Article Text

Abstract
Objective To investigate a possible association between fever admissions and 4 component Meningococcal B (4CMenB).
Design 4CMenB is given at 8 and 16 weeks in the first year of life. Self-controlled case series using linked routinely collected healthcare data, where the risk period was the 3 days immediately following receipt of a vaccine dose.
Patients Children aged under 1 year in Scotland preintroduction and postintroduction of 4CMenB vaccine (pre—September 2014 to August 2015 and post—September 2015 to June 2016).
Main outcome measures Hospitalisations for fever attributable to 4CMenB vaccine.
Results The postintroduction model showed an increased risk in the 3 days after dose 1 (relative incidence (RI), 10.78; 95% CI: 8.31 to 14.00) and dose 3 (RI, 9.80; 95% CI: 7.10 to 13.62), with a smaller increased risk after dose 2 (RI, 2.20; 95% CI: 1.27 to 3.82). The magnitude of these effects was greater than in the preintroduction model. The attributable fractions were 90.7%, 54.8% and 89.7%, equating to 162, 14 and 84 vaccine attributable cases per 100 000 doses, respectively.
This is equivalent to 102 extra hospitalisations in Scotland annually, based on a birth cohort of 55 100 and extrapolated to 1430 across the UK based on a birth cohort of 777 165.
Conclusion There is an increased risk of hospital admission with fever within 3 days of the routine childhood immunisations at 8 and 16 weeks following introduction of 4CMenB vaccine. The results indicate that further understanding of the current use of prophylactic paracetamol is needed. Communication to parents and health professionals may also need to be re-examined, and guidance on the use of prophylactic paracetamol reinforced.
- Menb
- Vaccination
- Fever
Statistics from Altmetric.com
What is already known on this topic?
Fever occurs at increased levels following 4 component Meningococcal B (4CMenB) vaccination, leading to prophylactic paracetamol being recommended for doses at 8 and 16 weeks.
Adherence to this recommendation is not known.
What this study adds?
There are an estimated extra 1440 hospitalisations for fever associated with 4CMenB vaccine each year across the UK.
Parents and vaccine providers should be reminded about the importance of giving paracetamol before 4CMenB vaccination, not waiting until fever develops.
Introduction
Meningococcal disease is a systemic bacterial infection caused by Neisseria meningitidis, an organism commonly carried harmlessly in the nasopharynx.1 In the UK, meningococcal disease serogroup B is responsible for the highest number of cases and remains the main cause of infant deaths from infectious disease.2 The disease has a rapid onset, and even with prompt treatment, survivors can be left with serious long-term sequelae such as deafness, epilepsy and limb amputations.3 Vaccination is therefore the most effective control measure. Although recent years have seen a decline in meningococcal disease across the UK, new virulent strains can arise resulting in national outbreaks such as serogroup W, which prompted the introduction of meningococcal ACWY (MenACWY) vaccine into the adolescent and student programmes.2 4
The 4 component Meningococcal B (4CMenB) vaccine, Bexsero, was introduced in Scotland in September 2015 and offered to all babies born on or after 1 July 2015 at their routine appointments at 8 weeks, 16 weeks and 12–13 months.5 There was also an initial catch-up programme for babies born on or after 1 May 2015 and who were attending for vaccinations at 3 and 4 months. Fever is a known side effect when 4CMenB is administered alongside other routine vaccines, with highest rates within 6 hours. Other side effects such as irritability, drowsiness and loss of appetite were also reported.6–8 Results of a clinical trial indicated that administration of prophylactic paracetamol significantly reduced reports of fever by 40%–50%; to around the expected occurrence prior to the introduction of 4CMenB. Reports of other symptoms were also reduced.9 As a result, the UK Joint Committee on Vaccination and Immunisation (JCVI) recommended 3 doses of infant paracetamol following vaccinations at 8 and 16 weeks, with the first dose given at the time of the vaccination followed by two further doses at 4–6-hour intervals, regardless of whether fever develops.4
Suspected adverse events following immunisation (AEFI) is reported to the UK Medicines and Healthcare Products Regulatory Agency via the yellow card scheme. We developed a supplementary method to proactively identify potential AEFI resulting in hospital admission.10 This has been used to monitor rotavirus, shingles, human papillomavirus and more recently 4CMenB vaccines. Ongoing monitoring showed a signal for fever admissions corresponding to the start of the 4CMenB programme. Due to inherent time lags in completion of hospital admission data, this pattern of repeating signal became more conclusive after a few months. We therefore decided to investigate, conducting a self controlled case series (SCCS) analysis, using linked routine healthcare data. This method has previously been used to investigate potential AEFI, having advantages including control of sex, location and underlying health.11–13
Methods
SCCS analysis
All general and acute inpatient and day cases in hospitals across Scotland (SMR01) were included for children aged less than 1 year and records extracted using predefined International Classification of Diseases 10 (ICD10) code. SMR01 data is held by the Information Services Division, and unit of analysis is an ‘episode’. An episode is generated when a patient is discharged, transferred between hospitals or specialties or to a different consultant. Episodes are grouped as continuous inpatient stays (CIS), and each CIS is defined as a case.
