Article Text

Abstract
Objectives Describe cases of female genital mutilation (FGM) presenting to consultant paediatricians and sexual assault referral centres (SARCs), including demographics, medical symptoms, examination findings and outcome.
Design The well-established epidemiological surveillance study performed through the British Paediatric Surveillance Unit included FGM on the monthly returns.
Setting All consultant paediatricians and relevant SARC leads across the UK and Ireland.
Patients Under 16 years old with FGM.
Interventions Data on cases from November 2015 to November 2017 and 12 months later meeting the case definition of FGM.
Main outcome measures Returns included 146 cases, 103 (71%) had confirmed FGM and 43 (29%) did not meet the case definition. There were none from Northern Ireland.
Results The mean reported age was 3 years. Using the WHO classification of FGM, 58% (n=60) had either type 1 or type 2, 8% (n=8) had type 3 and 21% (n=22) had type 4. 13% (n=13) of the cases were not classified and none had piercings or labiaplasty. The majority, 70% had FGM performed in Africa with others from Europe, Middle East and South-East Asia. There were few physical and mental health symptoms. Only one case resulted in a successful prosecution.
Conclusions There were low numbers of children presenting with FGM and in the 2 years there was only one prosecution. The findings may be consistent with attitude changes in FGM practising communities and those at risk should be protected and supported by culturally competent national policies
- epidemiology
- child abuse
Statistics from Altmetric.com
What is already known on this topic?
Estimated figures based on 2011 census data have been interpreted to mean that thousands of girls could be at risk of undergoing female genital mutilation (FGM).
Although illegal since 1985, the first conviction for FGM in the UK was in 2019.
This is the first study of presentations of paediatric cases in the UK and Republic of Ireland.
What this study adds?
The findings of 103 reported cases over a 2-year period is far less than expected from the estimates.
The possibility of the abandonment of the practice of FGM after migration to the UK must be considered.
Anti-FGM measures need to be proportionate to the empirical evidence.
Background
Female genital mutilation (FGM) is defined by the WHO as ‘all procedures that involve partial or total removal of the external female genitalia, or other injury to the female genital organs for non-medical reasons’.1 FGM is a harmful traditional practice carried out in many countries across Africa, Asia and the Middle East, that spans religious and ethnic groups.2 Representative data suggest at least 200 million women and girls worldwide have been subject to FGM.1 The practice is now internationally recognised as a violation of the rights of women and children, it has no known health benefits and can cause serious damage to physical and psychological health.
FGM was criminalised in the UK in 19853 and, since 2003, it has been illegal to take a child out of the country for the purpose of FGM.4 In 2015, the Serious Crime Act introduced provisions including an offence of failing to protect a girl from risk of FGM and a mandatory duty on healthcare professionals to report FGM in children under the age of 18 years.5 In January 2019, the first conviction for FGM in the UK took place at the Central Criminal Court in London.6
Currently, there is a lack of evidence regarding prevalence of paediatric FGM in the UK. A report estimating prevalence based on 2011 census data concluded there were 60 000 girls in England and Wales under age 14 years who were born to mothers with FGM, and a further 10 000 girls who may have had FGM before entry to the UK.7 These figures have been interpreted to mean that thousands of girls could be at risk of being cut.8
This study is the first of its kind to look at presentations of paediatric FGM across the UK and Ireland. The study aims to assess cases of FGM that presented to consultant paediatricians and to some sexual assault referral centres (SARCs), including the type of FGM (WHO classification), associated demographics, clinical presentations, medical symptoms, examination findings and clinical management.
Methods
This was an epidemiological surveillance study performed through the British Paediatric Surveillance Unit (BPSU). The BPSU is a well-established epidemiological surveillance system designed to study paediatric rare diseases, with an average monthly response rate of over 90% from consultant paediatricians.9 For this study, surveillance extended to SARCs who see children.
