Article Text

Abstract
Whether or not adolescence should be treated as a special period, there is now no doubt that the brain changes much during adolescence. From an evolutionary perspective, the idea of an under developed brain which is not fit for purpose until adulthood is illogical. Rather, the adolescent brain is likely to support the challenges specific to that period of life. New imaging techniques show striking changes in white and grey matter between 11 and 25 years of age, with increased connectivity between brain regions, and increased dopaminergic activity in the pre-frontal cortices, striatum and limbic system and the pathways linking them. The brain is dynamic, with some areas developing faster and becoming more dominant until other areas catch up. Plausible mechanisms link these changes to cognitive and behavioural features of adolescence. The changing brain may lead to abrupt behavioural change with attendant risks, but such a brain is flexible and can respond quickly and imaginatively. Society allows adolescent exuberance and creativity to be bounded and explored in relative safety. In healthcare settings these changes are especially relevant to young people with long term conditions as they move to young adult life; such young people need to learn to manage their health conditions with the support of their healthcare providers.
- Adolescent Health
- Neurodevelopment
- Transition
Statistics from Altmetric.com
Introduction
The transition of young people with long term conditions from childhood to adulthood, and the part health services should play in the transfer of their healthcare, have come to prominence in the last 10 years. This is partly because young people with such problems now live longer and partly because we know that this transition is often accompanied by poor health and social outcomes in terms of disease control, social participation and educational achievement.1–3
Government guidance on transition is prolific but does not have an evidence base.4 The Kennedy report5 identified the requirements of young people with complex health needs and the failure of commissioning groups to address these needs. More recently, the UK Child Health Outcomes Forum has recommended there should be two new indicators, one for transition and one for developmentally appropriate healthcare.6
The issues that need to be researched in transition have been set out,4 as have good practice principles in research with young people,7 and the National Institute for Health Research has funded a 5-year programme of research.8
Adolescent development used to be regarded as determined by changes in hormones and social expectations occurring in an unchanging brain. However, over the last 10 years it has been recognised that the adolescent brain changes in fundamental ways, as striking as the changes over the first few years of life or in old age. Also, this period of change lasts longer than puberty and should be considered to extend from 11 to 25 years of age.9–11
