Article Text

Abstract
Aim To investigate the epidemiology, clinical profile and risk factors of pseudotumor cerebri syndrome (PTCS) in children aged 1–16 years.
Methods A national prospective population-based cohort study over 25 months. Newly diagnosed PTCS cases notified via British Paediatric Surveillance Unit were ascertained using classical diagnostic criteria and categorised according to 2013 revised diagnostic criteria. We derived national age, sex and weight-specific annual incidence rates and assessed effects of sex and weight categories.
Results We identified 185 PTCS cases of which 166 also fulfilled revised diagnostic criteria. The national annual incidence (95% CI) of PTCS in children aged 1–16 years was 0.71 (0.57 to 0.87) per 100 000 population increasing with age and weight to 4.18 and 10.7 per 100 000 in obese boys and girls aged 12–15 years, respectively. Incidence rates under 7 years were similar in both sexes. From 7 years onwards, the incidence in girls was double that in boys, but only in overweight (including obese) children. In children aged 12–15 years, an estimated 82% of the incidence of PTCS was attributable to obesity. Two subgroups of PTCS were apparent: 168 (91%) cases aged from 7 years frequently presented on medication and with headache and were predominantly female and obese. The remaining 17 (9%) cases under 7 years often lacked these risk factors and commonly presented with paralytic squint.
Conclusions This uniquely large population-based study of childhood PTCS will inform the design of future intervention studies. It suggests that weight reduction is central to the prevention of PTCS.
- pseudotumor cerebri
- idiopathic intracranial hypertension
- Obesity
- Epidemiology
- BPSU
Statistics from Altmetric.com
What is already known?
Pseudotumor cerebri syndrome (PTCS) is a rare syndrome of intracranial hypertension defined by an evolving diagnostic algorithm, most recently revised in 2013.
Risk factors for PTCS include female sex and obesity.
The epidemiology of PTCS in childhood has not been reliably established in a prospective study but is thought to be lower than that in adults.
What this study adds?
This prospective survey of all cases in Great Britain and Ireland is the largest study of pseudotumour cerebri syndrome (PTCS) in childhood and establishes, for the first time, reliable estimates of age-specific, sex-specific and weight-specific annual incidence rates.
In a few, childhood PTCS occurs before the age of 7 years, often without identifiable risk factors and with some distinctive features in its clinical presentation.
Most childhood PTCS occurs from the age of 7 years when it is twice as common in girls and progressively commoner with increasing age and degrees of overweight. More than 80% of PTCS cases aged 12–15 years are attributable to obesity.
Introduction
Pseudotumor cerebri syndrome (PTCS), also known as idiopathic intracranial hypertension, is a rare syndrome of raised intracranial pressure (ICP) first described in 1893.1 Its annual incidence in adults and children has been estimated to be 1.6–2.22–4 and 0.5–0.95–7 per 100 000, respectively, although the latter estimates are based on small or retrospective studies. PTCS has potentially serious morbidities of distressing headache, blindness8 ,9 and complications of invasive treatment procedures. Its management remains controversial.
Classical diagnostic criteria for PTCS, in use since 1937,10 combine the absence of other causes of raised ICP, including mass lesions and cerebral venous sinus thrombosis (CVST), with the presence of three cardinal features: symptoms of raised ICP, papilloedema and elevated opening cerebrospinal fluid (CSF) pressure at lumbar puncture (LP).11 These criteria provided the present study case definition (table 1A). Although CVST excludes the diagnosis of PTCS, the presence of risk factors does not and it is therefore not ‘idiopathic’. The fidelity of the clinical diagnosis of PTCS may be reduced first by misdiagnosis of papilloedema when evaluated by clinicians lacking access to specialist ophthalmological assessment12 and second by the estimation of CSF pressure based on brief recording of lumbar CSF opening pressure. This varies with posture, movement, emotion, anaesthetics and hypercapnia, and may not accurately reflect mean CSF pressure.13
Diagnostic criteria for pseudotumor cerebri syndrome in children
An increase in the upper normal threshold of lumbar CSF opening pressure from 20 to 25 cm CSF in non-obese children and 28 cm in children who are either obese or sedated for their LP has been proposed.14 Furthermore, specific (but insensitive) neuroradiological markers of raised ICP have been established.15–19 In 2013, Friedman et al 20 published revised diagnostic criteria for PTCS that incorporated these changes, but did not include symptoms of raised ICP (table 1B). The revised criteria categorise PTCS as ‘definite’ (elevated CSF pressure and either papilloedema or abducens nerve palsy), ‘probable’ (papilloedema but normal CSF pressure) or ‘suggestive of PTCS’ (lacking papilloedema and abducens nerve palsy but manifesting elevated CSF pressure plus at least three valid neuroimaging markers of raised ICP).20
This study aimed to establish the incidence of childhood PTCS reliably, quantify the impact of known risk factors and identify clinical subgroups.
