Article Text

Abstract
Objective: To compare the current prevalence of risk factors for sudden infant death syndrome (SIDS) in Sweden with a decade earlier, and assess factors associated with prone sleeping.
Methods: The results of a cohort study (Infants of Western Sweden) and a population based case-control study (Nordic Epidemiological SIDS Study) were examined. Subjects were 5600 healthy 6 month old infants born in 2003 in the Western Sweden region and 430 healthy Swedish infants born between 1991 and 1995.
Results: Prone sleeping decreased from 31.8% to 5.6% and supine sleeping increased from 35.3% to 47.3%. Side or side/supine sleeping increased from 25.2% to 43.8%. Maternal smoking during pregnancy decreased from 23.5% to 9.5%. The risk for prone sleeping increased if the mother was unemployed (OR 2.4, 95% CI 1.5 to 4.0), if she was a heavy smoker in the third trimester (OR 44.1, 95% CI 1.6 to 1199.6), and if the child was irritable (OR 2.5, 95% CI 1.3 to 5.1), shared a bedroom with siblings (OR 2.6, 95% CI 1.0 to 6.6), or never used a dummy (OR 3.2, 95% CI 1.9 to 5.4).
Conclusions: Parents have complied with advice to prevent SIDS given at infant welfare centres for the last 10 years. A change in the preferred sleeping position from side variants to exclusively supine, and reducing the number of pregnant women smoking may be beneficial. Use of a prone sleeping position was associated with maternal employment status, maternal smoking, temperament of the child, dummy use, and sharing a bedroom with siblings.
- epidemiologic factors
- maternal smoking
- prone position
- SIDS incidence
- sudden infant death syndrome
Statistics from Altmetric.com
The incidence of sudden infant death syndrome (SIDS) increased in most Western countries in the 1980s.1 At the end of that decade, evidence started to accumulate that prone sleeping was a major risk factor.2,3 Following campaigns to avoid the prone sleeping position, there was a dramatic decrease in SIDS incidence. This was also seen in Sweden,4 although the initial incidence from an international perspective was low (1.1 deaths per 1000 live births in 1991). In Sweden, the campaign to reduce the risk of SIDS promoted a supine sleeping position, non-smoking, breastfeeding, and not over-wrapping the infant.
In the Nordic Epidemiological SIDS Study, we were able to demonstrate that risk factors for SIDS in Scandinavia were prone sleeping,4,5 smoking,6 bottle feeding,7 symptoms of infectious disease,8 and social factors.9 It is recommended that all infants in Sweden receive vitamin A and D supplements. In a paper from the Nordic Epidemiological SIDS Study, we showed that infants not receiving these supplements had a higher risk of SIDS.10 Prone sleeping decreased during the study period of 1992–1995.4
After the Nordic Epidemiological SIDS Study was completed in 1995, no further SIDS case-control studies were carried out in Sweden.
The aims of the present study were to compare the prevalence of SIDS risk factors today with those of a decade earlier and to examine why babies are still placed prone to sleep. To achieve this, we have utilised the ongoing study Infants of Western Sweden and compared these data with Swedish controls in the Nordic Epidemiological SIDS Study. In the former study, we also investigated determinators for prone sleeping among 6 month old infants.
METHODS
Infants of Western Sweden
The Infants of Western Sweden is an ongoing study in the Western Sweden region. The region has 1.5 million inhabitants, which is equal to one sixth of the Swedish population. It embraces urban, rural, and coastal areas, and the chief city is Göteborg, with 500 000 inhabitants.
Of the total birth cohort of 16 682 infants born in the region in 2003, the families of one half (8176 families) were randomly selected and sent an invitation to participate together with a questionnaire to be filled out when the infant had reached the age of 6 months. The questionnaire was filled in by 5600 parents, that is, the response rate was 68.5%.
The Nordic Epidemiological SIDS Study
Conducted between 1992 and 1995, the Nordic Epidemiological SIDS Study clarified the epidemiology of SIDS in Scandinavia at the beginning of the 1990s. The study recruited 244 cases and 869 matched controls in Norway, Sweden, and Denmark, of which 117 cases and 430 controls were from Sweden. The response rate was 83% among cases and 72% among controls. The mean age of the infants used as controls was 19 weeks. Details of this study have been reported previously.4,5
SIDS incidence
Information on SIDS incidence was obtained from data from the National Board of Health and Welfare and forensic departments. In Sweden, infants who die outside hospital undergo forensic autopsy.