The teenage years may be marked by certain indisputable biological and social realities, but what is widely understood as ‘normal adolescence’ is socially constructed.12 Anthropological and historical research has demonstrated that what it means to be young varies between cultures and over historical periods.13 ,14 For instance, in our time, many people in their twenties now return or continue to live at home for economic reasons, while increased life expectancy may persuade young people to spend more time exploring places, jobs and relationships, thus delaying their search for a permanent job or long tem relationship. This article will not discuss further these interesting issues because we want to concentrate on the very concrete changes that occur in the brain between the ages of 11 and 25.
In this article we link some of the behavioural manifestations of adolescence to the new knowledge of brain morphology, neurochemistry and function. We will then discuss their relevance to healthcare providers of services for young people with long term conditions in transition from childhood to adulthood.
Anatomical, hormonal and neuro-chemical changes
Cortical grey matter
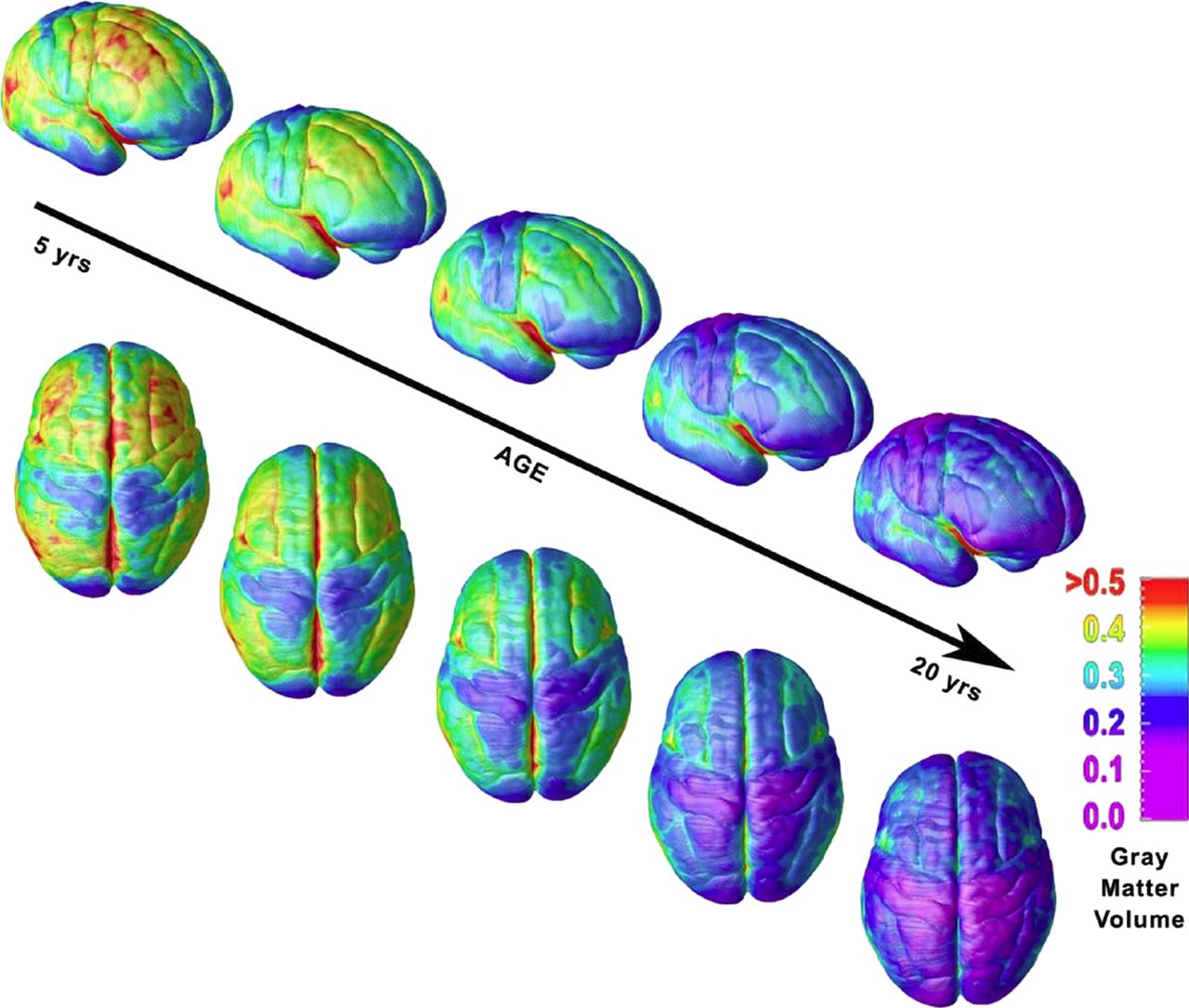
In the adolescent brain there is a gradual increase in grey matter followed by reduction—the so-called inverted U.9 ,15–17 The sensory and motor regions mature first, followed by the remainder of the cortex, with a posterior to anterior loss of grey matter and the superior temporal cortex being the last area to change15 (figure 1).18 Histological studies, mainly in animals, show there is massive synaptic proliferation in the pre-frontal area in early adolescence, followed by a plateau phase and subsequent reduction and reorganisation. Longitudinal imaging studies in humans have recently confirmed histological studies. It is the rarely used synaptic connections that are assumed to be pruned, leading to a more efficient and specialised brain.19 ,20

Right lateral and top views of the dynamic sequence of grey matter maturation over the cortical surface. The side bar shows a colour representation in units of grey matter volume. Fifty-two scans from 13 subjects each scanned four times at approximately 2-year intervals.
Of particular interest are the pre-frontal cortices which are thought to be the site of executive control of planning, emotional regulation, decision making, multi-tasking, self-awareness, impulse control and reflective thought.
White matter
White matter tracts between the pre-frontal cortex and sub-cortical structures develop9 in a steady but non-linear manner,11 with more rapid development of functional tracts in early adolescence and levelling off in young adulthood. The changes reflect a mixture of on-going myelination and increased axonal diameter. In contrast to grey matter changes, the white matter increases occur in all lobes of the brain simultaneously.16 ,21–23 The most recent studies, using diffusion tensor imaging (DTI) (see the online supplementary appendix titled ‘Neuroimaging methods to study brain development’) have shown that this increased myelination and axon density in white matter tracts between the pre-frontal cortex and basal ganglia continues to develop throughout adolescence.11 ,24 ,25
Sub-cortical grey matter
The basal ganglia or nuclei are: the striatum (caudate nucleus and putamen), ventral striatum (nucleus acumbens), globus pallidus, subthalamic nucleus and substantia nigra. These nuclei are involved in transmission circuits which control movement and higher order cognitive and emotional functioning. The limbic system, consisting of the hippocampus, amgydala, septic nuclei and limbic lobe, is closely involved in emotional regulation, reward processing, appetite and pleasure seeking.
