Article Text

Abstract
Objective This survey aims to describe and analyse the dosage regimens of antibiotics in French neonatal intensive care units (NICUs).
Methods Senior doctors from 56 French NICUs were contacted by telephone and/or email to provide their local guidelines for antibiotic therapy.
Results 44 (79%) NICUs agreed to participate in this survey. In total, 444 dosage regimens were identified in French NICUs for 41 antibiotics. The number of different dosage regimens varied from 1 to 32 per drug (mean 9, SD 7.8). 37% of intravenous dosage regimens used a unique mg/kg dose from preterm to full-term neonates. Doses and/or dosing intervals varied significantly for 12 antibiotics (amikacin, gentamicin, netilmicin, tobramycin, vancomycin administered as continuous infusion, ceftazidime, cloxacillin, oxacillin, penicillin G, imipenem/cilastatin, clindamycin and metronidazole). Among these antibiotics, 6 were used in more than 70% of local guidelines and had significant variations in (1) maintenance daily doses for amikacin, imipenem/cilastatin, ceftazidime and metronidazole; (2) loading doses for continuous infusion of vancomycin; and (3) dosing intervals for gentamicin and amikacin.
Conclusions A considerable inter-centre variability of dosage regimens of antibiotics exists in French NICUs. Developmental pharmacokinetic–pharmacodynamic studies are essential for the evaluation of antibiotics in order to establish evidence-based dosage regimens for effective and safe administration in neonates.
- Infectious Diseases
- Neonatology
- Pharmacology
- Evidence Based Medicine
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Most antibiotics are used off-label in neonates.
Local practice is variable to manage antimicrobial therapy in neonates.
Previous work demonstrated a considerable variation of dosage regimens of vancomycin and gentamicin among UK neonatal intensive care units.
What this study adds?
A considerable inter-centre variability of dosage regimens of antibiotics exists in French neonatal intensive care units.
Evidence-based dosage regimens of antibiotics should be validated for neonatal treatment on the basis of developmental pharmacokinetics–pharmacodynamics.
Introduction
Neonatal bacterial sepsis, classified as early or late onset, is a major cause of mortality and morbidity, particularly for premature neonates.1 ,2 Suspected infections are quite frequent in premature newborns and empirical antibiotic therapy is an emergency. If treatment is delayed or ineffective, neonatal sepsis can be rapidly fatal, making optimal use of antibiotics essential.
Previous work demonstrated a considerable variation of dosage regimens of vancomycin and gentamicin among UK neonatal intensive care units (NICUs).3 This implies that either toxic or subtherapeutic treatment courses may exist in neonatal clinical care, which obviously impacts clinical outcomes, especially for drug with narrow therapeutic index, such as aminoglycosides and vancomycin. We speculated that the variation in the dosage regimens is a common problem for antibiotic therapy in neonates because of limited number of high quality pharmacokinetic–pharmacodynamic studies. We surveyed local guidelines for antibiotic therapy in all French NICUs to evaluate the current local dosage recommendations.
Methods
Data collection
A total of 56 level 3 NICUs were identified from the directory of French paediatric intensive care network (Groupe Francophone de Reanimation et Urgences Pédiatriques): 54 metropolitan and 2 overseas. A senior doctor from each NICU was contacted by phone and/or email between May and June 2013 to participate in this survey.
Therapeutic guidelines and data extraction
All local therapeutic guidelines typically included various antibiotics, each of them with different dosage regimen defined by a dose and a dosing interval, based primarily on patients’ variables such as age, weight and/or renal function. The following data were extracted for each antibiotic in all guidelines: (1) drug name; (2) lower and upper bound values for the daily doses (mg/kg/day) and dosing intervals (h); and (3) variables for dosage individualisation, when used (i.e., age or weight). Exclusion criteria included: (1) dosage recommendations for infants with a postmenstrual age over 44 weeks4 or (2) therapeutic guidelines for meningitis.
Data analysis
The number of antibiotics in each local guideline, the number of dosage regimens and the distribution (minimum, median, maximum) of the lower bound and upper bound of daily dose and dosing interval in each local guideline were described for each antibiotic. Median of daily doses and dosing intervals for all the guidelines were calculated for each antibiotic. Inter-centre variability was assessed by comparing the medians of the daily dose and dosing interval among NICUs using non-parametric statistical test of Kruskal–Wallis (n>2 medians) or Mann–Whitney-Wilcoxon (n=2 medians). Statistical analyses were conducted using R software (V.3.0). A value of p<0.05 was considered statistically significant.