Methods
We ascertained newly diagnosed PTCS cases aged 1–16 years presenting over a 25-month period (August 2007 to October 2009) to general or specialised paediatricians in the UK or Ireland using the monthly reporting scheme of the British Paediatric Surveillance Unit (BPSU).21 Notifying clinicians completed questionnaires detailing demographics, referral source, presentation, prior medications and medical conditions, and anthropometric, ophthalmological, CSF and neuroimaging data. Y-YM assessed jointly with at least one coauthor whether the submitted data fulfilled the study case definition (table 1A). The validity of the diagnosis was checked with the notifying clinician 1 year after diagnosis. Data collection concluded in July 2013. Each valid PTCS case was then categorised according to the subsequently published revised diagnostic criteria (table 1B).
CSF opening pressure reported above a recorded value was rounded up to the nearest integer (eg, ‘>40 cm’ became ‘41 cm’). The age-specific and sex-specific annual incidences for eligible PTCS cases were determined from contemporary population estimates22 ,23 and evaluated in three age categories: 1–6, 7–11 and 12–16 years. The choice of these three age categories was based on previous reports of variation of incidence rates with age and puberty status. Age-specific incidences for each year of age within each age band did not differ significantly from each other (data not shown).
Participants' growth data were expressed as z-scores of body mass index (or weight, when height was unavailable) in three weight categories: non-overweight (z-score <1.04=<85th percentile), overweight (excluding obese) (z-score ≥1.04 to <1.64=≥85th to <95th percentile) and obese (z-score ≥1.64=≥95th percentile), relative to the sex-specific and age-specific 1996 British Growth reference population.24 The weight-specific annual incidence of PTCS cases aged 4–6, 7–11 and 12–15 years was derived relative to the prevalence of these weight categories in national health surveys that were available for those age ranges.25 The UK and Ireland population aged 1–16 years during the survey was 12 451 742 of which 6 375 886 were male. The population aged 4–15 years included 1 604 499 males among 3 003 247 overweight children. Age-specific, sex-specific and weight-specific annual incidence rates were calculated with 95% CIs based on the Poisson distribution.
Continuous data were summarised as median values with IQRs and categorical data as n (%). Homogeneity of variance was assessed with the Levene's F-test. Case-wise deletion was performed for missing data. Groups were compared by Mann-Whitney U or Kruskal-Wallis tests and Fisher's exact test for continuous and categorical data, respectively. The impact of the known risk factors for PTCS was expressed as relative risk (RR), population attributable risk (PAR) and percentage PAR (%PAR). IBM SPSS Statistics 21 was used with two-tailed statistical testing at p<0.05.
This study was approved by the East London & The City Research Ethics Committee, the Patient Information Advisory Group and the North Wales NHS Research & Development.
Results
Of 379 notifications, 185 (49%) fulfilled the study case definition for newly diagnosed PTCS (figure 1). Of these, 124/185 (67%) were girls, 167/185 (90%) were of white ethnicity and 157/185 (85%) were directly referred to general paediatricians. The mean case accrual rate and percentage of cases relative to total notifications for each 6-month period remained steady throughout the 25-month survey at 46 (range 44–48) cases and 50% (range 42–57), respectively. The diagnosis remained valid in all 163/185 (88%) eligible cases for whom 1-year follow-up data were available (figure 1).
