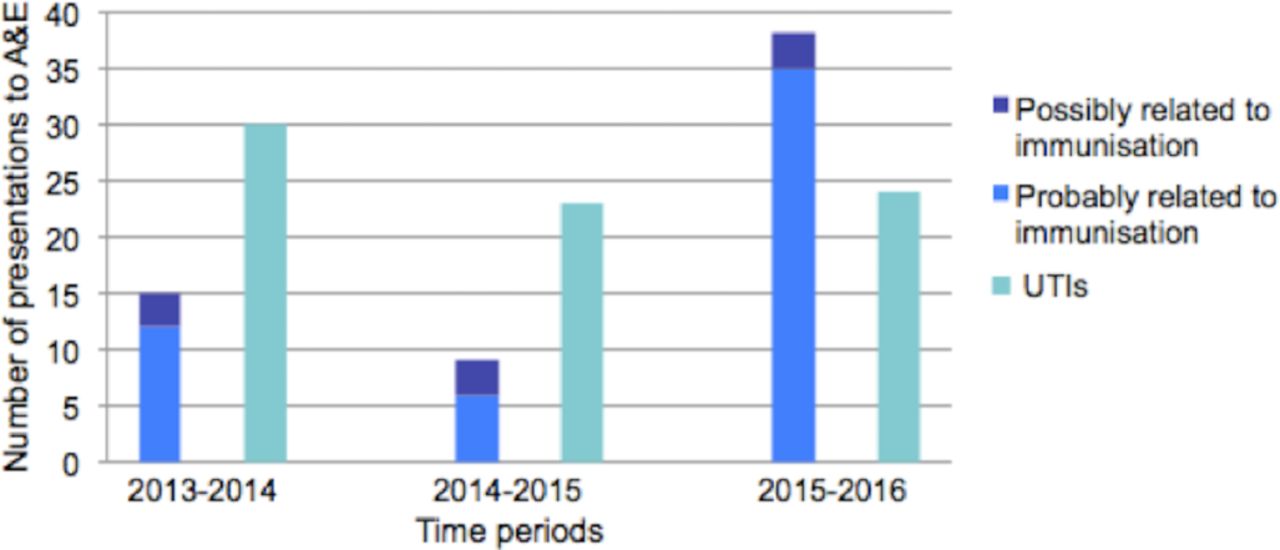
Number of presentations to A&E for probable and possible AEFIs and for UTIs per year. A&E, accident and emergency; AEFI, Emergency Departments with Adverse Events Following Immunisation; UTI, urinary tract infection.
The rates of A&E presentations for AEFIs (possible and probable combined) per 1000 vaccines administered at 2, 3 or 4 months in Oxfordshire are shown in table 1 and online supplementary figure 2. These increased significantly in the post-4CMenB era following the immunisation episodes at 2 months (1.03/1000–3.4/1000) and 4 months (0.14/1000–1.13/1000). No similar increase was observed for the 3-month immunisation episodes, when no 4CMenB vaccine is administered in the routine schedule. Of note, when infants aged 3 months received 4CMenB together with routine vaccines in the ‘catch-up’ campaign, 6.76 AEFIs were seen per 1000 doses; almost double the rate observed in infants aged 2 months in the post-MenB era. Overall, there were 2.36 presentations for AEFIs per 1000 doses of 4CMenB administered during routine immunisation at 2-month and 4-month immunisation episodes, compared with 0.59 per 1000 doses at these times in the pre-4CMenB era (OR (95% CI)=4.0 (2.2 to 7.2), p<0.001).
AEFIs by age at immunisation and expressed in terms of numbers of doses of routine or 4CMenB vaccines
Clinical interventions following routine 4CMenB immunisation at 2 and 4 months of age
Following immunisation at 2 and 4 months of age, 23 of the 32 (71.9%) children presenting with AEFIs were admitted to hospital for AEFIs in the post-4CMenB era (13 to the ward and 10 to the CDU); thus meeting a WHO criteria for a serious AEFI. This compares with 7 of 17 (41.2%) in the pre-4CMenB era (four to the ward, three to the CDU), representing an increase in rates of ward admissions from 0.14 (in the pre-4CMenB era) to 0.96 (in the post-4CMenB era) per 1000 immunisation episodes and to the CDU from 0.10/1000 to 0.74/1000 (figure 2A).

{kind=link}
{kind=link}
Rates of clinical intervention for probable or possible AEFIs per 1000 doses of vaccine by pre-/post- 4CMenB era, for (A) 2-month and 4-month immunisation episodes combine and (B) 3-month immunisation episodes. ORs and 95% CIs are presented above the x-axis in each plot. There are no ORs for when there were no cases. 4CMenB, capsular group B meningococcal vaccine; AEFI, Adverse Events Following Immunisation; CDU, Clinical Decision Unit.
Lumbar punctures were performed on 21.9% of children 2 and 4 months of age presenting with AEFIs in the post-4CMenB era (7/32), compared with 17.6% in the pre-4CMenB era (3/17), an increase from 0.1 to 0.52 per 1000 immunisation episodes (figure 2A). In the post-4CMenB era, the likelihood of receiving a lumbar puncture was similar at 2 and 4 months of age (5/25 (20%) and 2/7 (28.6%) respectively).
Venepuncture (for blood cultures, full blood counts and/or CRP) was performed in 12/32 (37.5%) of children presenting with AEFIs following 4CMenB immunisation at 2 and 4 months, compared with 6/17 (35.3%) in the pre-4CMenB era, an increase from 0.21 to 0.89 per 1000 immunisation episodes (figure 2A). Rates of intravenous antibiotics were similarly increased (figure 2A).