Statistics
Comparisons were carried out using the Epi Table option in Epi Info v. 6.0.4.11 Binary logistic regression was used to calculate odds ratios for factors associated with prone sleeping position using the SPSS statistical package.12
The percentage of missing answers was 0.0–4.4% in the Nordic Study, and in the Western Sweden study 0.4–4.0%, with the exception of when breast feeding was stopped, where 12.3% of answers were missing. This is probably due to the fact that many mothers continue to breast feed after the age of 1 year and thus could not state when breastfeeding was stopped.
Ethical approval
Ethics committees approved both studies. The Nordic Study was approved in all participating countries, and Infants of Western Sweden was approved by the Ethics Committee of Göteborg University.
RESULTS
SIDS incidence
Following the advice introduced in 1992 on supine sleeping, non-smoking, breastfeeding, and not over-wrapping infants, a rapid decrease in SIDS incidence was seen between 1992 and 1995, followed by a gradual decrease between 1995 and 2000. SIDS incidence has since been stable at between 0.2 and 0.3 per 1000 live births. In 2004 the incidence was 0.28 per 1000 live births (fig 1).

SIDS incidence in Sweden 1975–2004, cases per 1000 live births. Data are from the National Board of Health and Welfare and forensic departments in Sweden.
Sleeping position
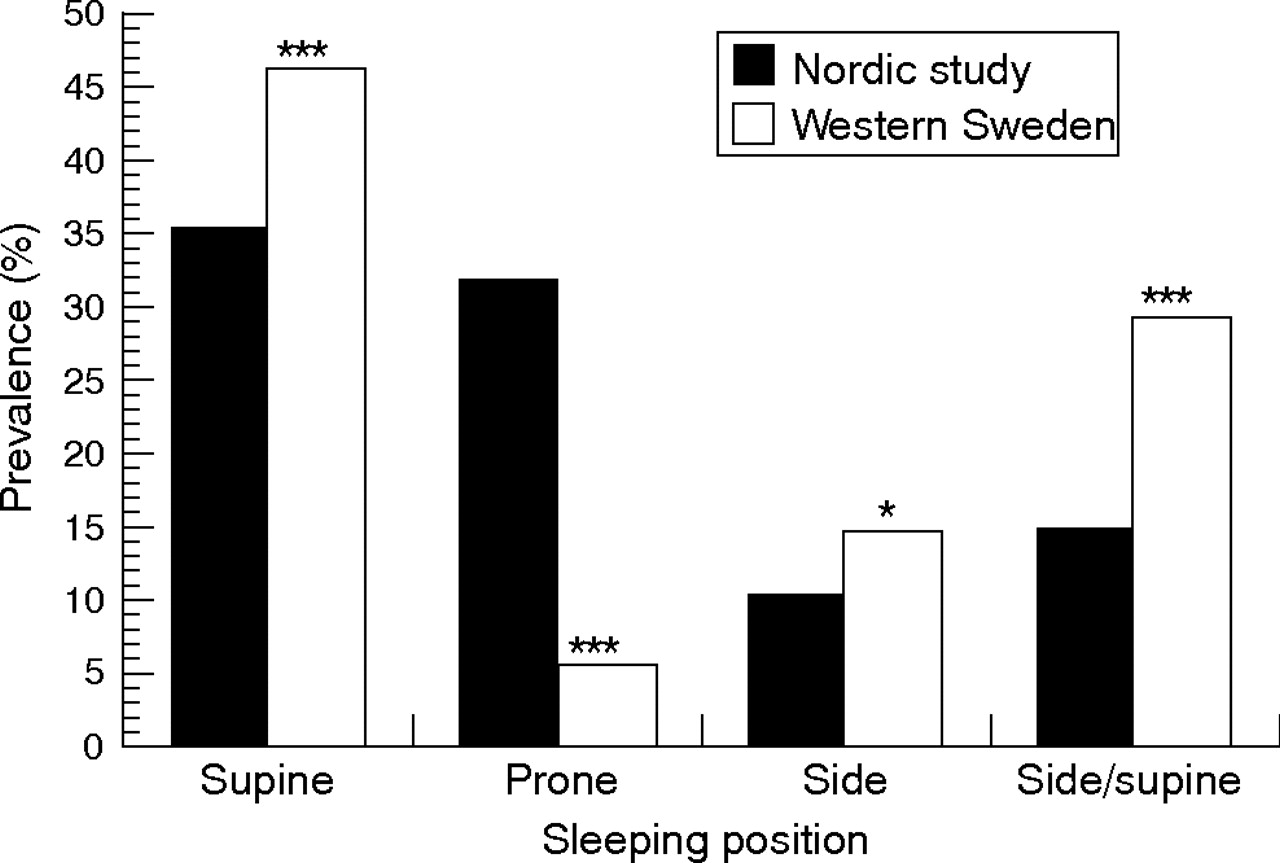
We have seen a significant increase in the number of infants always sleeping in the supine position, and a significant decrease in infants sleeping prone. Among 6 month old infants in Western Sweden, only 5.6% sleep prone compared to 31.8% a decade ago. The prevalence of infants sleeping exclusively supine has increased from 35.3% to 47.3%. The fraction alternating between side and supine sleeping positions has increased from 14.8% to 29.1%, and the fraction using exclusively side sleeping has increased slightly from 10.4% to 14.7% (table 1, fig 2).
Percentage of infants with different epidemiological factors among healthy Swedish infants between 1992 and 1995 (control infants of the Nordic SIDS Study, mean age 19 weeks) and in 2003 and 2004 (Infants of Western Sweden, age 6 months)
{kind=link}
{kind=link}
Sleeping position in healthy Swedish infants between 1992 and 1995 (Swedish control infants of the Nordic SIDS Study) and in 2003–2004 (Infants of Western Sweden). ***p<0.001; *p<0.05.
Smoking
In the Western Sweden study only 9.5% of the mothers smoked during pregnancy compared to 23.5% in the Swedish controls of the Nordic Study. The figures for smoking after pregnancy were 8.6% and 25.4%, respectively.
Breast feeding
