Article Text

Abstract
Respiratory rate (RR) is a valuable early marker of illness in vulnerable infants, but current monitoring methods are unsuitable for sustained home use. We have demonstrated accurate measurement of RR from brief recordings of pulse oximeter plethysmogram (pleth) trace in full-term neonates in hospital. This study assessed the feasibility of this method in preterm infants during overnight recordings in the home. We collected simultaneous overnight SpO2, pleth and respiratory inductive plethysmography (RIP) on 24 preterm infants in the home. RR from pleth analysis was compared with RR from RIP bands; pleth quality was assessed by the presence of visible artefact. Median (range) RR from RIP and pleth were not significantly different at 42 (25–65) and 42 (25–64) breaths/min. Median (range) % of epochs rejected due to artefact was 20 (8–75) for pleth and 10 (3–53) for RIP. Our results suggest that home RR monitoring by pulse oximeter pleth signal is accurate and feasible.
- respiratory rate
- infant
- pulse oximetry
Statistics from Altmetric.com
What is already known?
Respiratory rate is a key vital sign in young children, and tachypnoea is an important early marker of a range of diseases.
Existing methods for recording respiratory rate, such as respiratory inductive plethysmography or nasal thermistor, are problematic for sustained home use.
The plethysmogram recorded by pulse oximeters contains respiratory data, which can be extracted by appropriate signal processing.
What this study adds?
Prolonged respiratory rate monitoring of preterm infants in the home is feasible using a pulse oximeter, with no additional sensors on the infant.
This technique has the potential to allow early identification of deterioration in selected vulnerable infants and young children.
Introduction
Elevated respiratory rate can be an early indicator of illness in infants and children. To compensate for impaired gas exchange, infants and young children increase minute volume predominantly by increasing respiratory rate to maintain blood oxygenation. Tachypnoea in infants is an early and consistent marker of a number of acute conditions including infection1 and can also be the presenting sign in a wide variety of congenital respiratory, cardiac and neurological disorders.2 Thus, respiratory rate is a key measurement for sick and vulnerable infants and children,1 ,2 and monitoring it could help in early identification and treatment of disease. However, at present, monitoring respiration requires the use of sensors such as effort bands or nasal thermistor, which are problematic for regular clinical use.
Infants born preterm, especially those who develop chronic lung disease of prematurity, remain vulnerable after discharge from hospital and are an example of a group in whom respiratory rate monitoring could be helpful. Pulse oximetry is already widely used in these infants for monitoring of oxygen saturation (SpO2) and heart rate in the home, and placement of a pulse oximeter sensor on a limb is well tolerated by infants.
Pulse oximeters produce a plethysmogram (pleth) trace reflecting the instantaneous volume of blood in the extremity under the probe, and this pleth trace is affected by changes in respiratory effort.3 Low-pass filtering can be used to remove the dominant heart rate component and yield a trace containing only the lower frequency components. Using this method, we have previously derived respiratory data from short segments of the pulse oximeter pleth trace in healthy newborn infants3 and for longer periods in infants undergoing investigation in hospital for sleep-disordered breathing.4 The feasibility of this technique for prolonged infant home recordings has not previously been established.
Aim
The aim of this study was to examine if respiratory rate can be derived from home pleth recordings in infants born prematurely. Specifically, we wished to establish, in this clinical setting (1) whether respiratory rate measurement is accurate with reference to a standard method (respiratory inductive plethysmography, RIP) and (2) whether respiratory rate can be monitored for a useful proportion of the duration of recordings.
Method
The study was approved by the NRES Ethics Committee West Midlands—Edgbaston. A Nonin pulse oximeter module and sensor (Nonin Medical, USA) was used to record a continuous pleth trace, oxygen saturation and pulse rate in two groups of infants born at <37 weeks gestation. One group was healthy preterm infants with no current respiratory disease, and the second group was preterm infants who subsequently developed chronic lung disease (CLD) of prematurity, defined as persisting oxygen requirement at 28 days of age. Simultaneously, respiratory movements were recorded using thoracic and abdominal RIP bands, and both RIP and pulse oximetry data were recorded on a SOMNOscreen plus multichannel recorder (SOMNOmedics GmbH, Germany).