Fever cases were extracted from September 2014 until July 2016 for infants using the ICD10 code ‘R50’ and included if recorded in any diagnostic position during the hospital stay. Age was defined as on admission.
Vaccination records for all children born between January 2013 and August 2016 were extracted from the Scottish Immunisation & Recall System (SIRS). This study concentrated on vaccinations given at 8, 12 and 16 weeks. Combined diphtheria, tetanus, pertussis, polio and Haemophilus influenzae type B (DTaP-IPV-Hib) vaccine records were examined, to enable a consistent comparator preintroduction and postintroduction of 4CMenB. In Scotland, uptake rates by 12 months of age for complete primary courses of immunisation against DTaP-IPV-Hib are high, with rates around 97%. Uptake of 4CMenB vaccine for the first routine cohort (born July 2015) was 95.7% for one dose and 82.4% for two doses of vaccine at 6 months of age, rising to 94.5% for two doses at aged 12 months.14 15 Table 1 shows the current routine childhood schedule for infants.
Routine childhood immunisation schedule in Scotland (2016)
Vaccination records were matched with fever cases using the Community Health Index (CHI) number. Fever cases without a CHI number were excluded, which resulted in one case being excluded. Patients were included whether they had received no, partial or full (three) doses of DTaP-IPV-Hib. Eight fever cases did not match to SIRS records and were included as non-vaccinated patients.
Patients were excluded if the time between birth and first dose of DTaP-IPV-Hib was less than 20 days as it was assumed to be due to inaccurate recording, resulting in exclusion of five fever cases.
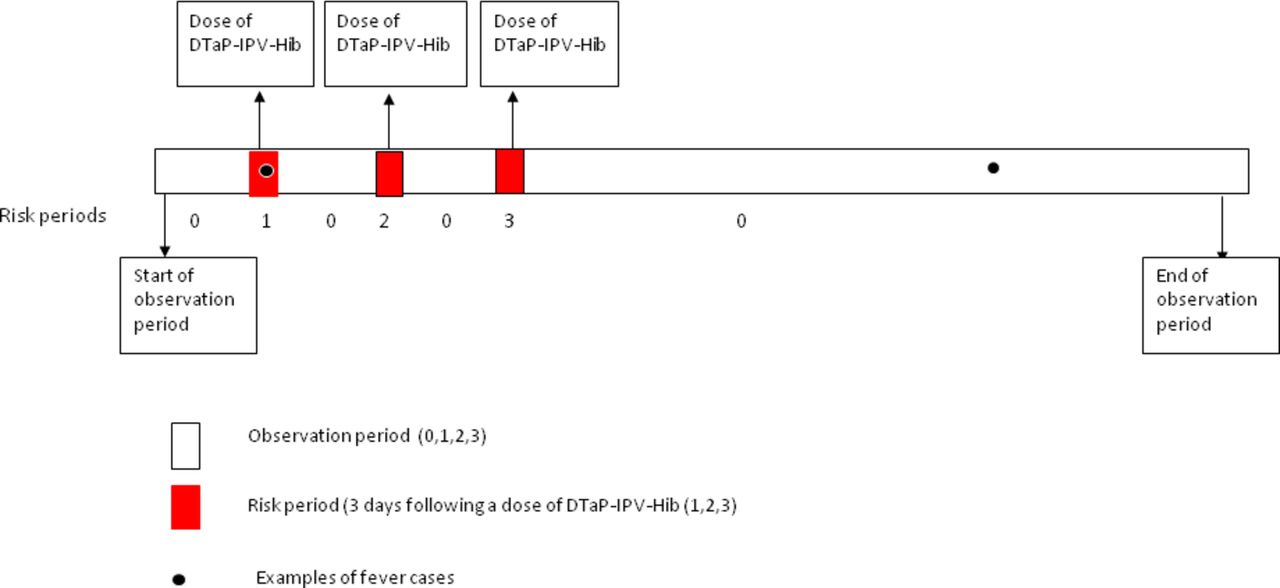
Age in days at vaccination and fever admission was calculated, and the risk period was defined as 3 days post-DTaP-IPV-Hib vaccination. Figure 1 shows an example of a SCCS design of a single patient timeline with two fever admissions.

