Article Text

Abstract
Despite the fall in numbers of unexpected infant deaths that followed the ‘Back to Sleep’ campaigns in the early 1990s in the UK and many other countries, such deaths remain one of the largest single groups of deaths in the postneonatal period in many Western countries. Changes in the ways in which unexpected infant deaths are categorised by pathologists and coroners, and increasing reluctance to use the term ‘sudden infant death syndrome’, make assessment of nationally and internationally collected data on incidence potentially inaccurate and confusing. In this paper, we review current understanding of the epidemiology and aetiology of unexpected deaths in infancy, and current hypotheses on the pathophysiology of the processes that may lead to death. We also review interventions that have been adopted, with variable degrees of effectiveness in efforts to reduce the numbers of deaths, and new approaches that offer the possibility of prevention in the future.
- Mortality
- SIDS
- Sleep
- Temp Regulation
- Respiratory
Statistics from Altmetric.com
Historical overview
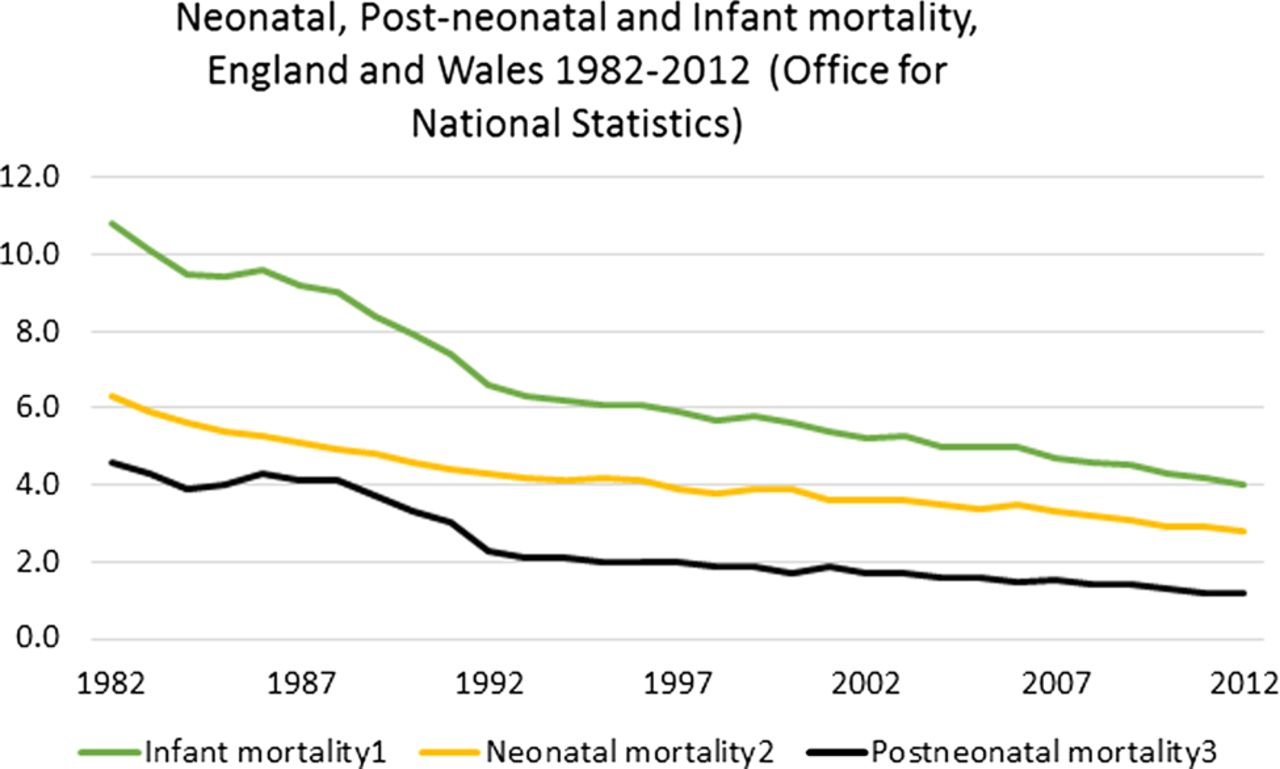
While sudden unexpected deaths of apparently healthy infants have been recognised since antiquity, such deaths did not form a focus of medical attention until the second half of the 20th century. The dramatic fall in infant mortality rates in the 20th century in England and Wales from 95 per thousand live births in 1912 to 10.8 in 1982 and to 4 per thousand live births in 2012 (see figure 1) meant that more attention was given to those deaths for which no sufficient explanation could be found. In the 1970s and 1980s, several studies showed an apparently increasing number of such deaths, and epidemiological studies in Europe and New Zealand showed an apparent association with the (relatively recently introduced) practice of putting infants down to sleep in a prone position.1 ,2 The dramatic reduction in the numbers of such deaths that followed attempts to dissuade parents from using the prone sleeping position for babies, in Avon County in England and in New Zealand, led to the widespread adoption of ‘Back to Sleep’ campaigns in many countries in the early 1990s, almost all of which were followed by substantial falls in the numbers of unexpected infant deaths, which was reflected in a marked fall in the overall infant mortality rate and the postneonatal mortality rate3 (see figure 1).

