Article Text

Abstract
Childhood obesity is increasing nationally and worldwide. Using the child's total body weight to calculate drug doses for certain medications could result in incorrect dosing. The aim of this study was to assess whether paediatric doctors have knowledge about prescribing correct doses of medications for obese children by using methods to calculate the ‘ideal body weight’ (IBW). A questionnaire was sent to paediatric doctors asking whether they understand IBW and how to calculate it using the McLaren method. The results suggested that most paediatric doctors did not determine whether a child was obese when calculating drug doses. There was relatively poor understanding about the concept of IBW and only 9% of paediatricians in this study knew how to calculate it. There should be more training and guidance about calculating IBW in obese children to avoid potentially toxic errors.
- Obesity
- Pharmacology
- Paediatric Practice
Statistics from Altmetric.com
Introduction
According to WHO, childhood obesity is one of the most serious global public health challenges for the 21st century.1 Childhood obesity is defined as a body mass index (BMI) at or above the 95th percentile for children and teens of the same age and sex.2 Recent data published by Public Health England confirm that in England 19.1% of year 6 school children are obese and another 14.4% are overweight.2 It is also recognised that increased fat and lean masses in obese children affect pharmacokinetics and the distribution of drugs in tissues.3 ,4 Using the child's total body weight (TBW) to calculate the dose, especially for drugs with a narrow therapeutic window, could potentially result in incorrect dosing in obese children. Therefore, it is recommended to use ideal body weight (IBW) to calculate the correct dose. The most commonly used method is the McLaren method.5
Background
This study was prompted by an incident of drug toxicity in an obese child where a very large dose of aminophylline was administered. The child developed severe vomiting and became quite unwell, so a review was carried out. It was then noticed that drug calculations were based on TBW, and had IBW been used, the dose would have been smaller and the overdose would most likely not have occurred.
Objective
The aim was to assess the level of understanding that paediatric doctors have about prescribing the correct doses of medications for obese children. This requires doctors to be aware that in obese children certain medications cannot be calculated using TBW and they must have knowledge about the methods used to calculate the IBW.
Methods
The study consisted of two parts. Part 1 explored whether local paediatric doctors recognised that a child was obese and then used their IBW as per British National Formulary for Children (BNFC) guidance to calculate drug doses correctly. Part 2 was a region-wide survey of paediatric doctors exploring their understanding of the concept of IBW and whether they took any special measures when calculating drug doses in obese children.
Part 1
A questionnaire was given to all paediatric doctors attending a departmental educational meeting. The grades of doctors attending were from Foundation Year 1 doctors up to consultants. The questionnaire contained four clinical scenarios about prescribing medicines for children. Each scenario gave the child's age, weight and height. The BMI was not given. All of the scenarios involved children who were obese (which would have been obvious if the BMI was calculated) and drugs (aminophylline, aciclovir, gentamicin, vecuronium) in which the recommendation was to use IBW. The participants were also given a BNFC (paper or electronic) and asked to prescribe a drug for each child, showing their working out. These results were collected and analysed in a spreadsheet, and compared with the correct answer as worked out using the McLaren method for estimating the child's IBW.
Part 2
An online questionnaire was sent out to all paediatric trainees and consultants in the region (West Midlands), asking four questions to determine whether they take into account the child's weight when prescribing for obese children, whether they understand the term ‘ideal body weight’ and also how to calculate it using the McLaren method. These results were collected and analysed in a spreadsheet.
Results
Part 1
The response rate was 100%. None of the respondents (0/15) gave any of the correct answers to the drug dosing questions, and no one calculated the child's BMI or their IBW. This was despite the BNFC clearly having a box highlighting the need to use IBW in each of these drug's sections. Most respondents correctly calculated the dose for the child's TBW (Q1 67%, Q2 100%, Q3 100%, Q4 87%). All of the answers given for each question were a higher dose than the correct answer, which was calculated using the child's IBW. This meant that all of the given answers would have been overdoses.
Part 2
There were 111 respondents to the online questionnaire, which consisted of 88 consultants (response rate 24%) and 23 trainees (response rate 9%) (ranging from ST1 to ST8) with a range of experience varying from 1 year to >35 years. Of the respondents, only 3% (3/111) calculated BMI and determined whether the child was obese for its age when prescribing medications. Also, 35% (38/111) of prescribers gave special consideration to the weight when calculating drug doses in obese children. And, 16% (17/111) of prescribers were familiar with, and understood, the terms TBW, IBW, adjusted body weight and lean body weight. Only 9% (10/111) of prescribers knew how to calculate IBW using the McLaren method.