Due to their small size, accurate visualisation of these regions is more difficult than for cortical grey matter; however, the caudate nucleus follows a similar ‘inverted U’ shape trajectory and limbic structures develop sooner than the basal ganglia.18
Pubertal hormones
Grey matter changes in the same sequence in boys and girls, but girls' grey matter peaks about 1 year before that of boys.9 This difference corresponds to pubertal maturity, suggesting brain development and puberty may be inter-related.26 The behavioural changes of adolescence correspond to the timing of puberty, not chronological age, as do the gender differences in mental health problems such as depression.
Striatal volumes are unrelated to pubertal stage or circulating testosterone level. However, larger grey matter volumes in limbic system structures in both sexes are associated with later stages of puberty and higher levels of circulating testosterone. There is a differential sensitivity between boys and girls to testosterone in the limbic structures and this may be responsible for the greater risk of anxiety and depression in girls.27 ,28
Neurotransmitters
Adolescence brings a peak in the brain's sensitivity to dopamine, the neurotransmitter which appears to prime and fire reward circuits and to reinforce learning.29 Dopamine systems are necessary for ‘wanting’ incentives and the neuro-circuitry of reward seeking is thought to be determined by dopamine signals received by the nucleus accumbens.29 Organisational changes in the dopaminergic system have been observed in non-human primates as well as in humans.30 Dopamine receptors increase in the striatum and pre-frontal cortex in adolescence and then decline, but this is not due to underlying pubertal hormone levels.31
Oxytocin, the hormone commonly known for its role in a variety of social behaviours, including social bonding in maternal behaviour and hostility to those outside a person's core social group,32 can also act as a neurotransmitter and may play an important role during adolescence. Gonadal steroid levels are strongly correlated with oxytocin-mediated neurotransmission in the limbic areas,33–35 where there is proliferation of oxytocin receptors. These changes in oxytocin transmission may explain why adolescents show heightened responses to emotional stimuli in comparison to children and adults.
In summary, these changes in the adolescent brain represent a period of ‘pruning, re-wiring and insulation’, that sees predominant neural circuits surviving and becoming more efficient. This happens first in primary systems (such as motor and sensory) in early adolescence, with executive systems (memory, planning, emotional regulation, decision-making and behavioural inhibition) maturing into young adulthood.
Development of the atypical or damaged adolescent brain
These are important areas for research and below are four examples where possible mechanisms have been hypothesised.
Schizophrenia
As far back as 1982, Feinberg36 postulated that schizophrenia, which typically begins in adolescence, might be related to exaggerated synaptic pruning, for he had noticed those with schizophrenia had a more pronounced reduction in delta rhythm sleep than those without schizophrenia. Subsequent studies of other indicators of exaggerated synaptic pruning37 ,38 and post mortem studies39 continue to support this hypothesis.
Head injury
Concussion may not be a mild event, especially if recurrent. The best predictor of further concussion is having had a head injury because the damage compromises brain areas regulating memory, co-ordination and speed of judgement, so making further head injuries more likely. Adolescents experience more recurrent concussion that older and younger children due to their participation in sport and the effects may be more significant because of the rapid and complex changes their brains are undergoing.40
Severe head injury in childhood may appear to be followed by striking recovery to the developmental stage the child had reached before the injury. However, after a number of settled years significant behavioural, attentional and psychological problems may then appear in the teenage years.41 ,42 The assumption is that damage to grey matter and white matter tracts is masked until the maturation phases of adolescent brain development begin.43
Cerebral palsy
Children and young people with cerebral palsy have increased rates of psychological and behavioural difficulties as compared to the general population.44 Such problems seem to start early in life,45 and this argues against the maturation of their damaged brain in adolescence being a significant factor; indeed there is evidence that such difficulties may be due to the different ways in which parents manage a disabled child in the early years.46
Diabetes
Mild cognitive effects of hypoglycaemia appear soon after diagnosis and by adolescence executive function deficits and low vocabulary and general knowledge test scores are found.47 ,48 The protracted period of myelination in the frontal lobes during adolescence also renders adolescents vulnerable to hyperglycaemia. Poorer metabolic control is associated with higher levels in the frontal and temporal lobes of myoinositol and choline, which are related to demyelination and gliosis.49 Low levels of N-acetylaspartate (indicating neuronal death or reduced neuronal metabolism) are found in the frontal lobes and basal ganglia.50 The effects of long term poor metabolic control on planning, organisation and memory could influence the ability of young people to manage a complex regimen and understand the cause–consequence interactions of not following the regimen.
Behavioural changes
A number of behavioural changes throughout adolescence are postulated to be adaptive mechanisms for the human race.51 Increased importance is attached to social behaviour, and there is increased novelty seeking, reward seeking, impulsivity and risk taking, all of which tend to be interlinked.