Breast feeding rates remained largely unchanged with 64.3% of 6 month old infants in Western Sweden being breast fed in 2003 compared to 67.5% of control infants in the Nordic Study.
Alcohol habits
A very small fraction, only 0.2% of the mothers in the Infants of Western Sweden study admitted frequent (more than once a week) alcohol use during pregnancy, which was significantly lower than the 0.9% among the Nordic Study control mothers. After pregnancy, the corresponding figures were 0.6% and 3.3%, respectively, which was a highly significant difference.
A and D vitamins
Among Western Sweden infants in 2003, 5.7% of infants did not receive vitamin A and D supplements. In the Nordic Study, this figure was 2.7%
Sleeping in own bedroom
Fewer infants slept in a separate bedroom in 2003 (12.6% compared with 28.8%).
Regular maternity controls
While 0.4% of the control mothers in the Western Sweden study had not visited the maternity health centre regularly, this figure was 1.4% among the Swedish controls in the Nordic Study.
No differences
There has been no increase in the prevalence of breast feeding following the introduction of the campaign to reduce the risk of SIDS. Furthermore, there were no differences regarding admissions to neonatal wards, the use of a pacifier/dummy, colicky pains, the prevalence of co-sleeping, or the prevalence of sleeping indoors with outdoor clothes on (table 1).
Factors associated with prone sleeping
The following variables were used to analyse what determines the prone sleeping position: birthweight <2500 g, parents not cohabitating at birth, parents not cohabitating at 6 months, more than two siblings, father ill, mother ill, father unemployed, mother unemployed, low paternal education, low maternal education, living in an apartment, location of housing (city centre, suburban, other densely populated area, or rural), no access to a summer holiday house, dampness or mould at home, air pollution, no regular maternity check ups, any alcohol during pregnancy, any alcohol after pregnancy, medication during pregnancy, admission to neonatal ward, antibiotics in the neonatal period, exclusive breastfeeding in the first week, temperament in the first week, feeding problems in the first week, maternal smoking, mother used smoke-free tobacco during pregnancy, paternal smoking, sleeping position in the first week, sleeping place, hours spent outdoors per day, sleeping indoors with outdoor clothes on, difficulties going to sleep, easy to wake up, difficult to wake up, troubled sleep, waking up more than three times at night, temperament at 6 months, colicky pains, poor appetite, dummy use, and season of birth.