Discussion and conclusion
IBW is the recommended weight to be used for dose calculations for certain drugs, especially those with a narrow therapeutic index. Although there are many methods for calculating IBW, there are three main ones.5 These are the McLaren method, the Moore method and the BMI method. Each method has advantages and disadvantages, and gives a slightly different answer, but the McLaren method is the most commonly used (see figure 1). In the Moore method, the participant's height-for-age percentile is determined, and the IBW is the weight that corresponds to that weight percentile. The BMI method is calculated as IBW=[BMI at the 50th percentile for that child's age× (height in m)2].5
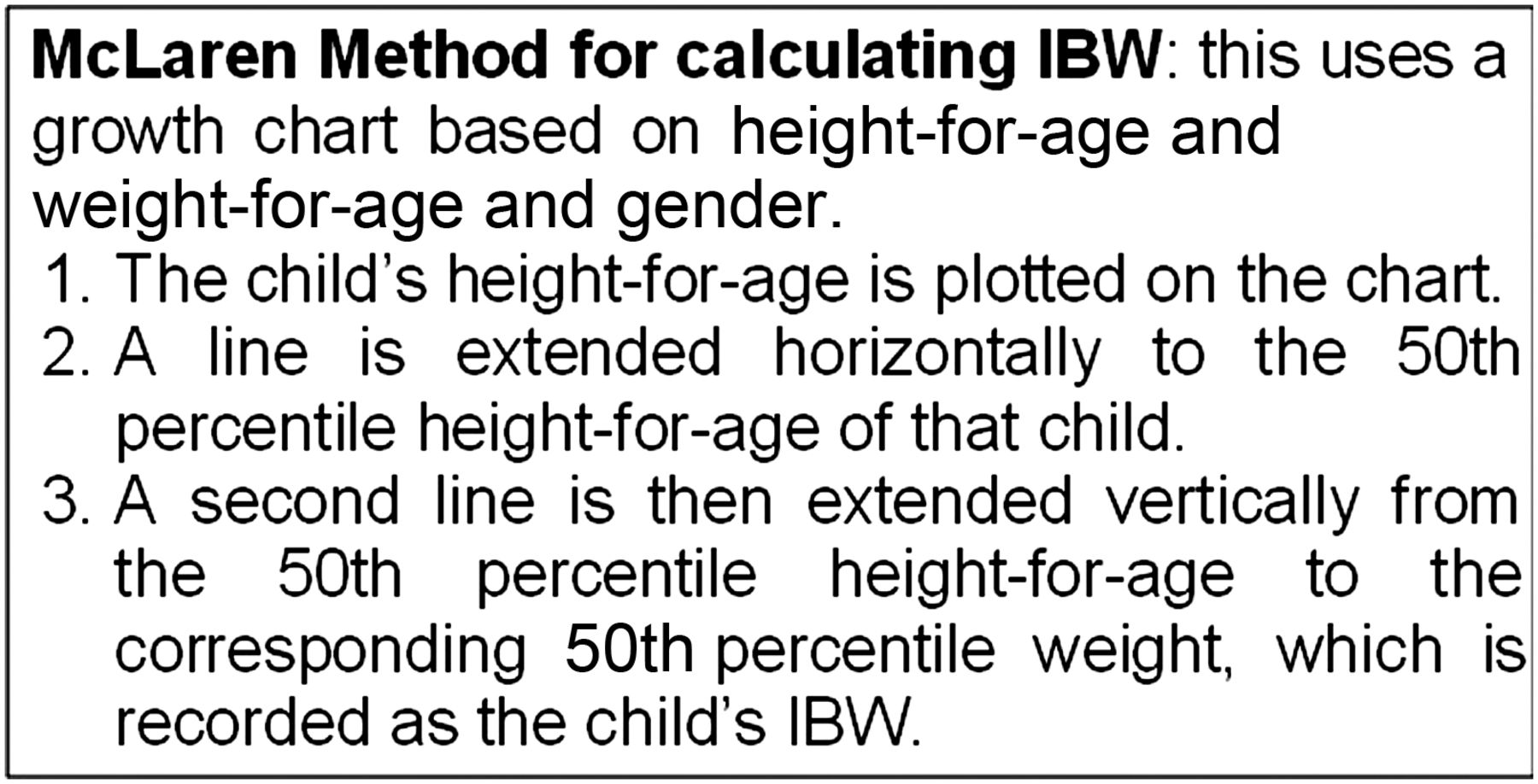
McLaren method. IBW, ideal body weight.
The findings from both parts of the study suggested that most paediatric prescribers did not ascertain whether a child was obese when calculating drug doses. There was relatively poor understanding about the concept of IBW, and paediatric doctors were not familiar with how to calculate it, suggesting that underdosing or overdosing in obese children was therefore more likely to happen.
These deficiencies should be addressed regionally and perhaps nationally by including relevant information in prescribing training for medical students and junior doctors. Locally, the prescribing education session for new paediatric trainees has been updated. A section was included on recognising obesity and guidance on using IBW. Furthermore, it must be considered that some existing paediatric doctors will need further training to ensure that the same practice is followed across the trust.
The BNFC highlighted which drugs need IBW estimation (see figure 2) and recommended using IBW for height. It does not, however, provide a method for calculating it. Therefore, the BNFC should include more guidance about calculating IBW in obese children to avoid potentially toxic errors. A copy of this report will be sent to the British National Formulary editorial team. This report will hopefully highlight the importance of paediatric prescribing training, especially with regard to obese children.

{kind=link}
{kind=link}
Drugs requiring IBW calculation. BNF, British National Formulary; IBW, ideal body weight.
Footnotes
Twitter Follow Maria Nasim at @Maria89_2
Contributors HC was responsible for review of literature, devising the questionnaire, collecting and analysing the data, drafting the article. AG was responsible for conceiving the idea, review of literature, devising the questionnaire, drafting the article. MN was responsible for contributing to development of a practice improvement plan in response to the survey results and undertaking responsibility for this locally.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement We are happy to share all the collected data, which has been summarised in the article.