{kind=link}
Design of self controlled case series showing an example of a single patient timeline with two fever events. DTaP-IPV-Hib, diphtheria, tetanus, pertussis, polio and Haemophilus influenzae type B.
The analysis was based on each case of fever, rather than just the first case for each patient, consistent with study methodology. The rationale was that the risk after each vaccine dose at 8, 12 and 16 weeks would differ due to the differences in vaccination schedule; therefore, each dose was assigned a different risk factor (1, 2 and 3). The observation period (the rest of the year) was assumed to have the same ‘risk’ and therefore coded as 0 (figure 1).
The data were split into pre-4CMenB and post-4CMenB vaccine introduction, from September 2014 to August 2015 and from September 2015 to June 2016, respectively, and the relative incidence (RI) for each time period was calculated. In the pre-4CMenB vaccination period, the RI refers to the DTaP-IPV-Hib doses, whereas in the post-4CMenB vaccination period for DTaP-IPV-Hib/4CMenB doses. Comparison of the two sets of RI gives the impact of the 4CMenB vaccine.
The RI compares the period 3 days after vaccination for an individual to all days not included in that period for the same individual. Age was included as a covariate, taking different values every 30 days. The analysis was carried out as a conditional logistic regression, stratified by individual, with covariates of age group and whether or not the individual was in or out of the exposure period. The age group effect was used to control and adjust for the different hospitalisation rates in, for example, months 0–6 compared with months 6–12, and so the effect of the exposure period takes into account the known differences in hospitalisation rates associated with age. Age was restricted to those who were under 1 year of age at admission.
The case series analysis was carried out in R using the clogit function in the survival package to account for the repeated observations on the subjects and an offset of the logarithm of the interval length to account for the exposure period. The attributable fractions were calculated using the RI (RI−1)/RI × 100 for each risk period of 3 days after each dose of DTaP-IPV-Hib. This was applied to calculate the attributable number of cases and a rate calculated using the relevant midyear population estimates. CIs were obtained using a parametric bootstrap approach where the log relative risks were sampled from a normal distribution, and the numbers of cases from Poisson distributions were centred at the observed values. Medians and upper and lower 2.5% percentiles are reported from the 10 000 bootstrap simulations.
Analysis of admissions for all seizures including febrile seizures
SMR01 data was extracted for admissions for all cause seizures including febrile seizures (R56, G40 and G41) within 3 days of the routine child vaccinations at 8, 12 and 16 weeks and compared prevaccine and postvaccine introduction and tested for significance by a two-sample z-test.
Analysis of lumbar puncture procedures
SMR01 data was extracted for admissions which included lumbar puncture procedures (LP) using OPCS Classification of Interventions and Procedures version (OPCS4) codes ‘A553’, ‘A558’ and ‘A559’ from 2011 to 2016 within 3 days of the routine child immunisations at 8, 12 and 16 weeks and compared prevaccine and postvaccine introduction and tested for significance by a two-sample z-test.
Analysis of length of stay
Length of stay was calculated from the extracted SMR01 data within 3 days of the routine childhood vaccinations at 8, 12 and 16 weeks and compared prevaccine and postvaccine introduction and tested for significance by a two-sample z-test.
Results
SCCS analysis
Table 2 presents the number of fever cases preintroduction and postintroduction of 4CMenB programme, with a total of 1435 fever cases identified; 670 before 4CMenB introduction and 765 following introduction of the programme.