Results
All 56 French level 3 NICUs were contacted: 3 declared no local antibiotic guidelines and 9 declined participation. Thus, 44 (79%) agreed to participate.
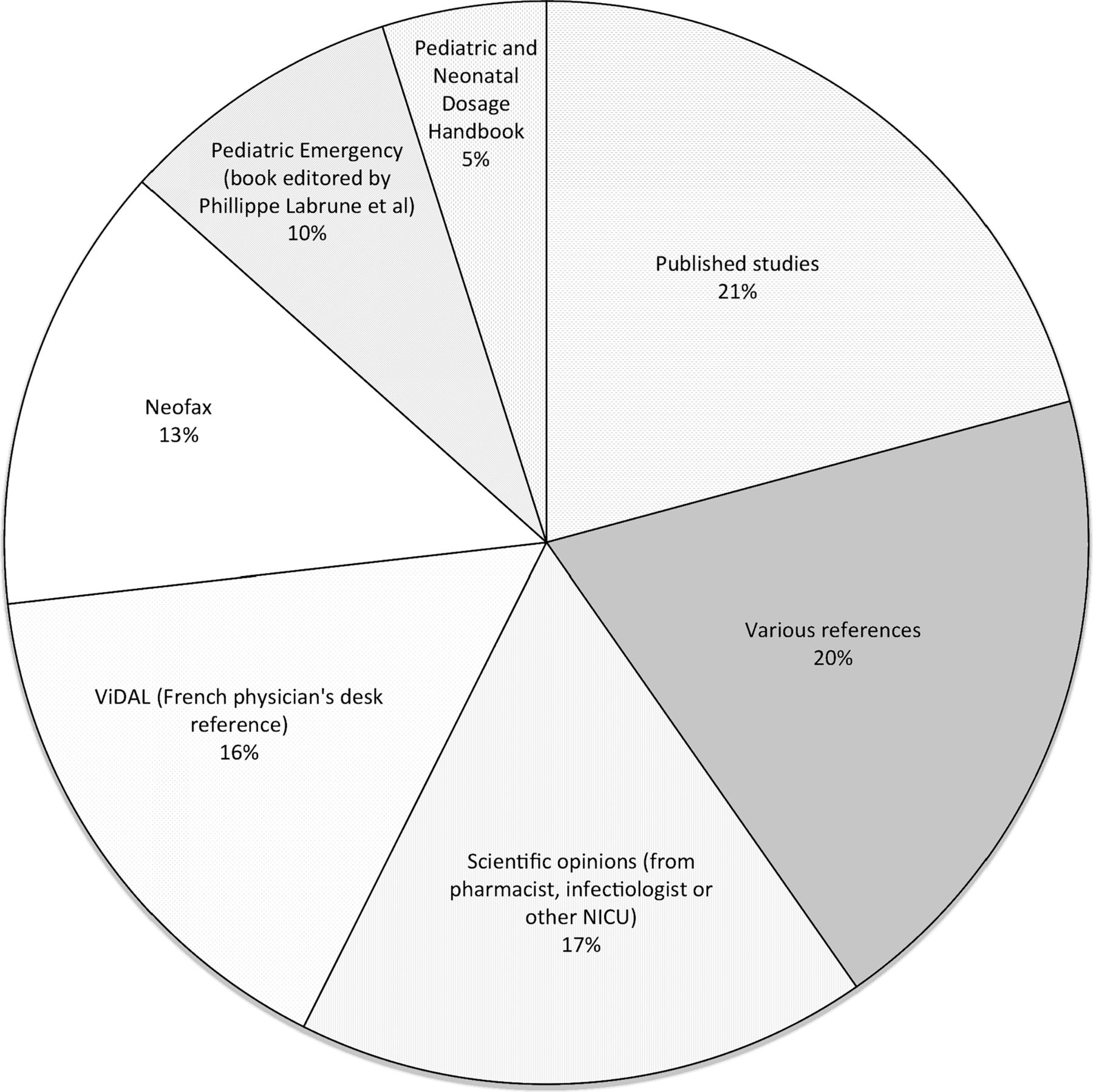
Each local guideline included a mean of 16 antibiotics (range 5–24). A total of 41 antibiotics were identified, including 19 beta-lactams, 4 aminoglycosides, 2 glycopeptides, 3 fluoroquinolones, 6 macrolides, 2 imidazoles, 1 sulfonamide and 4 other antibacterial agents. They are administered intravenously (n=31), orally (n=3) or both (n=7). Intravenous administration was either intermittent (n=37) or both intermittent and continuous (n=1), with a loading dose strategy in 4 cases (metronidazole, ornidazole, teicoplanin, vancomycin). The different sources from which the local guidelines were developed are illustrated in figure 1.