Parents applied equipment in the home after instruction in hospital. The pulse oximeter probe was placed on the foot under clothing and bedding to minimise the possible movement-related artefact, and recordings were made during natural overnight sleep.
Pleth traces were low-pass filtered (LPF) to extract respiratory data employing a similar technique to that of previously described3 ,4 using software we developed with MATLAB (The MathWorks, Natick, Massachusetts, USA). The LPF cut-off frequency was at half the 90th percentile pulse rate calculated in sequential epochs of length 2 min; the filter characteristics give a steep roll-off to remove the pulse rate component. The data recorded were visually reviewed using a signal viewer in 1 min sections. Respiratory rate was computed in sections with little or no artefact of the LPF pleth and RIP traces. In all but one case, the LPF pleth trace was compared with the abdominal RIP band; in one case, the abdominal band did not record so the thoracic band was used for comparison.
To evaluate how sensitive the two techniques are to artefact, the first hour after the traces had settled was assessed in the 21 analysed recordings. The proportions of 60-s epochs with over 10 s of artefact for the LPF pleth data and separately for the RIP band data were evaluated by visual examination.
Data were tested for consistency with a normal distribution using the Ryan–Joiner test in Minitab v16 (Minitab, USA) and analysed using parametric or non-parametric tests as appropriate.
Results
Home recordings were analysed from 21 preterm born infants. Three other recordings were not analysed because of technical problems: no RIP band trace in one, no pulse rate and SpO2 data in another and no pleth trace in the third. Nine of the 21 analysed recordings were from infants with CLD, and seven of the nine CLD infants were receiving supplemental oxygen at the time of the home recording. Twelve of the 21 recordings were from infants who were born prematurely but had no respiratory or other medical compromise (healthy preterm group).
Table 1 summarises the descriptive data for all infants and the respiratory rate measurements using the two methods. As expected, the gestation and weight at birth of the healthy preterm infants were greater than the CLD preterm infants. However, at the time of recording, the postnatal ages and weights were comparable.
Gestation, age and weight details of infants in the study together with respiratory rate derived from pleth traces compared with respiratory inductive plethysmography (RIP) band recordings
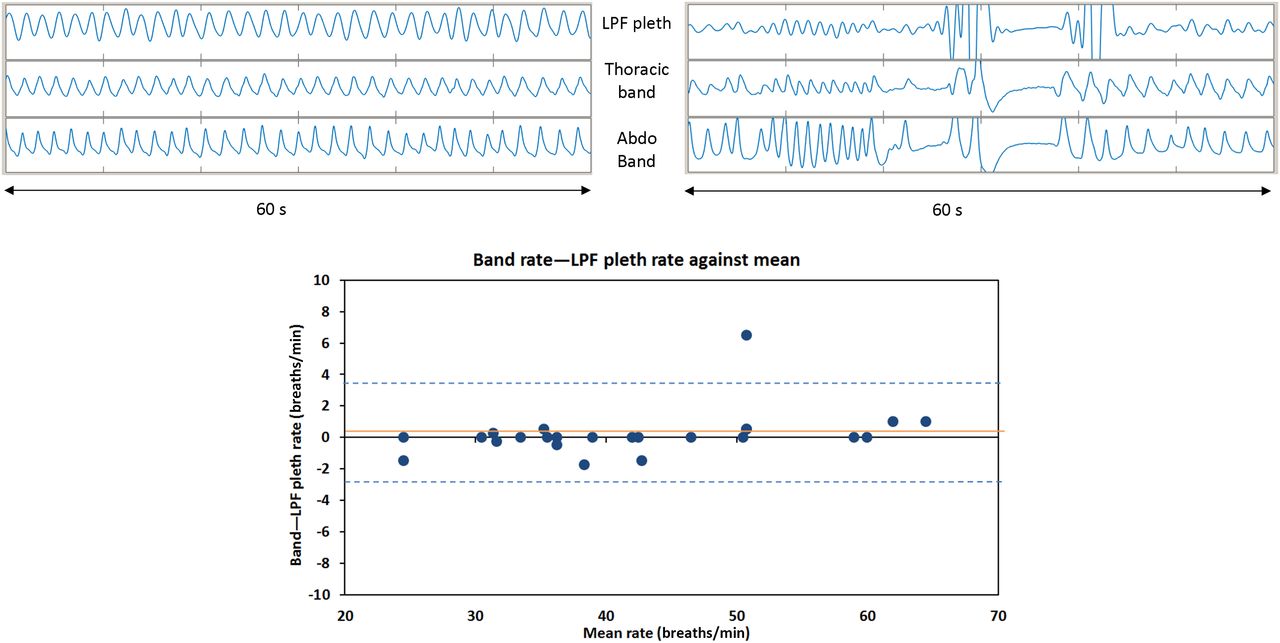
Overall, the respiratory rate from bands was median (range) 42 (25–65) breaths/min. Respiratory rate and pattern from LPF pleth trace were similar to bands (figure 1 shows two examples) with median (range) 42 (25–64) breaths/min (table 1). The median difference (RIP-pleth difference) was 0 and range −1.75–6.5 breaths/min (figure 1, lower graph), the Bland-Altman plot indicating no difference in accuracy at higher rates.

{kind=link}