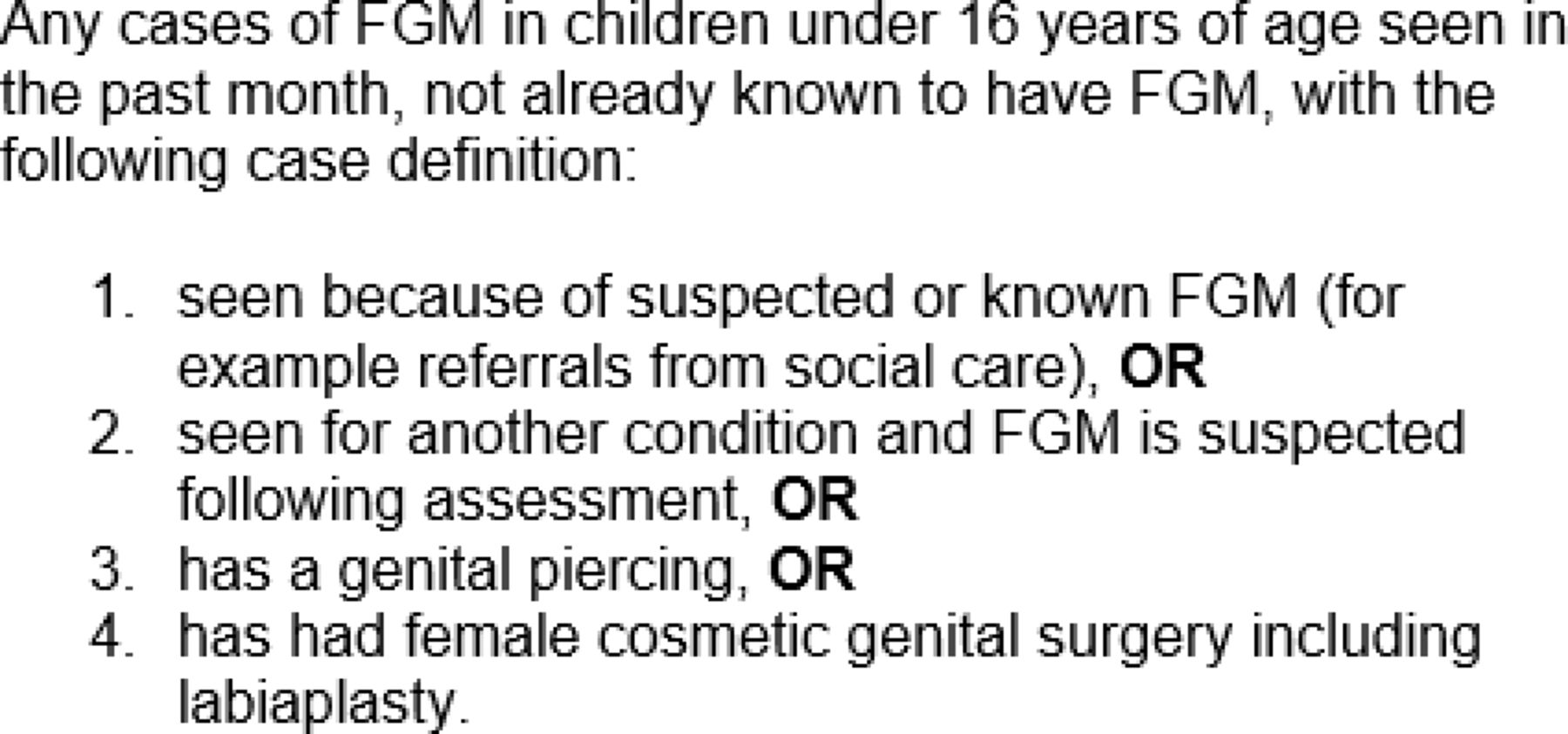
Following an application to the BPSU scientific committee, FGM was included on the BPSU surveillance card for the 25-month period between November 2015 and November 2017. The sponsor, the Royal College of Paediatrics and Child Health, undertook the management of day-to-day running of the project, data collection and analysis. All consultant paediatricians across the UK and Ireland, along with SARC leads, received the BPSU monthly e-card via an email link. Recipients reported any cases that fitted the case definition seen in the last month (figure 1) or reported if there were no cases seen. Following notification of a suspected case, the BPSU sent the reporting doctor a questionnaire via a secure on-line portal.

Surveillance case definition. FGM, female genital mutilation.