{kind=link}
Sources for local guidelines.
Inter-centre variability in daily dose and dosing intervals
Antibiotics with significant inter-centre variability in median daily doses and dosing intervals are presented in table 1.
The daily doses and dosing intervals of antibiotics with significant inter-centre variability: comparison with Neofax and RedBook
Daily dose
The daily doses were significantly different among NICUs for 9 antibiotics, administrated intravenously.
Maintenance daily doses were significantly different among NICUs for 8 antibiotics (amikacin, penicillin G, imipenem/cilastatin, netilmicin, cloxacillin, oxacilline, metronidazole, ceftazidime); 4 of them (amikacin, imipenem/cilastatin, metronidazole, ceftazidime) were included in more than 70% of local guidelines and their median daily doses varied from 2 to 5 times. Table 1 compared their doses in local guidelines with doses recommended by Neofax and Redbook.
Loading doses were significantly different for continuous infusion vancomycin (p<0.001), which was included in 78.4% of local guidelines. The loading dose varied 3 times (7–20 mg/kg).
Dosing intervals
The dosing intervals were significantly different for 5 antibiotics: gentamicin (p<0.001), amikacin (p<0.001), netilmicin (p<0.001), tobramycin (p<0.001) and clindamycin (p=0.023). Gentamicin and amikacin were included in more than 70% of local guidelines and median dosing intervals varied 3.5 times (12–42 h) (table 1).
Dosage individualisation
A total of 444 dosage regimens (407 intravenous and 37 oral) were used in French NICUs for 41 antibiotics. The number of different dosage regimens per antibiotic ranged from 1 to 32. In all, 37% of intravenous and 87% of oral dosage regimens used a unique mg/kg dose, without taking into account any patients’ characteristics. The most used covariate of dosage individualisation was age, which appeared in 88% of individualised dosage regimens.
Discussion
This study analysed the local guidelines used to prescribe antibiotics in the French NICUS and included 44 guidelines with a total of 41 antibiotics. Our data show considerable inter-centre variability as the number of antibiotics per local guideline varied from 5 to 24 and the number of dosage regimens from 1 to 32 per drug, with important differences in daily doses, dosing intervals and covariates used for dosage individualisation. These data highlighted the urgent need to optimise antibiotic prescriptions in neonates and developing evidence-based therapeutic consensus from already available data.
Antibiotics are extensively prescribed in neonates as infections are frequent and associated with a high risk of morbidity and mortality.5 ,6 However, few antibiotics have been evaluated in order to obtain a marketing authorisation for neonatal use and most of them are used off-label.7 ,8
As microbiologically evaluated infection is rare in neonates,9 treatment has to be started as early as possible and merely upon clinical suspicion. The initial choice of antibiotic therapy will depend on the clinical context and local bacterial epidemiology, while dosing will be ultimately determined by the area under the inhibitory curve AUIC (i.e., the AUC24 to MIC ratio of the antibiotic area under the concentration–time curve to the organism's minimum inhibitory concentration).10 To determine such ratio, MIC is based on sensitivity and resistance breakpoints of microorganisms provided by ‘The European Committee on Antimicrobial Susceptibility Testing—EUCAST‘ or by the ‘Clinical Laboratory Standards Institute’11–13 while AUC is patient dependant. Therefore, appropriate neonatal dosing needs to integrate the rapid developmental changes of the neonatal period, as reflected by covariates influencing drug disposition.14 Depending on the drug, these covariates are markers of size and maturation and may include gestational, postnatal, postmenstrual age, creatine concentration liver function tests and so on. Additional variables may be tested: disease, associated drugs, cardiovascular and ventilatory support.