{kind=link}
Neonatal, postneonatal and infant mortality, England and Wales 1982–2012 (Office for National Statistics).
In the 20–25 years since the original 'Back to sleep' campaigns, the numbers of unexpected infant deaths have continued to fall in many countries, but the numbers of such deaths in certain high-risk groups have remained relatively constant.4 ,5 In particular, the numbers of deaths that occur in the most economically deprived groups have fallen much more slowly than in the less-deprived groups. The proportion of unexpected infant deaths that have occurred while sharing a sleep surface (‘co-sleeping’) with an adult has fallen more slowly than the deaths of infants sleeping alone in a cot.6 This has led some countries to advocate a complete ban on infants sharing a sleep surface with an adult.7 More recent evidence8 ,9 however suggests many of the co-sleeping deaths occur in hazardous environments (parents consuming alcohol, recreational drugs or using sofas) and emphasise the potential value of targeting these risk-taking behaviours rather than focusing only on co-sleeping.
Definition
The term sudden infant death syndrome (SIDS), originally proposed to describe those sudden and unexpected infant deaths for which no sufficient explanation could be found, has been criticised on the basis that there is little evidence that all such deaths arise from the same or similar mechanisms. The term SIDS represents a diagnosis by exclusion and thus is only valid if all appropriate investigations have been carried out to look for all known identifiable conditions that may lead to sudden and unexpected death. Studies in many societies over many decades have however shown certain characteristic recurring features of such deaths. The deaths are rare in the first week or two after birth, rise to a peak incidence between the second and fourth months and then decrease to become rare after 6 months of age. There is a characteristic excess of boys who constitute around 60% of the deaths. There is evidence that the peak age of occurrence and the previously marked winter peak of deaths have both decreased in the 20 years or so since the ‘Back to Sleep’ campaign2 ,4–6
With the caveat that the term SIDS’ represents a group of causes of death some of which will eventually be identifiable as specific medical conditions, it remains a useful term to describe those deaths for which no sufficient explanation can currently be given on the basis of clinical history, postmortem findings or investigation of the scene and circumstances of death. The use of the term 'unascertained' was accepted by the Kennedy Committee10 as being appropriate at the time of postmortem when insufficient information was available to attribute death to SIDS or another defined cause, but in the absence of a clearly defined and agreed meaning this term is less helpful as a final ‘cause’ of death at the conclusion of an inquest or infant death review process as it makes the collection of consistent National Data and thus assessment of trends over long periods of time more difficult. The Kennedy Report,10 the contents of which have been incorporated into the National guidance in England, emphasised the importance of detailed multiagency input into the assessment of the likely cause of all unexpected infant deaths, including where relevant the expertise of police, social care, primary care and paediatrics.
The term ‘positional asphyxia’ to describe the cause of death in infants found unexpectedly dead should only be used in the presence of specific findings to indicate external physical asphyxia.
In this paper, we will use the definition of SIDS proposed in 1991.11 This defines SIDS asThe sudden death of an infant under 1 year of age, which remains unexplained after a thorough case investigation, including performance of a complete autopsy, examination of the death scene and review of the clinical history.
A number of publications have described the necessary standards and specific content of the various investigations that must be included in order to meet the stringent requirements of this definition.11
The triple risk hypothesis: physiological vulnerability, developmental changes and environmental factors
In 1994, Kinney and Filiano12 proposed that unexpected infant deaths might arise as a consequence of the combination of three factors coming together:
a vulnerable infant
a vulnerable phase of development
a final insult occurring in this window of vulnerability.
This ‘triple risk’ hypothesis has been widely accepted and has proved valuable in helping to understand why particular infants may die at particular ages when exposed to potential stressors that they may have previously encountered without adverse effect.