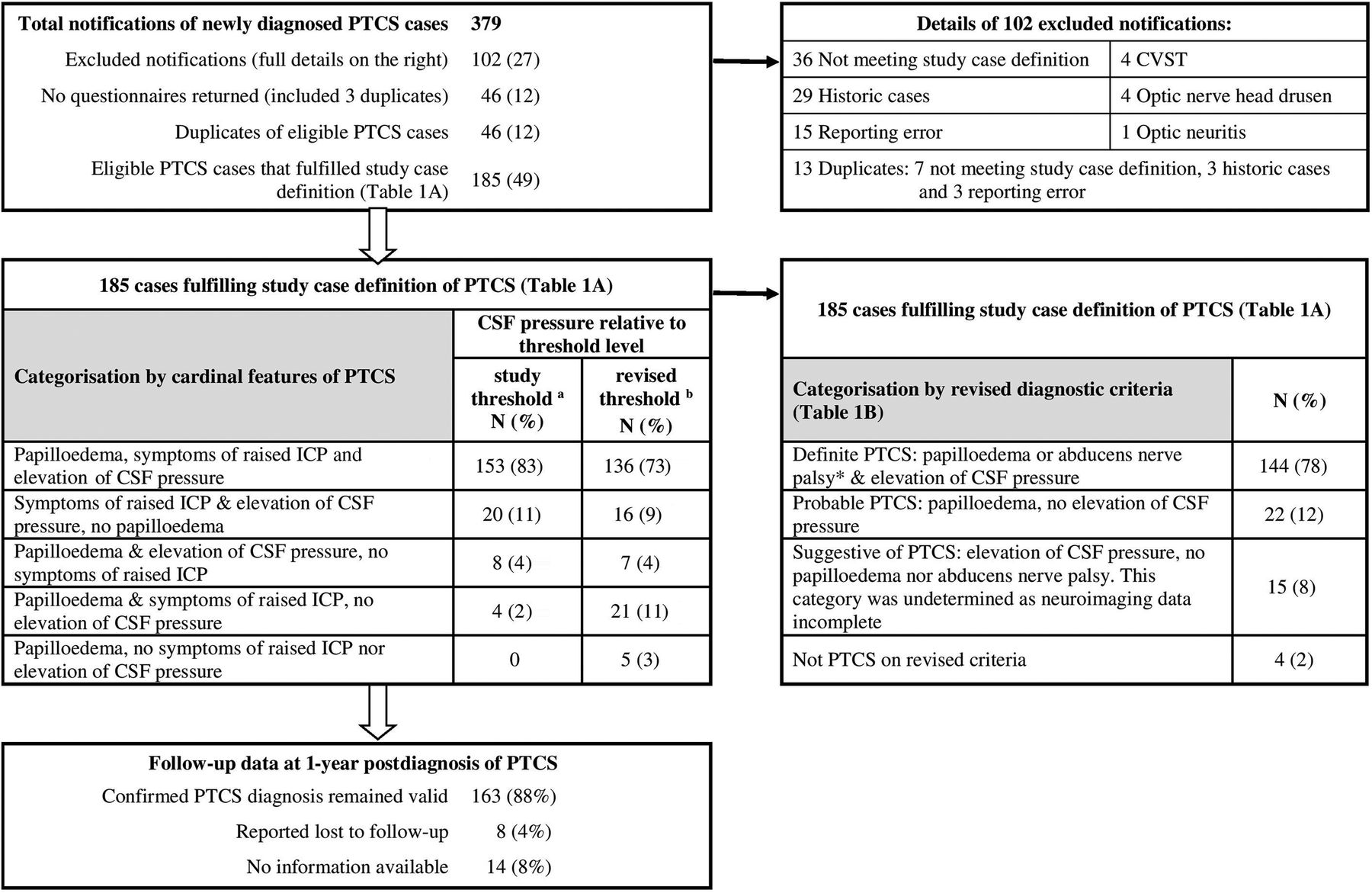
Notifications and cases fulfilling diagnostic criteria for pseudotumor cerebri syndrome (PTCS). CVST, Cerebral Venous Sinus Thrombosis. a>20 cm of cerebrospinal fluid (CSF).11 b ≥25 cm CSF in non-obese and unsedated child; ≥28 cm CSF if obese and/or sedated for lumbar puncture.14 *One definite PTCS case without papilloedema had abducens nerve palsy and elevated CSF pressure. ICP, intracranial pressure.