Accordingly, regulatory guidelines15–17 recommend pharmacokinetic modelling and simulation approaches to establish neonatal dosage recommendation of antibiotics, underlying the importance of well designed pharmacokinetic studies.
However, evidence-based dosing regimens to support optimal prescriptions are lacking for almost all antibiotics in neonates, as illustrated by the two extreme examples of amikacin and metronidazole.
(1) For amikacin, 19 different neonatal dosing regimens are proposed in the literature18–32 and 31 were identified in the present study. None of them were clinically validated resulting in the lack of consensus on the optimal dosage regimen to be used in neonates. A consensus on neonatal dosing can only be evidence-based and requires a validated pharmacokinetic model (with both internal and external validation) but also clinical evaluation of the proposed regimen by a prospective efficacy and safety study.33 As pharmacokinetic studies in neonates usually have a limited number of patients included in many centres, study-related factors (such as characteristics of the neonates included, analytical methods to measure biological covariates or drug concentrations.) may have an important impact when extrapolating the published results to different clinical settings.34 In such cases, population pharmacokinetic meta-analysis might ensure thorough understanding of study-related pharmacokinetic differences in drug disposition, a prerequisite for clinical evaluation of efficacy and safety.
(2) For metronidazole, only 2 population pharmacokinetic studies with a limited number of neonates (n=32) have been published,35 ,36 even though the drug has been used for many years for treating complicated abdominal infections in neonates. Additional data are obviously required as treated patients are highly variable from extremely low birth weight to term neonates.
The French inter-NICU variability reported in this survey almost certainly reflects more common situations encountered in European countries or at the international level. Indeed, such heterogeneity in clinical practice is in agreement with previous data evaluating the dosage recommendations of vancomycin and gentamicin3 or ciprofloxacin.37 The National Institute of Health and Care Excellence guidance recommends a unique gentamicin starting dose of 5 mg/kg every 36 h for early onset neonatal infection treatment;38 however, the current clinical practice is variable for gentamicin therapy. In UK survey, 24 different combinations of dose were revealed and the dosing interval varied markedly from 12 to 48 h. In a French survey, we found 25 different combinations of doses and the dosing interval varied from 8 to 48 h. For vancomycin, clinical practice is even more variable in France, as both of continuous infusion and intermittent infusion were routinely used. Our results are also consistent with the previous findings by Porta et al39 who reported wide variation between four children's hospitals in the type and dose of antibiotic used in paediatrics based on daily prescription data.
We further compared the doses in local guidelines with dosages recommended by Neofax and Redbook,40 ,41 as they are frequently used reference books by neonatologists. Inconsistencies were highlighted, e.g. for ceftazidime, Neofax recommends 30 mg/kg per dose every 8 or 12 h according to postmenstrual age and postnatal age, while RedBook recommends 50 mg/kg per dose every 8 or 12 h according to body weight and postnatal age. Reaching a consensus on antibiotic therapy in neonates is urgently required, but will need close collaboration between paediatric pharmacologists and neonatologists.
Such variability in local guidelines, along with the paucity and poor quality of randomised controlled trials, highlights the difficulties in conducting studies assessing the effects of antibiotics in neonates,42 ,43 despite regulatory initiatives that encourage drug studies in neonatology.44 Several factors may explain this situation: (1) signs of neonatal sepsis (either early or late onset sepsis) are unspecific and antibiotic treatment has to be started as early as possible and merely upon clinical suspicion;9 (2) the empirical treatment varies between units, as it depends on local epidemiology and clinical context; (3) antibiotics with proven efficacy and safety in older paediatric patients or even adults frequently enter neonatal care because clinicians perceive them to have a more adapted spectrum of activity and/or better risks to benefit ratio than the currently used antibiotics; and (4) in such emergency situations, and whatever the study design (pharmacokinetics and safety or randomised controlled trial for efficacy), informed consent is difficult to obtain.45 ,46
In conclusion, this survey analysed the multiple dosage regimens to be followed to prescribe antibiotics in the French NICUs. A wide inter-centre variability was evidenced in terms of daily doses, dosing intervals and covariates used for dosage individualisation. Obviously, evidence-based dosage regimens of antibiotics should be validated for neonatal treatment on the basis of developmental pharmacokinetics–pharmacodynamics.