By contrast, figure 2B shows that there was no statistically significant increase in rates of admissions, lumbar punctures, blood tests or intravenous antibiotic use after immunisation at 3 months of age in the pre-4CMenB versus post-4CMenB era (not including children presenting with 4CMenB administered at 3 months in the ‘catch-up’ campaign).
Discussion
This study has shown an increase in presentations to A&E for AEFIs since the introduction of the 4CMenB vaccine from 1 in 972 doses to 1 in 295 at the 2-month immunisation episode, and from 1 in 7043 doses to 1 in 881 at the 4-month immunisation episode. This has been associated with an increase in hospital admissions (classified as serious AEFIs), invasive investigations and use of intravenous antibiotics.
Despite this being a retrospective study, the risk of overlooking any presentations due to AEFIs was minimised by reviewing all relevant presentations in the age groups of interest rather than relying on clinician assessment alone. Conversely, any child with an identified alternative cause for their symptoms (eg, microbiologically confirmed sepsis or meningitis) was excluded. Nevertheless, an element of diagnostic uncertainty remains, particularly as some infants were treated for sepsis. However, a real and causally related increase in AEFI presentations following 4CMenB introduction is supported by the consistency of assessment methods used for the pre-/post-4CMenB eras, the lack of changes in presentations due to a control condition (UTIs) and the specificity of the increases to the 2-month and 4-month immunisation episodes, as opposed to 3 months (when no 4CMenB immunisation is given). Also, while calculations about rates of AEFIs per vaccine administered requires assumptions that all children immunised in Oxfordshire sought emergency department management in this county and that no children seeking emergency care in Oxfordshire had been immunised elsewhere, it is expected that these factors would be unchanged in the pre-/post-4CMenB eras.
While these data reflect the first ‘real-life’ evidence on the impact on hospital healthcare consumption of AEFIs observed following routine introduction of the 4CMenB vaccine, relevant data were obtained in a phase 3 study evaluating all medically attended post-immunisation fever in a 2, 4 and 6-month schedule of 4CMenB and routine vaccines.7 Overall rates of medically attended fever following immunisation were higher in this trial than in our study (21.9/1000 following immunisation episodes containing 4CMenB) likely reflecting its inclusion of primary care as well as hospital services. Strikingly, despite lower rates of fever in children immunised with routine vaccines than after 4CMenB and routine vaccines, rates of medically attended fever in the routine-only group were at least as high as those after 4CMenB (22.14/1000 immunisation episodes). An increase in medically attended fever following 4CMenB was observed only in a ‘blinded’ subgroup within this study by Vesikari et al, raising the possibility that parental education about the likelihood of postimmunisation fever might reduce subsequent health seeking behaviour. It was also anticipated that medically attended AEFIs could be minimised by recommendations to use prophylactic paracetamol at the time of immunisation as this was shown to reduce rates of fever (≥38.5°C) from 70.3% to 39.1% without impacting on vaccine immunogenicity.4 8 Whether or not parents presenting their child to A and E with AEFIs had followed this advice was not determined in this study due to its retrospective nature but is an area that warrants further research. Also relevant to the use of paracetamol around the time of immunisation are two studies suggesting that this could impact on vaccine immunogenicity.8 9 Of note is that neither of these studies involved 4CMenB, and the one study evaluating the impact of paracetamol on the immunogenicity of a schedule that included 4CMenB showed no significant effect.10
While additional research is required to confirm these findings across a great number of hospitals, and over a longer period of time, our data suggest that clinicians will have to manage infants aged 2 months presenting with AEFIs more frequently. A particular challenge for clinicians is distinguishing AEFIs from coincidental sepsis in this vulnerable age group (for which full septic screens are recommended for fever without a focus).3 We have not attempted to differentiate these presentations in this study (and any children with confirmed sepsis were excluded from our analysis); however, further research to guide decision making and guideline development in this area may reduce the number of invasive investigations performed in these infants. As the vaccine only started being given to infants aged 12 monthsin May 2016, it would also be of interest to study both the rates of AEFIs and the impact of the known risk of febrile seizures at this age.7 Preliminary results from a general practice database survey led by Public Health England also suggest an increase in primary care consultations and this research is ongoing.11
These data should not detract from the success of the 4CMenB immunisation campaign, which has halved the number of cases of group B meningococcal disease in the immunised cohort.1 It should also be emphasised that the AEFIs described here are temporary and would not be expected to have long-term consequences, in contrast to the devastating impact that invasive meningococcal disease can have. Nevertheless, countries considering routine introduction of 4CMenB should expect an increase in AEFI-related medical consultations, and further research is required to determine how these can be minimised.
Acknowledgments
The authors wish to thank Karyn Gokcil and Annette Sandrawich from the Oxfordshire Child Health Information Services—South, Central and West CSU for their assistance in determining immunisation histories.
Footnotes
Contributors MDS conceived the study. VN wrote the initial draft as well as all subsequent drafts, which were all edited by UG, MS and JB.
Funding This project was internally funded. We have received support from the NIHR Oxford Biomedical Research Centre and a travel grant from Monash University Department of Paediatrics.
Competing interests MDS is currently, or has been, a principal investigator on clinical trials funded and/or sponsored by vaccine manufacturers including GlaxoSmithKline, Pfizer, Medimmune and Johnson and Johnson. MDS has also spoken at industry sponsored symposia and contributed to advisory boards. This work is undertaken on behalf of the University of Oxford. JB is an investigator on clinical vaccine trials or observational studies sponsored by vaccine manufacturers including Novavax, Pfizer and MedImmune. JB also serves on data safety monitoring committees for Sequiris. This work was undertaken on behalf of Monash Health.
Ethics approval Permission to conduct this study as a service evaluation was obtained through the OUH NHS trust, thus the study did not require approval from an NHS ethics committee. Low-risk ethical approval was granted by Monash University.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Original article
- Original article
- Atoms