In any unclear cases, the study team reached a consensus on whether the case definition for FGM had been met. As far as possible, the clinical experts assigned a WHO classification of FGM (table 1) from anatomical descriptions provided. For the purposes of analysis, WHO type 1 and 2 were combined. Type 4 was defined as visual evidence of a scar on examination and/or verbal confirmation of FGM (being cut) by child or parent with normal examination. For confirmed cases, the team sent reporting doctors a follow-up questionnaire after 12 months focussing on health, social care and legal case outcomes of the case. Email and telephone reminders were used to optimise response rates, and respondents were reminded of their mandatory reporting duty.5 Anonymised data were exported to MS Excel for analysis.
Who classification of FGM1
The BPSU scientific committee independently reviewed the application. It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Results
For the period of surveillance, the e-card response rate was over 90% among consultant paediatricians, and 61% for SARCs.
During the study, the BPSU received 146 reports for suspected cases of FGM in the UK and Ireland. Of these cases, 8 were duplicates and 28 were excluded because they did not meet the case definition or were outside the reporting period. In a further seven cases the notifying doctor did not complete the initial forms and therefore there were insufficient data to include. Data are available for the remaining 103 cases of confirmed paediatric FGM. The SARCs identified 13 children with FGM who would not otherwise have been reported. Reports of FGM were received from across the UK (table 2).
Female genital mutilation (FGM) distribution of confirmed cases across the UK
Of the 103 confirmed cases, the mean reported age of FGM was 3 years (range 0–11 years) (figure 2), with 59 (57%) reported to have undergone FGM under the age of 5 years. The mean age of presentation to professionals was 10 years of age (range 2–16 years). The mean time from undergoing FGM to presentation was 6 years (range 0.5–15 years).

Age distribution at female genital mutilation (FGM) presentation (where data available, n=78).
From anatomical descriptions, 60 cases (58%) were classified as WHO type 1 or 2 FGM, 8 cases (8%) type 3 FGM and 22 cases (21%) as type 4 FGM (figure 3). The remaining 13% (n=13) of cases could not be assigned a WHO classification as the girls were not examined (case definition met through clear history of FGM). No cases of piercing or cosmetic genital surgery including labiaplasty were reported.

{kind=link}
{kind=link}
{kind=link}
WHO classification of female genital mutilation (FGM).
FGM was said to be most commonly performed in Sudan (n=25; 24%), Somalia (n=22; 21%), Gambia (n=19; 18%) and Eritrea (n=7; 7%) with smaller numbers from Europe (n=<5), the Middle East (n=<5) and South-East Asia (n=<5) (table 3).
Region where female genital mutilation (FGM) was said to have been done
Of those cases reported to have occurred in Sudan the majority (15/25; 60%) were performed at age 5 years and over, a significantly higher percentage for this age group than any other country. Of the 103 confirmed cases, 57% (n=59) of cases were performed on girls aged under 5 years and 27% (n=28) were performed on girls aged between 5 years and 11 years. In the majority of cases (n=74, 72%), FGM was performed in the country of birth and only one was reported as performed in the UK.
Where data on who performed FGM were available (n=58), 45% (26/58) were performed by health professionals, 36% (21/58) were performed by a ‘traditional circumciser’ and 12% (n=7) were performed by a relative.
In 22 cases (21%), there were 24 mental health symptoms that were considered attributable to FGM, with a small number of reports listing several symptoms for the same child. Specific mental health issues included anxiety including panic attacks, emotional and behavioural issues, and sleep disturbances, for example, nightmares. There were physical symptoms in a total of 13 cases and unspecified symptoms in 6 (table 4).
Physical health symptoms attributed to female genital mutilation (FGM)
In 91% (n=31) of the 34 cases where FGM was initially suspected due to a relative being known to have had FGM, the girl’s mother was reported to have had FGM. Where data were supplied (n=82), FGM was reported in 99% (n=81) of mothers and 78% (n=60) of siblings.
Longer-term outcomes and legal aspects
Of the 103 confirmed cases, the 12-month follow-up questionnaire was returned for 71 cases (69%). Four children in this group were offered deinfibulation but only one child was reported to have had the surgery. In nine cases, the police had initiated a criminal investigation and in four of these there was no further action. In the five remaining, there were no further details in two and in the remaining three, one case performed in the UK resulted in a successful prosecution, and the two were part of a wider investigation on child cruelty.