Incidence by age, sex and weight categories
The annual incidence of PTCS cases (95% CI) aged 1–16 years was 0.71 (0.57 to 0.87) per 100 000 population. The age-specific incidence increased from 0.17 to 0.75 and then to 1.32 per 100 000 in population aged 1–6, 7–11 and 12–16 years, respectively (see online supplementary appendix figure e1). Incidence rates in girls versus boys were 0.19 and 0.16, 1.06 and 0.46 and 1.85 and 0.82 per 100 000 in these respective age categories (see online supplementary appendix figure e1). Annual incidence per 100 000 obese population increased from 0.45 to 1.24 and then to 4.18 with age in boys aged 4–6, 7–11 and 12–15 years and from 0.56 to 3.44 and then to 10.7 in girls (see online supplementary appendix figure e1). The incidence remained low at 0.18–0.42 per 100 000 among non-overweight boys and girls throughout the age range of 4–15 years (see online supplementary appendix figure e1).
supplementary data
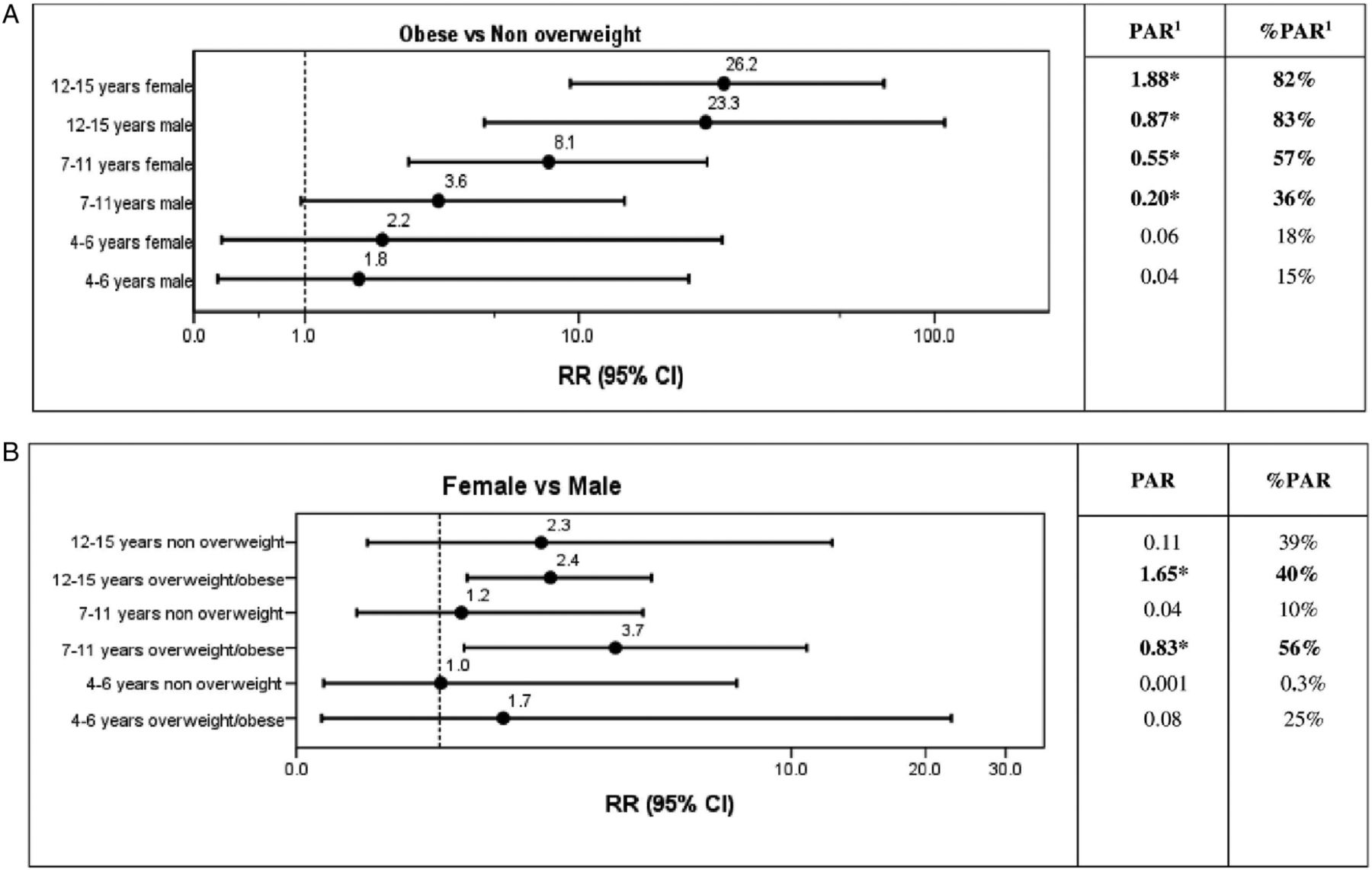
Weight and height measurements were available in 100% and 94% of cases, respectively. Twenty-one (11%) cases were overweight and 120/185 (65%) were obese (figure 2). In both sexes, the percentage of obese cases increased significantly with age (p<0.01) across the age categories from 41% (7/17) to 50% (29/58) and then to 76% (84/110) (p<0.001). The RR of PTCS associated with obesity relative to non-overweight children of the same age and sex was 3.6 and 8.1 in boys and girls aged 7–11 years, respectively, and 23.3 and 26.2 in boys and girls aged 12–15 years, respectively (figure 3). Among overweight (including obese) children, the RR for PTCS in girls relative to boys was 3.7 in those aged 7–11 years and 2.4 in those aged 12–15 years (figure 3).