Acknowledgments
We acknowledge all neonatologists from paediatric and neonatal intensive care network (listed in alphabetic order) who participated in this survey (CH: centre hospitalier): Amiens CHU (G. Kongolo), Angers CHU Hôtel Dieu (S. Le bouedec, B. Leboucher), Arras CH (B. Theret, L. Desnoulez), Bayonne CH de la Côte Basque (P. Jouvencel), Bicêtre Hôpital Bicètre (D. Devictor, L. Chevret), Brest CHRU Morvan Brest (A. Garenne, JM. Roue), Caen, Hôpital Côte de Nacre (B. Guillois, A. Ceneric), Calais CH (MJ. Thieuleux, L. Egreteau), Clamart Hôpital Antoine Béclère (O. Romain), Chambery CH (M. Deiber), Cherbourg CH public du Cotentin (S. Saumureau), Clermont-Ferrand Hôpital Estaing (B. Bœuf, V. Poirier), Creteil—CH Intercommunal (C. Danan, X. Durrmeyer), Grenoble CHU Hôpital Couple Enfant (T. Debillon, L. Marcus, F. Audeoud), Lens CH Docteur Schaffner (C. Morisot, S. Klosowski), Lille Hôpital Jeanne de Flandre (L. Storme, A. Fily), Lyon Hôpital Femme Mère Enfant (O. Claris, F. Plaisant), Lyon Hôpital Croix Rousse (JC. Picaud, I. Jordan), Marseille Hôpital Nord (U. Simeoni, S. Hassid), Marseille Hôpital de la Conception (U. Simeoni, I. Ligi), Montpellier hôpital Arnaud de Villeneuve (G. Cambonie, R. Mesnage), Montreuil Hôpital André Grégoire (P. Daoud), Mulhouse—Hôpital Hasenrain (J. Nakhleh), Nantes Hôpital Mère-Enfant (JC. Rozé), Nice Hôpital Archet 2 (C. Dageville), Nimes CHU Caremeau (JB. Mariette), Noumea Hôpital Magenta (L. Tauzin), Paris Hôpital Cochin (PH. Jarreau), Paris Hôpital Necker Enfants-Malades (P. Hubert, M. Nicloux), Paris Hôpital Robert Debré (O. Baud, V Biran); Paris Hôpital Trousseau (D. Mitanchez, F. Kieffer), Perpignan Hôpital Saint Jean (P. Thevenot, R. Mesnage), Poissy CH Intercommunal (P. Boileau, G. Ciarlo), Pontoise Hôpital René Dubos (P. Boize), Reims, Hôpital Maison Blanche (P. Morville, A. David), Rouen Hôpital Charles Nicolle (S. Marret), Rennes Hôpital sud Anne de Bretagne (P. Pladys, P. Betremieux), Saint Brieux Hôpital Yves Le Foll (E. Boutaric), Saint Denis La Reunion CHU Felix Guyon (S. Samperiz, D. Ramful), Strasbourg Hôpital Hautepierre (D. Astruc, L. Palpacuer), Tours Hôpital Clocheville (E. Saliba, A. Bouissou), Troyes CH (I. Arnault), Valenciennes CH (F. Lapeyre, M. Hassan), Vannes CH Bretagne Atlantique (H. Journel, H. Bourdial).
References
Footnotes
Collaborators Societé Française de Neonatologie (http://sdp.perinat-france.org/SFN).
Contributors SL, ZW and EJ-A defined the study. SL contacted the NICUs with the participation of PB, PP and ES. SL, ZW and EJ-A planned the analysis. SL performed the analysis and wrote the first draft of the manuscript. WZ and EJ-A reviewed the manuscript; the last version was validated by all authors.
Funding This work was supported by “Treat Infections in NeoNates network” (TINN1 and TINN2, EU-funded FP7 projects, Grant Agreement numbers no 223614 TINN1; no 260908 TINN2) and Global Research in Paediatrics—Network of Excellence (GRIP, EU-funded FP7 project, Grant Agreement number 261060).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Drug therapy
- Atoms