Novelty seeking
Novelty seeking is a striking feature of adolescence and it is hypothesised that it may be an important part of our evolution, contributing to the search for different sources of food and mates.52 ,53 However, novelty seeking also renders adolescents more susceptible to harm. Boys in particular experience higher rates of serious injuries than children or young men in their late twenties.54 ,55
Reward seeking
Reward seeking behaviour increases at the onset of puberty, peaking around age 15, after which it begins to decline.56 For instance, younger adolescents are less likely to wait for monetary rewards as compared to older adolescents.57 Functional brain imaging shows that the nucleus accumbens and amygdala have increased activity in response to rewards in adolescents.58 Behaviour that seeks social rewards affects the same brain regions as for other sorts of reward.59
Impulsivity
Impulse control is largely dependent on the ability to suppress irrelevant thoughts and actions in order to focus on the goal in question, especially when there are appealing distractions.60 Impulse control improves in an almost linear course with age.56 ,61 In a ‘go-no-go’ task, functional MRI showed the pre-frontal cortex was activated, and improving impulse control was associated with maturation of the pre-frontal cortex and basal ganglia.20
Risk taking
The risky behaviours that adolescents take part in, such as drink driving, drug taking or unprotected sex, are not due to their ignorance or perceived invincibility as adolescents in fact evaluate risks in the same way as adults, even tending to overestimate risk.62 ,63 Increased risk taking in adolescents is associated with the drive to try something new61 ,64 and is thus intertwined with their novelty seeking behaviour.
In contrast to the linear improvement of impulse control with age, risk taking is exaggerated in adolescence, relative to both children and adults.58 ,65 Development of the sub-cortical structures appears to out-run the development of the pre-frontal cortex, which progresses at a steady pace.66 Strong reward and novelty seeking behaviour cannot be fully restrained by impulse control which was sufficient in 10-year-olds but does not then keep up until full maturation of the pre-frontal cortex. Thus, rapid change in dopaminergic activity in the sub-cortical grey matter renders the neural circuits hypersensitive to reward and novelty at a time when the pre-frontal cortex has not changed sufficiently to deal with this large, sudden sub-cortical drive. This may not be a steady state; adolescents understand risks well but they sometimes make apparently odd decisions, often in exciting or stressful situations and especially in the presence of peers—so-called ‘hot cognition’. The increase in activation of the nucleus accumbens and amygdala when making risky choices is more pronounced when emotional information is also being processed.58 ,67
Social behaviour
Adolescents become more sociable, form more complex social relationships and are more sensitive to peer acceptance and rejection than younger children.68–70
It is postulated that there may be a ‘social brain’.71 Functional MRI has revealed parts of the brain associated with empathy,72 theory of mind,73 facial processing74 ,75 and being influenced by acceptance and rejection of peers.76 While these abilities operate from about 4 years of age, studies in adolescence show that the skills develop further, corresponding to the white and grey matter changes in the medial pre-frontal cortex and temporo-parietal regions. In laboratory tasks that require various types of mentalising about other people and their intentions, these regions were much more active in adolescents than in younger children or in 25-year-olds.71 ,73
Adolescents attach great importance to socialising with peers52 and find such relationships more rewarding than adults do.77 These interactions help develop social skills away from the home environment. It is not clear how peer approval comes to dominate over other spheres of social approval. Socialising may also have disadvantages and several studies show adolescents are hypersensitive to peer rejection as compared to children or adults.68–70 The ability to regulate the psychological distress caused by social ostracism develops through adolescence into adulthood.78
Impact of behaviour
Adolescents are risk-takers and view ‘anything as possible’. This, combined with their adaptability, enables adolescents to push ideas and boundaries to the limit. However, there are disadvantages that include the increased risks of road traffic accidents, sexually transmitted infections, unwanted pregnancies and substance abuse.79 Mortality rates are higher than in childhood or the early twenties, with the majority of deaths resulting from suicides or accidents.54 ,57 There is also an increased vulnerability to mental health problems, in particular affective disorders and substance abuse.80 ,81
Teenagers are more likely to engage in risky behaviours when they think their peers are doing the same.82 ,83 The risky activities that sometimes end in disaster usually happen when the adolescent is with peers in an exciting situation. Such behaviours can be modelled in laboratory games—for example, in relation to driving.84 ,85
Relevance to healthcare and transition of young people with long term conditions
Our paper has indicated a number of changes in the brain and behaviour which have implications for adolescent healthcare. These implications are relevant to all teenage healthcare but are especially important in the context of a long term health condition where there is a need for regular healthcare and transfer of care between paediatric and adult health services.