Number of cases of pseudotumor cerebri syndrome (PTCS) by age, sex and weight categories. Non-overweight: body mass index (BMI) or weight z-score <1.04=<85th percentile. Overweight: BMI or weight z-score ≥1.04 to <1.64=≥85th to <95th percentile. Obese: BMI or weight z-score ≥1.64=≥95th percentile.

Risk of pseudotumor cerebri syndrome (PTCS) associated with obesity and female sex by age. PAR, population attributable risk; RR, relative risk; error bar, 95% CI. *The observed RR is statistically significant, that is, 95% CI does not include unity. (A) Association between obesity and incidence of PTCS by sex and age categories. RR of PTCS in obese versus non-overweight children is the ratio of the annual PTCS incidences in obese and non-overweight children, adjusted for age and sex categories. PAR of obesity=annual PTCS incidences in obese and non-overweight children—annual PTCS incidence in non-overweight children. Percentage PAR (%PAR) of obesity=(PAR of obesity×100)/annual PTCS incidence in obese and non-overweight children. (B) Association between female sex and incidence of PTCS by age and weight categories. RR in girls versus boys is the ratio of annual PTCS incidence rates in girls and boys, adjusted for age and weight categories. PAR of female sex=annual PTCS incidence in all child population—annual PTCS incidence in boys. %PAR of female sex=(PAR of female sex×100)/annual PTCS incidence of the total child population.