Infants with underlying vulnerability include those born preterm or of low birth weight, those exposed to maternal smoking in utero and infants with certain metabolic abnormalities or common polymorphisms that may make them more vulnerable to certain environmental factors or infectious agents. As noted above, the marked male preponderance in SIDS victims may also represent an intrinsic vulnerability.4 ,13
The normal processes of development of thermal, respiratory and cardiovascular control may lead to periods of increased vulnerability to external stressors such as infection, thermal stress or the prone sleeping position.13 The relationship between respiratory control, normal developmental physiology and brainstem neurophysiology has been very clearly described by Garcia et al14 and is summarised below.
In a number of infants, physiological recordings have been made at the time of sudden unexpected collapse and death, and the characteristics of these recordings, which commonly show periods of worsening bradycardia with gasping before complete cessation of respiratory efforts, suggest a failure of arousal and autoresuscitation as a final event in these infants.15
Studies of infants who have subsequently died as SIDS have shown that some such infants have shown a lower frequency of sighs during sleep than age-matched control infants, suggesting the possibility of some underlying abnormality of respiratory control.16
Sighs, which are commonly triggered by a slight fall in blood oxygen saturation, are most frequent in newborn infants and decrease in frequency with increasing age and size.17 Under conditions of mild to moderate hypoxaemia, an increase in the frequency and magnitude of sighs is associated with cerebral cortical arousal, an important protective mechanism. Under conditions of progressive hypoxaemia, eupnoea gives way to gasping respiratory efforts, with progressive bradycardia and finally to apnoea or cessation of all respiratory efforts. Under normal conditions, the mechanism giving rise to the respiratory pattern is a consequence of the interactions of several interacting neural networks and is thus particularly resistant to failure, but in conditions of progressive or persisting hypoxaemia there is a reconfiguration of the relevant networks to a simpler but more vulnerable system. This less complex neural network is particularly dependent on the activity of serotonergic neurons in the brainstem. Recent animal studies have shown a transient developmental dependence on serotonergic neuromodulation to maintain respiratory rhythm in early postnatal life. A further important feature of the response to hypoxia is the occurrence of a period during the recovery phase from hypoxia in which there is relative inhibition of respiratory activity—this posthypoxic ventilator depression that follows gasping and precedes eupnoea may represent a further potentially vulnerable period, which if prolonged might increase the risk of resuscitation failure and thus of SIDS.14 ,15
The pre-Bötzinger complex, a bilateral network of neurons in the ventrolateral medulla, is responsible for both maintenance of normal breathing (eupnoea) and also the generation of sighs and gasping. It also has important effects on cardiorespiratory coupling, a crucial component of the autoresuscitation response to hypoxia. The generation of gasping within this complex is critically dependent upon serotonergic neurons.14
The critical importance of serotonergic neurons in these brainstem homeostatic mechanisms has been underscored by the consistent findings of abnormalities of brainstem serotonergic pathways in postmortem investigation of infants who have died as SIDS.14 ,18
Several potential mechanisms have been postulated by which the prone sleeping position might lead to increased risk of SIDS, including the possibility of rebreathing expired gases (leading to a potential rise in CO2 and a fall in oxygen saturation), increased arousal threshold and decreased heat loss leading both to possible thermal stress and to increased nasal temperature that in turn leads to increased growth of toxigenic bacteria.2 ,13 ,14 ,19
Increased environmental temperature may lead to decreased arterial oxygen saturation, increased arousal threshold and decreased gasping in hypoxic conditions.14 ,20
Increased growth of toxigenic bacteria, particularly in the presence of exposure to tobacco smoke, may be a significant contributory factor in some unexpected infant deaths, particularly of male infants.21
A number of polymorphisms have been identified at increased frequency in infants who have died as SIDS, including polymorphisms of hepatic glucose-6-phosphatase transporter, Aquaporin 4, tumour necrosis factor-alpha and proinflammatory cytokines. While the mechanisms by which these polymorphisms might lead to increased risk of SIDS are not known, all are known to have potentially significant effects on brainstem neurophysiology—mostly independent of serotonergic mechanisms.13 ,14 ,20 ,22
The study by Rubens, which reported that certain features of the routinely administered otoacoustic emissions hearing screening test might identify some infants at increased risk of SIDS in infants who passed the hearing screening test,23 has not yet been repeated, though others have shown that failing the hearing screening test was not a good marker for increased risk of SIDS.24 The potential significance of these findings has been highlighted by the observation in mice that damage to the vestibular nucleus has major effects on the control of breathing, with a loss of CO2 sensitivity.25
In several studies, a small but significant proportion of infants who die suddenly and unexpectedly have been shown on postmortem genetic testing to have cardiac channelopathies, conditions with considerable implications for surviving and future family members. This has led to the suggestion that such genetic testing should be performed as part of the routine postmortem investigation of all infants who die suddenly and unexpectedly.26
The epidemiology of unexpected infant deaths
The characteristic age distribution of unexpected infant deaths, with few during the first week, an increasing prevalence with age peaking between 2 and 4 months of age and few deaths occurring beyond the age of 6 months has been recognised for many years.4 As noted above, the peak age of incidence has decreased since the implementation of the ‘Back to Sleep’ campaign5 ,6 and the proportion of deaths in the first month has increased.