Discussion
This study is the first in the UK to identify the number of cases of FGM reported to or identified by consultant paediatricians and doctors working in the SARCs; as such it is a new contribution to the literature on paediatric FGM in the UK. Like most epidemiological studies ascertainment is dependent on the effectiveness of the reporting methods and cases may have be seen by these sources but for whatever reason not reported. Although BPSU return rates are good for paediatricians, other doctors in child health who might have seen these girls include non-consultant doctors working in community child health and others in gynaecology or genitourinary medicine clinics. As the return rate from SARCs was only 61%, some may have been missed through the non-responders. Hence the figure of 103 should be taken as a minimum. Children suffering immediate and long-term effects of FGM may not be brought for medical consultation. If children or families are asked about FGM, knowledge of the legal status may prevent an honest history being given and so could remain hidden.
The only similar prevalence study from a high-income country is that from the Australian Paediatric Surveillance Unit. They recruited paediatricians and other child health specialists who reported seeing 59 children aged under 18 years seen between 2009 and 2014. These low numbers are similar to our study, although the Australian study differed in that it took place earlier when there was less knowledge of the practice of FGM.10 The other available source of data from the UK is the FGM Enhanced Dataset, collected by NHS Digital. Hospital trusts and GP practices are required to submit data on all women and girls seen with FGM.11 NHS Digital shared their updated figures for the 25-month study period, during which they identified 100 children under 16 years of age with FGM. Data from both these sources suggest that very low numbers of girls are being identified with FGM, and that these numbers are significantly lower than rates proposed from estimates of girls at risk.7 Lack of governance approvals has yet to allow a comparison of the BPSU data with the FGM Enhanced Dataset to maximise ascertainment.
Experts in paediatric gynaecology and child sexual abuse from the study team classified the type of FGM from the anatomical description given in the questionnaire. It is known that the size and appearance of prepubertal female genital anatomy varies12 and there are reports of failures of paediatricians to accurately diagnose FGM based on the normal labia minora or majora.13 Many of the physicians had limited experience in FGM, making it a challenge to accurately distinguish between cut labia minora and normal small labia minora. Hence, the decision was made to group WHO type 1 and type 2 FGM together for the analysis.
As best practice is not to force genital examination, 13% could not be classified as an FGM type. Of those examined, 58% had either WHO type 1 or type 2 FGM. WHO type 3 FGM, also known as infibulation, was found in 8% of cases, which is close to the international prevalence data on the global proportion of type 3 FGM of approximately 10%.14
Type 4 was classified in 21% and there may be a global trend towards less mutilating types of FGM.14 In addition this type of FGM is associated with fewer complications15 as well as being harder to diagnose on examination. Thus, our data do not support the predominant narrative in the UK, that all FGM is easily identifiable on genital examination.16
In this study a small number (n=13, 13%) of cases was associated with complications that were attributed to FGM. We do not know whether all children were asked about complications, or whether the doctor, child or parent attributed the symptom to FGM. We are unable to state whether the physical or mental health symptoms are direct complications of FGM as no causal inference can be drawn from cross-sectional data, and the symptoms could have been misunderstood or under-reported in this cohort. However, these data suggest that the majority of children with FGM in the UK do not experience significant complications, and that complications are unlikely to be the reason that FGM presents to doctors. Since the 2003 Female Genital Mutilation Act, there have been only two identified cases of FGM in the UK and Republic of Ireland that have presented to the emergency department with acute bleeding requiring surgical intervention.6 17
This study shows that 25% (n=26) of cases were performed by a health professional or in a healthcare setting such as a clinic. This ‘medicalisation’ of FGM mirrors a global trend among practising communities,14 which may have arisen as a result of campaigns warning of medical consequences of FGM. Medicalisation could potentially reduce some complications of FGM, but has been shown to legitimise and prolong the practice in communities;14 ‘medicalised’ FGM is illegal in the countries of origin of patients in this study.