In the transition of young people with long term conditions we must take account of the realities of the adolescent brain, rather than attributing adolescent behaviour to ‘being difficult’. UK86 and Australian guidance87 is available, now supported by the neuroscientific literature we have reported. Effort should be made to get communication right in a manner that suits teenagers. It may not come easily to paediatricians or adult physicians, but if we are to engage adolescent patients we must employ tactics that adolescents are programmed to value. Adolescents want to feel secure, needing people to be friendly, considerate and approachable. This does not mean the physician should try to be ‘cool’ and youthful, rather that he/she should be open, use more facial expression, and take an interest in the young person as well as their illness. Adolescents are learning to value and understand relationships outside of the family. They are nervous and we have to respond to them in an open, friendly manner. They need in their hesitating ways, to form relationships and value structures outside the family and this must also happen in healthcare settings.
Imposing one's views of good healthcare on the young person may produce a defiant reaction, with deliberate non-compliance. It may also stop the young person experimenting with different approaches to their health and healthcare management. The adolescent brain is more flexible, excitable, original and adjustable than the adult brain and needs to find its own way of incorporating new behaviour, rather than being imposed upon by anxious health providers. Thus, adolescents need graded opportunities for self-management and risk taking. Peer support can be very helpful if it validates a decision, but being with peers may also lead to perverse decisions. Adolescents should not be asked to make key decisions at times of excitement or stress.
Our earlier discussion of the social brain suggests that adolescence is a period where confidence in managing one's own condition might come more easily from peer interaction than from educational programmes delivered by healthcare providers. There is mounting evidence to support this, for example, from experience of residential camps for those with diabetes88 ,89 and from promotion of social forums for those with long term renal problems.90
Paediatricians should be aware that adolescents themselves are learning about the changes taking place in their brains. Figure 2 is from a booklet91 designed by a 17-year-old from Cambridge after her experience of an admission to hospital. Also, this internet link http://www.islingtoncommunitytheatre.com/brainstorm, is to a drama production about adolescence by an adolescent group. Finally, we should remember that most medical students are still in adolescence.

{kind=link}
{kind=link}
A page from a booklet91 written by Jessica Platt, an A-level student.
Appendix: neuroimaging methods to study brain development
Current knowledge of adolescent brain development has depended on new neuroimaging techniques. The key investigations used are structural MRI, functional MRI and DTI.
Structural MRI identifies pixels and three dimensional voxels (volume elements) which are then examined by computer algorithms to determine whether the tissue type looks grey matter, white or is cerebrospinal fluid. However, there are uncertainties about precisely what tissues underlie grey and white colour appearances on scans. Grey matter consists of neurones, dendrites, synapses and short axons; white matter consists of axons, myelin, astrocytes and oligodendrocytes. A change in appearance of a brain area, from for example, grey to white, may imply a reduction in grey matter or alternatively an expansion of white matter with no loss of grey matter.
Functional MRI (fMRI) identifies brain regions with increased blood flow during specified tasks. It uses blood-oxygen-level-dependent contrast (BOLD) to generate a colour-coded representation of the active brain areas. The limitation of this technique is that it takes several seconds for these blood flow changes to be identified and therefore certain brain regions could be missed out at the start of a task. It is not known how the MRI structure relates to the BOLD signal of fMRI and nor is there evidence yet of developmental changes in the relationship between BOLD and structure.
There are also studies which examine the functional connectivity between brain regions. Some are resting state (in the absence of any task) and explore trends over time. Resting state fMRI examines the functional connectivity between brain regions. Other techniques use statistical techniques (psycho-physiological interaction analysis) to examine differences in connectivity during different tasks.
DTI allows identification of white matter tracts. DTI measures the diffusion properties of the water molecules in the white matter and how they interact with the tissue structure. DTI can therefore describe not only the size of the tissue matter but also the direction and organisation of the water molecules; this provides a picture of the projections of white matter tracts to different brain regions (see figure A1).1
None of these imaging modalities provide both high temporal and spatial resolution. Therefore information from several different imaging modalities must be integrated.
Reference
1. Vincent J, Schmithorst WY. White matter development during adolescence as shown by diffusion MRI. Brain Cogn 2009;72:16–25.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors SL undertook the preliminary literature search and drafted the article. AC participated in planning the study, coordinated the study, revised the draft article and added further references, took overall responsibility for delivery of the work and approved the final version. AC had full access to all the data in the study and had final responsibility for the decision to submit for publication. AC is guarantor.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.