A number of environmental risk factors have been identified including the prone or side sleeping positions exposure to tobacco smoke before or after birth, and sleeping in hazardous circumstances, particularly those in which the head might become covered or the baby might become covered with excess bedding, especially at the time of acute viral infections.4 ,5 ,27 ,28
There is clearly an association, the nature of which is controversial, between co-sleeping and the risk of SIDS.4 ,7–9 In the great majority of instances when infants die while co-sleeping (sharing a sleep surface) with an adult, there is no direct evidence that death has arisen by any identifiable mechanism such as overlying and thus such deaths may be appropriately categorised as SIDS even though some concern may have arisen as to the role of the adult in causing or contributing to the death.
The question of whether the risk of SIDS is increased for an infant sharing a bed with a breastfeeding mother who does not smoke or take recreational drugs, who has not been drinking alcohol and who is aware of how to maintain a safe sleep environment for her baby remains unclear.
The 2014 National Institute for Health and Care Excellence (NICE) guidance on parents co-sleeping with infants recognised that co-sleeping may be intentional or unintentional, and concluded that while there is evidence of an association between co-sleeping and increased risk of SIDS the evidence was not sufficient to deduce a causal relationship. The guidance suggested that all parents should be made aware of this association, particularly for preterm of low birthweight infants and for parents who smoke, have been drinking alcohol or taking recreational drugs.29
Unfortunately, this guidance did not distinguish between co-sleeping in a bed and co-sleeping on a sofa or armchair, though in three major UK studies and one from Ireland sofa sharing has been found to significantly increase the risk of SIDS compared with bedsharing.4–6 ,30 ,31
Two recently published individual-level analyses using the data from large, population-based case–control studies have reached different conclusions. Carpenter et al9 concluded that even in the absence of maternal smoking or alcohol intake co-sleeping carried a significantly increased risk of SIDS. One limitation of this analysis is that for some of the studies included information was not collected on alcohol intake and data on alcohol intake were imputed for these studies by reference to those constituent studies in which this information was collected despite the fact that they were in different populations, with potentially very different patterns of alcohol use.32
A similar individual-level analysis from the two large English case–control studies, in both of which detailed information was collected about alcohol use,8 found a substantially increased risk of SIDS for infants sharing a sofa with a parent or sleeping anywhere with a parent who had consumed alcohol or was a smoker, but in the absence of these risk factors, bedsharing was not associated with an increased risk of SIDS. In this study, the incidence of breast feeding among the bedsharing families was similar between SIDS and controls, so the apparent protective effect of breast feeding was present only for infants who slept in cots. Similarly, the apparent protective effect from dummy use was present only among bedsharing infants.8
Given the very strong, bidirectional relationship between breast feeding and bedsharing33 and the undoubted benefits of breast feeding, which include a lower infant mortality rate even in Western societies,34 it is important that all mothers, and breastfeeding mothers in particular, are given accurate information on which to make decisions about whether or not to bedshare with their baby.
Reducing the risk of SIDS
Infants at increased risk
Several studies have shown that the risk of SIDS is significantly higher for boys than girls, for twins or higher-order multiple births, for third or subsequent children in a family, for infants born preterm or of low birth weight, for infants of mothers who smoked or took recreational drugs during pregnancy, for infants of young mothers and for infants of socioeconomically deprived mothers, particularly those without a supportive partner.4 These same characteristics define a group of infants at increased risk of a range of adverse outcomes in infancy and childhood, and are commonly used to target increased healthcare input by health visitors. A scoring system developed from data collected in the first two years of the Confidential Enquiry into Stillbirths and Deaths in Infancy study of Sudden and Unexpected Deaths in Infancy (CESDI SUDI) study and tested on the data collected in the third year4 showed that using a simple scoring system, including maternal age, parity, smoking and low socioeconomic status, we could identify approximately 40% of the infants who would subsequently die as SIDS, in 8% of the population. Although this allows identification of a high-risk group, the large size of the group identified makes this approach of limited value in targeting interventions to reduce the risk of SIDS.