Number of hospital admissions for fever pre-4CMenB and post-4CMenB vaccine introduction
In the preintroduction model, there was a significantly increased risk in the 3 days after both dose 1 and dose 3 of DTaP-IPV-Hib (RI, 3.01; 95% CI: 1.99 to 4.53 and RI, 2.51; 95% CI: 1.47 to 4.27) (table 3). The attributable fractions were 66.8% and 60.1%, respectively. Calculation of vaccine attributable cases, based on an approximate vaccine uptake of 95%, was equivalent to 33 (95% CI: 20 to 49) and 16 (95% CI: 7 to 28) cases per 100 000 doses, respectively. Dose 2 was not associated with an increased risk of fever admission (RI, 0.43; 95% CI: 0.14 to 1.36).
Relative incidence of fever admission and attributable cases (per 100 000 vaccinations) in the 3 days following vaccination with DTaP-IPV-Hib dose preintroduction and postintroduction of pre-4CMenB
The postintroduction model showed a greater increased risk in the 3 days after both dose 1 (RI, 10.78; 95% CI: 8.31 to 14.00) and dose 3 (RI, 9.80; 95% CI: 7.10 to 13.62) with a smaller increase risk after dose 2 (RI, 2.20; 95% CI: 1.27 to 3.82), compared with the preintroduction model. The attributable fractions were 90.7%, 54.8% and 89.7%, equivalent to 162 (95% CI: 129 to 195), 14 (95% CI: 5 to 25) and 84 (95% CI: 62 to 109) vaccine attributable cases per 100 000 doses, respectively (table 3).
The total number of additional hospitalisations was estimated by comparing attributable cases before and after the introduction of 4CMenB vaccine. Therefore, following dose 1, the attributable cases would be 128/100 000 (95% CI: 93 to 165), which in a birth cohort of 55 100 (Scotland 2015) is equivalent to 68 (95% CI: 49 to 90) hospitalisations, extrapolated to 940 (95% CI: 680 to 1210) in the whole UK (UK, 2015). Similarly, for dose 3, the attributable cases would be 67 (95% CI: 43 to 94) per 1 00000 equating to 35 extra hospitalisations in Scotland (95% CI: 22 to 50) and 490 (95% CI: 310 to 690) in the UK. Therefore, combining doses 1 and 3 together, this would amount to 102 (95% CI: 80 to 126) extra hospitalisations in Scotland per year or 1430 (95% CI: 1120 to 1770) across the UK.
All seizures including febrile seizures
The proportions of seizure cases within 3 days of the routine childhood immunisations at 8, 12 and 16 weeks were compared prevaccine and postvaccine introduction. There were 12/765 (1.57%) cases preintroduction period (September 2013 to August 2015) compared with 8/374 (2.13%) in the postperiod (September 2015 to August 2016) (p=0.49).
Lumbar punctures
The proportions of LPs within 3 days of routine childhood immunisations at 8, 12 and 16 weeks were compared prevaccine and postvaccine introduction. There were 17/520 (3.27%) in the preintroduction period compared with 22/408 in the postintroduction period (5.39%) (p=0.11). Therefore, although there has been a small increase in the proportion of LPs postintroduction of 4CMenB in the 3 days following routine vaccinations, it is not statistically significant. However, as the absolute numbers are very low, this may need to be monitored further.
Length of stay
Most cases had a short length of stay of either ‘0’ or ‘1’ day. Following 4CMenB introduction, the increase was observed in short length of stays particularly with the ‘0’ day stays outnumbering the ‘1’ day stays approx 2:1. Following dose 1, there were 13/27 (48.1%) of cases of <1 day length of stay pre-4CMenB introduction compared with 48/95 (50.5%) (p=0.83). Following dose 3, there were 8/15 (53.3%) cases of <1 day length of stay pre-4CMenB compared with 26/51 (50.9%) post-4CMenB (p=0.87).
Discussion
This study has demonstrated the usefulness of proactively monitoring hospital admission data for potential adverse events following immunisation and the ability to further investigate by linking to vaccination records using the CHI number.
The results have shown a significant increased risk of hospital admission with fever within 3 days of the routine childhood immunisation schedule at 8 and 16 weeks (doses 1 and 3) following introduction of 4CMenB. There was also a small but significant risk following vaccinations at 12 weeks postintroduction of 4CMenB. This is likely related to the catch-up campaign at the start of the programme as admissions mainly occurred in the first couple of months of the programme.5 The results indicated that markers of severity such as all cause convulsions (including febrile), lumbar punctures and length of stay were not significantly increased consistent with clinical trial findings.8
To provide context, we estimated the number of additional hospitalisations by comparing attributable risk preintroduction and postintroduction of 4CMenB vaccine as equivalent to 103 extra hospitalisations annually in Scotland and 1440 across the UK.