Key diagnostic and neurological features
The triad of raised ICP symptoms, papilloedema and elevated CSF pressure was seen in 83% (153/185) and 73% (136/185) of those using the study and higher revised14 CSF pressure threshold criteria, respectively (figure 1). Papilloedema, symptoms of raised ICP and elevated CSF pressure were absent in 11% (20/185), 4% (8/185) and 2% (4/185), respectively or, using the revised CSF pressure threshold,14 9% (16/185), 4% (7/185) and 11% (21/185) of cases (figure 1). There were no differences between cases with and without any one of the three diagnostic cardinal features with respect to other presenting features, such as sex, age and weight categories or other risk factors.
Headache was present in 161/185 (87%) cases. Diplopia, blurring of vision or transient visual loss were reported in 87/161 (54%) cases with headache and 15/24 (62%) cases without headache. One or more other neurological features were reported in 70/185 (38%) cases (32 abducens nerve palsy, 19 new presentation of squint, 17 dizziness, 12 photophobia, 8 neck stiffness/pain, 5 ataxia/falling, 4 tinnitus, 3 vertigo, 2 each of facial weakness, torticollis, nystagmus, vertigo, paraesthesia and pain behind eyes).
Papilloedema was reported in 165/185 (89%), was unilateral in 13/185 (7%) and was detected incidentally in 5/185 (3%) asymptomatic cases. Ophthalmologists confirmed its presence in all but five cases and also affirmed its absence in the 20/185 (11%) cases without papilloedema. Optic nerve head drusen (ONHD) was coexistent with papilloedema in 8/185 (4%), absent in 134/185 (72%) and uncertain in 27/185 (15%) cases. Of 32/185 (17%) cases with abducens nerve palsy, 30/32 (94%) were accompanied by papilloedema.
New presentation of decreased visual acuity (DVA) and/or restricted visual fields (RVF) at diagnosis was reported in 61/185 (33%) of the 182/185 (98%) cases whose vision was assessed. Seventeen had DVA, 32 RVF, 11 both DVA and RVF and 1 had unspecified visual defects. Of those with a visual deficit, 54/61 (89%) had papilloedema. No differences were detected in the proportion of visual deficit between sexes, age or weight categories.
Comparison of cases fulfilling study and revised diagnostic criteria
Of the 185 valid study cases, PTCS diagnosis was classified on revised criteria as ‘definite’ in 144 (78%) cases, ‘probable’ in 22 (12%) cases, not present in 4 (2%) cases and ‘undetermined’ in 15 (8%) cases in whom the presence (or not) of neuroimaging criteria required for the ‘suggestive of PTCS’ category had not been assessed (figure 1). The 166 ‘definite’ or ‘probable’ PTCS cases did not differ from the other 19 cases with respect to age, sex, weight categories, other associations or clinical features other than papilloedema.
Relation of neurological features to age and weight
The report of headache increased from 41% (7/17) of those aged 1–6 years to 91% (53/58) of those aged 7–11 years and stabilised at 90% (99/110) of those aged 12–15 years (p<0.001, figure 4). The incidence of blurring of vision also increased across these age categories from 24% (4/17) to 28% (16/58) then to 53% (58/110) (p=0.002, figure 4). Conversely, there was a reduction in paralytic squint with successive age categories from 29% (5/17) to 9% (5/58) then to 8% (9/110), respectively (p=0.024) and of transient visual loss from 35% (6/17) to 10% (6/58) then to 9% (10/110), respectively (p=0.007) (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Number and percentage of neurological features and risk factors of childhood pseudotumor cerebri by age category. *p<0.05.
Risk factors for PTCS and their relationship with age and sex
Ninety-three (50%) cases had one and 61 (33%) had more than one recognised risk factor at diagnosis (see online supplementary appendix table e1). Overweight or obesity was the only risk factor in 87/185 (47%) and was accompanied by other risk factors in 54/185 (29%) cases (see online supplementary appendix table e1). Among 46/185 (25%) cases on medication, 16 (9%) had a medical condition and girls were overrepresented (40/124 or 32% vs 6/61 or 10%, p=0.001). A further 21(11%) cases had a medical condition without associated medication. The commonest reported medical conditions were migraine in 18/185 (10%), and antibiotic use for acne in 10/185 (5%). The percentage of cases with risk factors increased with successive age categories from 59% (10/17) to 76% (44/58) then to 91% (100/110) (p=0.001).