There was only one successful prosecution among cases in this study, even though nine cases were initially investigated for a possible prosecution. Due to the nature of the crime, where there may be insufficient evidence and unclear perpetrators,13 18 and the required burden of proof in an adversarial legal system, it is rare that cases are taken forward for potential prosecution. In addition, there is a possibility that parents lie about the country in which FGM took place given the threat of legal repercussions. There may be more chance of a successful prosecution in future, as the 2015 Serious Crime Act includes the offence of failing to protect a girl from risk of genital mutilation.5
The findings in this study, numbers from NHS digital and a recently published FGM clinic series19 all indicate very low numbers of girls with FGM being identified. This was an unexpected finding, as after the introduction of the much discussed Serious Crime Act in 2015, many expected that large numbers of illegal FGM would present to services. Several recent studies have found evidence that migrant communities are abandoning the practice of FGM,20–23 in part due to the work of activists and educators from within practising communities. Concern has been raised that estimates of FGM rates or risk to children derived from ethnicity of their mothers are inaccurate,24 and that attempts to estimate risk have been misrepresented.25 The low numbers identified in this study may indicate that there is very little FGM happening in the UK, although there remains the possibility that some FGM may be continuing on a hidden level. Measures to identify FGM in the UK need to be informed by available data; there is mounting evidence that anti-FGM approaches, including the push for prosecution, are considered by many to be disproportionate, ill-conceived and unnecessarily heavy-handed.13 22 24 26 27
Communities moving away from the practice of FGM may reflect the success of prevention programmes, although evidence for their efficacy is limited. One successful approach in Europe is the REPLACE (Researching Female Genital Mutilation Intervention Programmes Linked to African Communities in the EU) approach; the evaluation of the interventions developed and delivered by the five partners indicated that there had been a change in attitudes towards FGM.28
The findings point to a need for research on the attitudes to FGM among the communities in the diaspora in the UK, for example, by adding questions to existing anonymous national surveys, such at the Natsal Surveys.29 These could also be given to a cohort of young people over the age of 18 years from affected communities who may feel more able to give honest answers in an anonymous form.
Increased awareness of FGM as an issue is important but needs to be handled sensitively to avoid racial profiling of affected communities. We recommend that where children are taught about FGM this is considered within the wider framework of body integrity in the context of comprehensive personal, social and health education.
Conclusion
This epidemiological surveillance study identified a very low number of children with FGM in the UK, and these numbers are consistent with other sources of data. Most children in this study had had FGM performed prior to arrival in the UK, with only a few cases in British children. Where FGM was identified the majority was classified as WHO type 1 or 2 or 4, which can be difficult for doctors, even specialists, to identify, and was associated with few complications. There was only one criminal prosecution in the 2-year study period. These results are consistent with very little FGM happening in the UK, but do not exclude the possibility that paediatric FGM maybe continuing on a hidden level. In a recent statement from the Metropolitan Police, Inspector Allen Davis commented on the first criminal conviction in the UK, stating that this showed that ‘FGM is still happening across London and the U.K., behind a cloak of secrecy’ in ‘communities that can be quite closed’.30 However, to date there remains no empirical evidence for this effect. Anti-FGM measures should be proportionate to empirical evidence and weighed against the risk of negatively affecting communities from practising countries.
Acknowledgments
The authors thank the many paediatricians and doctors working in the SARCs who notified the BPSU and then spent time completing the questionnaires; without their help this study would not have been possible.
References
Footnotes
Twitter @doctornajette, @rareman4u
Contributors DH had the idea for the study and with AJA and RML designed the study. The BPSU Scientific Committee approved the application to run the study. KP, ML, WL, RML and NAO'D carried out the data analyses. DH, NAO'D, AJA, RML, KP, ML, WL and SMC reviewed the data. DH, NAO'D, AJA, RML, GD, WL, SMC wrote and finalised the manuscript.
Funding The RCPCH and North West London NHS Foundation Trust have been funded by the FGM Prevention Programme, Department of Health, reference number 7591.
Disclaimer The views and opinions expressed in this article are those of the authors and do not necessarily reflect those of the funder or the sponsor.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Confidentiality Advisory Group (CAG Ref: 15/CAG/0178) and Public Benefit and Benefit Privacy Panel (Ref 1516–0292). Ethics submission was made to the South East Scotland Research Ethics Service who stated that they didn’t consider the application 15/SS/0139 to be research and therefore the project does not require NHS ethical review.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.