Experience over more than three decades has shown that the use of infant monitoring of any type has made no difference to incidence of unexpected infants deaths, and in the CESDI study the use of such monitors was associated with a slightly increased risk of such deaths, suggesting that, despite being used primarily for infants at high risk, monitors did not reduce the risk of unexpected death.4
Circumstances of risk
Putting babies down to sleep in the prone or side positions, using excessive bedding or wrapping, using bedding that can ride up over the baby's head, and smoking in the vicinity of the baby all significantly increase the risk of SIDS and all have been targeted in public health risk reduction campaigns with measurable success in the UK and other countries. The dramatic fall in SIDS that followed ‘Back to Sleep’ campaigns in the UK and subsequently in many other countries reflects the effectiveness of avoiding the prone sleeping position (see figure 1). The adoption of the ‘feet to foot’ position for infants in cots was shown in the study of unexpected infant deaths in Southwest England5 to be associated with a significantly reduced risk of SIDS, and the same study showed that the creation of a ‘smoke-free zone’ around infants has become a much more common approach to reducing postnatal tobacco smoke exposure in recent years.
As noted above, the risk of SIDS is increased significantly for infants co-sleeping (sharing a sleep surface) with parents who smoke, have been drinking alcohol or taking recreational drugs, particularly for ex-preterm infants. The risk is also greatly increased for infants sharing a sofa or armchair to sleep with a parent regardless of other factors, and parents should be actively encouraged to avoid such co-sleeping.5–8
In a longitudinal study of bedsharing and breast feeding as part of the Avon Longitudinal Study of Parents and Children ALSPAC cohort study, we showed that bedsharing in early infancy was most common among well-educated, less-deprived families, in which smoking was less common and for whom the risk of SIDS was extremely low33 Such mothers are however the most likely to listen to healthcare advice, and if advised not to co-sleep may take this advice despite a lack of evidence that by so doing they will be helping to reduce the risk to their baby. In the ALSPAC study, we showed a close bidirectional relationship between breast feeding and bedsharing, thus stopping bedsharing for such families may have the unintended consequence of shortening the duration of breast feeding. A further unintended consequence is illustrated by a number of mothers in our population-based studies of unexpected infant deaths who were advised not to bedshare, so fed their infant on a sofa where they fell asleep and the infant died.5
UNICEF UK has adopted a constructive approach, acknowledging, as does the NICE guidance,29 that co-sleeping occurs either intentionally or unintentionally and targeting mothers who wish to breast feed their infant and giving advice on night-time infant feeding, including safe co-sleeping.35
Little is known about how mothers who do not breast feed their infant and those who smoke or drink alcohol make their decisions about whether and how to co-sleep with their baby. It is clear that high-profile antibedsharing campaigns used in the USA and some parts of the UK are ineffective for such families and may achieve the undesired consequence of making them less responsive to other, more evidence-based approaches to reducing the risk of SIDS. Such approaches are also inappropriate for families from those ethnic minority communities in which bedsharing is a culturally determined norm and SIDS is extremely uncommon.36
A number of current studies of infant care practices in high-risk populations are seeking to identify and understand these decision-making processes in order to develop approaches to promoting safe infant sleep arrangements in ways that are acceptable to this high-risk group.37
Targeted interventions: what works?
A number of attempts have been made to target families with infants at high risk of SIDS, with limited success, though recent studies in which interventions have been developed with input from the relevant target ethnic or socioeconomic group are more encouraging.37 In general in the UK, however, the mothers of the infants at highest risk remain hard to reach, largely because of a lack of information on how such mothers make their decisions about child care practices, and their resistance to the imposition by outsiders of ideas and practices that do not fit easily within their perceptions of how they wish to run their lives.
The development of appropriate, user-friendly approaches to identifying and promoting safe infant care practices in such high-risk groups remains an important objective for those seeking to avoid potentially preventable infant deaths.
Future prospects
If we were able to identify those infants who are at significantly increased risk of SIDS because of some physiological or metabolic abnormality, this would allow preventive strategies to be targeted to these infants. Currently, such infants cannot be identified reliably, and as noted above epidemiological risk factors are too crude in themselves to be used in this way, but a combination of physiological markers and epidemiological scoring might have some value. Current studies aimed at identifying physiological characteristics of infants at high risk of SIDS might offer such a prospect.
For now, ensuring all parents are made aware of and understand risk factors for SIDS and how to create a safe sleep environment for their infant remains the highest priority in strategies to prevent SIDS.
Recognising the difficulties inherent in getting these messages across to the high-risk population, it is important to consider the introduction of innovative targeted approaches to reaching and involving this target group.
While offering appropriate support to all bereaved families, we must also seek to understand the circumstances and events leading to the death and ensure that lessons learned are used to help prevent future deaths.
References
Footnotes
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.