Neuroimaging and CSF findings
All cases had cranial neuroimaging, and this included venography in 111/185 (60%) cases. Those with and without venography did not differ with respect to age, sex, weight, clinical features or other risk factors. At least one neuroimaging criteria of raised ICP20 (table 1B) was reported in 10/185 (5%) cases, all of whom had papilloedema but four lacked elevated CSF pressure on revised criteria.
The median CSF opening pressure was 35.5 cm CSF (range 12.0–74.0). It did not differ significantly between sexes or age categories, cases with and without headache or with and without papilloedema but was significantly higher in obese than other weight categories cases (p=0.004) and in the 82 cases whose LPs were undertaken with general anaesthesia (GA) compared with the 100 cases undertaken without GA (p=0.001) (see online supplementary appendix figure e2). However, the percentage of cases whose LP required GA did not differ between weight categories.
Discussion
This is the largest study of childhood PTCS to date and shows that the incidence increases eightfold from that in 1–6 years to that in 12–16 years and the numbers of girls and boys changes from being equal under the age of 7 years to two girls for each boy thereafter. These shifts were linked to obesity accounted for over four-fifths of the increased incidence among those aged 12–15 years. Even with the upwardly revised CSF pressure threshold,14 nearly three-quarter of cases had a classic triad of raised ICP symptoms, papilloedema and elevated CSF pressure and the clinical profile did not differ in other ways between cases with and without any one of the three cardinal features.
On revised diagnostic criteria,20 90% of cases captured by the study definition were classified as ‘definite’ or ‘probable’ PTCS and did not differ clinically from the remaining 10% except in manifesting papilloedema. This is consistent with PTCS being a single entity that includes either papilloedema or elevated CSF pressure or both. While PTCS is thus distinct, the findings on magnetic resonance venography and CSF haemodynamics are similar to those in the ‘slit ventricle syndrome’ of elevated CSF pressure.26 Slit ventricle syndrome is defined in patients with symptoms of raised ICP due to intraventricular shunt malfunction with slit-like radiological appearance of small ventricles. This usually arises when intermittent and functional shunt obstruction is associated with decreased compliance of the tissues surrounding the cerebral ventricles.
Although 90% were of white ethnicity, PTCS cases were reported in all ethnic groups. We believe this truly represents our nationwide paediatric practice. A smaller series of cases in California found similar relationships to those seen in this study between age, sex and overweight, and observed a significant increase in the risk of PTCS higher in non-Hispanic white children relative to that in Hispanic white or Asian/Pacific Island children.27
Cases younger than 7 years of age were less likely to have identifiable risk factors or to complain of headache or blurred vision but more likely to report transient visual loss and manifest paralytic squint. Their immature language skills may account for the differences in expressing symptomatology subjectively. However, their commoner squint presentation and the lack of association with sex, overweight or medication use may reflect late presentation and/or a different pathophysiology. Dysregulation of glucocorticoid signalling can alter ICP dynamics and cause elevation of ICP in obese individuals,28 whereas the mechanisms of PTCS in non-overweight younger children remain unclear.
The strength of this study is that it is potentially free from intentional or unintentional bias: the robust BPSU scheme for reporting cases prospectively has 94% reporting rate29 by unselected general and specialised paediatricians across the UK and Ireland whose rate of reporting and case detection was consistent throughout the survey period. It is very improbable that any confirmed childhood PTCS cases were managed without the involvement of a paediatrician, and the study case definition was inclusive, so this study is likely to have captured the full spectrum of newly diagnosed PTCS. Nevertheless, missed or unreported cases are inevitable with the voluntary BPSU reporting scheme and our estimates should be regarded as an estimate of the minimum incidence rate. We cannot exclude the possibility that a higher proportion of all overweight cases was ascertained due to paediatricians having a higher index of suspicion of the disorder in those children. We did not have an alternative source of information from which to estimate incidence or confirm completeness of ascertainment using capture/recapture analysis.