Upper graph: examples of two 60 s sections from a recording: filtered pleth (top), thoracic band (middle) and abdominal band (bottom trace). The left-hand example shows regular respiration, whereas the right-hand section is an example showing variable respiratory rate and short apnoeas. Lower graph: Bland–Altman plot of respiratory rate from respiratory inductive plethysmography (RIP) bands compared with filtered pleth (bands minus low-pass filtered (LPF) pleth vs mean of bands and LPF pleth). The mean (SD) difference is 0.3 (1.56) breaths/min. The orange solid line indicates the mean; dashed blue lines indicate mean+2SD.
For recordings on 21 infants, the median (range) % of epochs rejected due to artefact was 20 (8–75) for pleth and 10 (3–53) for RIP. Those recordings with lower levels of band artefacts tended to have lower pleth artefact; there was a relation between the percentage of epochs rejected for pleth and RIP band data (Spearman's rank correlation coefficient r=0.88, p<0.001).
Discussion
Our results demonstrate that respiratory rate can be derived accurately from good quality pleth home recordings in infants. Although more epochs were affected by artefact on the pleth than on band recordings, overall 80% of 1-min pleth epochs had no or minimal artefact. This method may thus enable near-continuous additional respiratory rate and rhythm to be derived using standard oximetry sensors.
Visual counting of respiration rate is problematic: the precise method used, duration of counting and state of arousal all influence the value obtained.5 In selected vulnerable infants and young children, respiratory rate data and trends recorded in the home, using the technique we have developed, could allow early identification of tachypnoea and of pathological respiratory patterns.4 In oxygen-dependent infants already undergoing intermittent overnight assessment of saturation and heart rate, respiratory rate would add additional clinical value and may flag up infants not yet ready to ‘wean’. In the future, continuous home monitoring of these parameters in very high-risk infants is a possibility.
Acknowledgments
This research was commissioned by the National Institute for Health Research (NIHR)—RfPB grant PB-PG-0610-22433. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Footnotes
Twitter Follow David Wertheim at @DWertheim
Contributors PS: literature search, study design, data interpretation, writing and review of manuscript. SS-K: study design, data collection, writing and review of manuscript. DW: literature search, study design, data analysis and interpretation, writing and review of manuscript.
Funding National Institute for Health Research (PB-PG-0610-22433).
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Ethics approval NRES Committee West Midlands—Edgbaston.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The following additional data are available to researchers on request: additional clinical data on the infants recruited and more detailed data on respiratory rate, heart rate and oxygen saturation during the studies.