All variables were analysed in a univariate model; variables with a significant effect were re-analysed in a multivariate model. We found that the factor with the strongest association with prone position at 6 months was how the infant was placed to sleep in the first week (univariate OR 38.1, 95% CI 24.9 to 58.3 for strictly prone; multivariate OR 42.7, 95% CI 21.3 to 85.7 for strictly prone).
Therefore, to identify which factors determined the use of the prone sleeping position in the first week, the same procedure was then repeated with all initial variables, first in a univariate and then in a multivariate model, the latter consisting of variables with a significant effect in the former.
In the multivariate analysis of factors associated with sleeping position in the first week (table 2), the following variables were significantly associated with an increased risk for prone sleeping: if the mother was unemployed (OR 2.4, 95% CI 1.5 to 4.0), if the child was irritable (OR 2.5, 95% CI 1.3 to 5.1), if the mother was a heavy smoker in the third trimester (OR 44.1, 95% CI 1.6 to 1199.6), if the child shared a bedroom with other children (OR 2.6, 95% CI 1.0 to 6.6), or if the child never used a dummy (OR 3.2, 95% CI 1.9 to 5.4).
Prevalence of factors associated with prone sleeping at 1 week of age with odds ratios in Western Sweden 2003–2004 (significant variables in the multivariate analysis)
Non-significant variables in the multivariate analysis were: parents not cohabitating at birth, more than two siblings, father unemployed, low paternal education, low maternal education, maternal smoking in early pregnancy, low or moderate maternal cigarette consumption in the third trimester, paternal smoking, sleeping in parental bed, or infant being a light sleeper.
DISCUSSION
The rapid decrease in SIDS incidence between 1992 and 1995 paralleled an equally rapid decrease in the use of the prone sleeping position. At the same time, a parallel decline in post neonatal mortality was seen.4 A more gradual decrease in SIDS incidence was observed between 1995 and 2000, with a levelling off between 2000 and 2004. The lack of further decline in SIDS incidence after 2000 may be because it is possible that the main decrease in prone sleeping position occurred before 2000. However, the gradual decline in smoking during pregnancy has been continuous, and we do not know why this is not reflected in a corresponding decrease in SIDS incidence in recent years.
The decrease in SIDS incidence was paralleled by a decrease in prone sleeping between 1995 and 2004. However, during this period smoking during pregnancy also decreased, which it did not between 1992 and 1995, suggesting that smoking behaviour is more resistant to campaigns.
The prevalence of side and an alternating side/supine position during sleep is still high and is rising in Sweden. Several studies have found an increased risk of SIDS with the side position,5,13 and a recent publication from the CESDI study14 reports more than multiplicative risks when the side position is combined with birth weight <2500 g. As in numerous other countries, the side position is advocated in many maternity wards in Sweden, supposedly for fear of aspiration. This is a matter of concern, and these findings on SIDS need to be communicated to maternity ward staff.
Since the prone position is preferred by 5.6% of families in Western Sweden, in spite of the well known dangers, we examined why this position is still used. In a univariate analysis we found several factors to be significantly associated with the choice of prone position at 6 months of age, and these were then analysed in a multivariate model. However, in both the univariate and the multivariate analysis, the factor with the strongest association with prone position at 6 months was that the infant was placed prone to sleep in the first week. When the same analyses were repeated with prone position in the first week as the dependent variable, we found that the choice of prone sleeping position is determined by maternal employment status, maternal smoking, temperament of the child, dummy use, and sharing a bedroom with other children. However, these results must be viewed with caution, since only 133 infants slept prone, which is fewer than the number of missing answers regarding sleep position at 1 week (137 were missing).
What is already known on this topic
-
Prone sleeping and maternal smoking are major preventable risk factors for SIDS.
-
In Sweden, prone sleeping decreased, supine sleeping increased, and smoking during pregnancy remained unchanged during the first years after a campaign was launched to reduce the risk of SIDS.