Other strengths of the study were the avoidance of diagnostic error by evaluation of suspected papilloedema and drusen (ONHD) by ophthalmologists, submission of weight and height data, documentation of GA use at LP, confirmation of the diagnosis 1 year later and neuroimaging including exclusion of CVST, which may be clinically indistinguishable from PTCS.30 ,31 Limitations of the study include the lack of standardisation in the method of assessment of opening CSF pressure and the failure of neuroradiological reports, in most cases, to give specific consideration to specific neuroradiological markers of raised ICP, thus reducing the numbers of cases that could be categorised as ‘suggestive of PTCS’.
Overdiagnosis of PTCS relative to the study case definition was present in 13% of notifications. This carries a potential risk of harm, suggesting the need for greater awareness of the diagnostic criteria among paediatricians. The higher CSF opening pressures seen in children who were obese or had GA for LP support the upwards revision of the diagnostic CSF pressure threshold in these children.
In summary, this study provides three important findings relating to childhood PTCS. First, it suggests that it is a unitary syndrome and describes its epidemiology reliably. These observations should be generalisable to populations of similar ethnicity and weight profile. Second, it established female sex and obesity as the dominant risk factors from the age of 7 years. Third, it shows that children aged below 7 years do not show these risk factors and may present somewhat differently. The age-specific, sex-specific and weight-specific PTCS incidence data will help investigators to estimate the size of the population required to achieve an adequately powered interventional trial. These data also suggest that the avoidance of overweight and weight reduction may have considerable potential impact as primary and secondary preventive measure for PTCS in children over the age of 7 years.
Acknowledgments
The authors are very grateful to all the general and specialised paediatricians in the UK and Ireland who contributed to the notification and submission of survey questionnaires data, to the BPSU who assisted in the development of the study protocol and survey questionnaires, to SHINE (Spina Bifida, Hydrocephalus, Information, Networking, Equality; formerly the Association for Spina Bifida and Hydrocephalus) and IIH UK for their support, to Dr Krystyna Matyka for contribution in the study design and case ascertainment, to Dr Jim Turner, Senior Research Fellow, for statistical support and to Mrs Jayne Cooke for administrative support.
References
Footnotes
Contributors The surveillance study was designed by Y-YM with key input from KMc and FD in the development of study protocol and survey questionnaires. WPW, CRK and CPW provided oversight of the surveillance study conducted by Y-YM. Y-YM, FD, KMc, CPW, WPW and CRK evaluated the eligibility of notifications. Y-YM analysed and interpreted the collected data. ASR advised and provided input in the statistical analysis. Y-YM did the literature reviews, drafted and revised all versions of the manuscript. CRK together with contributions from all others (WPW, MJL, CPW, FD, KMc, GAS and ASR) involved in the data interpretation, revised all versions and approved the final version of the manuscript.
Funding This national survey was supported by the BPSU/RCPCH Sir Peter Tizard Research Bursary.
Competing interests MJL receives research grants from Action Medical Research, DES society, GOSH charity, NIHR, MS Society, SPARKS charity; receives research support grants from the London Clinical Research Network and Evelina Appeal; has received consultation fees from CSL Behring; received travel grants from Merck Serono and awarded educational grants to organise meetings by Novartis, Biogen Idec, Merck Serono and Bayer. GAS has been an investigator in MPSII clinical trials with Shire, has received speaker's honorarium and travel support from BioMarin.
Ethics approval The East London & the City Research Ethics Committee (07/Q0603/47), the Patient Information Advisory Group (PIAG/BPSU1-05[FT3]/2007) and the North Wales NHS Research & Development (JJ/jh/RP07/02/02).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All authors are willing to share all unpublished data from the study with bona fide researchers. The database can be made available to them through discussion with the corresponding author and the BPSU.