Analysis of lumbar puncture procedures was also carried out pre-4CMenB and post-4CMenB vaccine. There is currently insufficient evidence that observed increase is associated with 4CMenB; however, as the numbers are low, this may need to be monitored further. This is particularly relevant as current guidance from the National Institute for Health and Care Excellence on management of fever in under 5 s recommends lumbar puncture is carried out on all infants aged 1–3 months with fever who appear unwell.16
An increased risk of fever admissions prior to the introduction of the 4CMenB following vaccinations at 8 and 16 weeks (doses 1 and 3) was observed. This timing coincides with pneumococcal conjugate vaccine (PCV) administration. Fever is mentioned as a potential adverse reaction for PCV with an increased level observed in clinical trials.17 However, the rates of admission were significantly higher following the introduction of 4CMenB vaccine.
The increased risk of fever associated with 4CMenB vaccine when given along with other routine vaccinations is a known adverse event.8 However, results of a phase 2 randomised controlled trial indicated that giving prophylactic paracetamol reduced postvaccination reactions including fever without impacting on immunogenicity.9 Therefore, the JCVI recommended prophylactic paracetamol at the time of the vaccinations followed by a further two doses even in the absence of fever.4 Adherence to this recommendation is not known. It is possible, particularly given the very young age of infants at the time of the first vaccination, that there may be some reluctance to give paracetamol before a fever is actually evident, which would reduce its impact. It is therefore unclear if any of these hospitalisations were avoidable. This is further strengthened by an initial analysis of community prescribing data from September 2015 until October 2016 which showed that approximately 1400 prescriptions were written by pharmacists for paracetamol 120 mg/5 mL liquid per month in Scotland, as part of a public health service for prophylaxis of post-4CMenB fever.18 This is lower than expected given the high uptake of 4CMenB and size of the birth cohort (approximately 5000 births per month). It is not known, however, if this represents a real under use of paracetamol or whether parents are not getting prescriptions as they already hold stocks or purchase elsewhere. Recent studies have shown a rise in infants presenting to accident and emergency departments and consulting with general practitioners for fever despite recommendation for prophylactic use of paracetamol.19 20 There may also be other factors which led to the increased risk of fever admissions postintroduction, including parental awareness of fever as a known side effect of 4CMenB vaccine, which we are unable to quantify.
The results indicate that further understanding of the current use of prophylactic paracetamol is needed and that communication to parents and health professionals may need to be re-examined.
Limitations
There are a number of limitations to this study. To include as much data as possible in the postintroduction cohort, we did not limit admissions by date of birth. Therefore, we may not capture every patient’s first full year, that is, patient could be born in February 2016, admitted April 2016 and may or may not have had their vaccines. The post-4CMenB model was limited including a full year’s data due to inherent delay in SMR01 completion at the time of analysis. In addition, we only looked at fever hospitalisations and were not able to assess impact on other areas including primary care consultations and attendances at accident and emergency. Furthermore, we were only able to look at a relatively short period of time following vaccine introduction. However, none of these should alter the overall result of the study, but rather increase its power as further data accumulates.
Conclusion
There is an increased risk of admission to hospital with fever within 3 days of the routine childhood immunisation schedule at 8 and 16 weeks following the introduction of 4CMenB vaccine. Other markers for potential severity, such as seizures and length of stay, have not significantly increased. There is a need for more information on paracetamol use among parents and caregivers. The results indicate that further understanding of the current use of prophylactic paracetamol is needed. Communication to parents and health professionals may also need to be re-examined, and guidance on the use of prophylactic paracetamol reinforced.
Acknowledgments
We gratefully acknowledge the Child Health Team, Information Services Division (ISD) for provision of the SIRS data and William Malcolm, Pharmaceutical Advisor, HPS and Helen Watson, Information Analyst ISD for the preliminary prescribing data. We are also grateful to all across NHS Scotland who contribute to high quality data recording and provision.
References
Footnotes
Contributors HM, LW, CR and JCC designed the study. HM drafted the manuscript. All other authors contributed revisions and agreed with the final manuscript.
Competing interests None declared.
Ethics approval The investigation received approval from the NHS National Services Scotland Privacy Advisory Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All available data can be obtained by contacting the corresponding author.
Linked Articles
- Editorial
- Original article
- Original article
- Atoms