-
A rapid decrease in SIDS incidence occurred between 1992 and 1995, paralleling abandonment of the prone sleeping position, followed by a slower decrease between 1995 and 2000.
It is well known that infants sleep better in the prone position and when they use a dummy. Therefore, we believe that infants not using a dummy, especially fussy infants, might be placed prone to make them sleep better. In a bedroom with older children, because of the possibility of disturbance, it might also be easier for a small infant to sleep when prone. Why maternal unemployment increases the risk is a more difficult question. It is possible that unemployment reflects a social situation with increased strain on the family, which might lower the threshold for using the prone position. The infants might also belong to families with difficulties adhering to official recommendations and thereby with a higher prevalence of other risk factors. In these families, especially with infants with insomnia or intensive crying, it might be appropriate to reinforce the advice on the supine sleeping position.
We found a statistically significant difference in alcohol habits between the Western Sweden study and the Nordic Study. High alcohol use during pregnancy and high use after pregnancy both decreased. In a recent study in Sweden,15 it was found that approximately 30% of pregnant women reported regular alcohol use during pregnancy, but only 2/1101 (that is, 0.18%) reported drinking two to three times a week. This is in accordance with the figures from the Western Sweden study.
Alcohol figures must be viewed with caution since there is a high risk of under-reporting the use of alcohol in studies of this type.16,17 On the other hand, it is quite possible that under-reporting is higher when the pregnant woman is personally interviewed by her midwife, which is how official statistics concerning alcohol use in pregnancy are obtained.
The reason for the fall in vitamin A and D supplements is unclear.
Consideration must be given to the fact that the study design differed between the two studies. All the infants in the cohort from Western Sweden were 6 months old. The age of the control infants in the Nordic Study varied between 2 and 57 weeks, with a mean of 19 weeks. This age difference can certainly influence the prevalence of factors such as sleeping position, but the trend from prone to alternating side/supine and exclusively supine seen in the Western Sweden study was also demonstrable during the years of the Nordic Study.4 Direct comparison of breast feeding figures is also restricted by the control infants in the Nordic Study being on average younger than the infants in Western Sweden, but the finding of an unchanged prevalence is supported by official statistics.18
An important issue in comparing the data was the response rate. In the Western Sweden study, the response rate was 68.5% among parents of 6 month old infants. Considering that this study was population based, it is reasonable to compare it with the response of the controls in the Nordic Study, which had a 72% response rate. The Nordic Study found odds ratios for important risk factors similar to those calculated from data in the Medical Birth Registry.19 We have compared the prevalence of smoking during pregnancy (9.5%) in the Western Sweden study with recent statistics from the National Board of Health and Welfare, showing that 11.4% of all pregnant women in Western Sweden smoked in 2002 compared to 10.6% in Sweden as a whole. There is a trend towards a lower prevalence of smoking during pregnancy.20 We were concerned that families from disadvantaged backgrounds might be under-represented, but since smoking is linked with several disadvantageous factors, we believe that the data from Western Sweden are representative.
What this study adds
-
The decrease in SIDS incidence levelled out in 2000.
-
Prone sleeping and maternal smoking during pregnancy decreased between 1995 and 2004. Variants of side sleeping are still used by 44% of parents.
-
Prone sleeping is associated with a disadvantaged background or an infant with sleeping difficulties. Changing the sleeping position to exclusively supine and reducing smoking by pregnant women will further reduce the risk of SIDS.
In conclusion, we have shown that parents of infants have in general complied with advice given at infant welfare centres to prevent sudden infant death and that the information is still effective 10 years after it was first introduced. Additional gains can be made by changing the preferred sleeping position from side and side/supine to exclusively supine and reducing the number of pregnant women smoking. We have also found that sleeping position is associated with whether the mother is unemployed, whether she smokes, and whether the infant is irritable, never uses a dummy, or shares a bedroom with other children.
REFERENCES
Footnotes
-
Published Online First 7 February 2006
-
The Infants of Western Sweden study was supported by the Unit for Research and Development in the Western Sweden Region, the Faculty of Medicine, the Sahlgrenska Academy, Göteborg University, the Committee of Public Health in the Western Sweden Region, the Vårdal Foundation for Health Care Sciences and Allergy Research, and the Research Fund of the Swedish Asthma and Allergy Association
-
Competing interests: None declared.