Article Text

Abstract
Background Outcome data for surgery in paediatric Crohn's disease are limited. We report 10 years’ experience at a regional paediatric gastroenterology centre.
Methods Children undergoing surgery for Crohn's disease (January 2002–December 2012) were identified from an onsite patient register. Patients were followed until transition to adult services. Data were obtained from medical records and are expressed as median (range).
Results Sixty-nine children, aged 13.8 years (6.3–17.0) at diagnosis, were included. 42 were male (61%). Follow-up was 1.8 years (27 days–6 years). Surgery followed diagnosis by 9 months (0 days–7 years). 52 children (75%) received thiopurines and 5 (7%) anti-TNF (tumour necrosis factor) therapy preoperatively. 58 (84%) underwent intra-abdominal surgery (40 right hemicolectomy, 8 stoma formation, 2 subtotal colectomy, 2 small bowel resection, 6 other) and 10 (14%) underwent surgery for perianal disease. The commonest indications for intra-abdominal surgery were stricturing disease 35 (60%) and unresponsive luminal disease 13 (22%). There were 13 (22%) early, and 5 (8.6%) late, complications following intra-abdominal surgery. Nine children had disease relapse, five required further surgery. Height SD scores (SDS) did not increase between diagnosis; −0.5 (−3.4–2.1) and most recent follow up; −0.4 (−3.0–1.1). Body Mass Index (BMI) SDS increased from −1.0 (−6.3–1.5) to −0.3 (−3.3–2.0) (p<0.05).
Conclusions Surgery was associated with a 22% early complication rate and a 15% risk of relapse. 21% of patients required a second unplanned intra-abdominal procedure. Surgical intervention was associated with an increase in BMI SDS, but not in height SDS.
- surgery
- ileocaecectomy
- outcomes
- paediatrics
Statistics from Altmetric.com
What is already known on this topic
-
The frequency of Crohn's disease in the paediatric population is increasing.
-
Paediatric Crohn's disease is associated with a high lifetime risk of surgical intervention.
-
Surgical outcome data is limited.
What this study adds
-
In a large regional centre, intra-abdominal surgery is associated with a 29% risk of complications and a 15% risk of relapse before transition to adult services.
-
The risk of an unplanned second intra-abdominal procedure before transition to adult services is 21%.
-
Surgical intervention is associated with an increase in Body Mass Index SD scores (SDS) but not in height SDS.
Introduction
Crohn's disease is associated with significant morbidity and is being diagnosed with increasing frequency in the paediatric population.1 ,2 In the UK, prospective data show the incidence to be 5.2 per 100 000 individuals per year,3 with an even distribution between ileitis, colitis and ileocolitis.4 The classic triad of abdominal pain, weight loss and diarrhoea is present in only 25%.4
The lifelong risk of surgery is high, with as many as a third of patients requiring surgical therapy within 5 years of diagnosis.5 ,6 The high rate of relapse following surgical treatment, and the likelihood of second surgical procedures being required7 mean that surgical management of Crohn's disease is often regarded as a ‘last resort’ treatment, with a view taken that it is only appropriate when medical treatment has failed or is unlikely to be successful.
Despite the frequency of surgical therapy in children with Crohn's disease, there is a paucity of publications reporting outcomes, with evidence limited to relatively small, retrospective, single-centre series,7–9 those containing data from well before modern medical therapy was available10 and several describing the results of minimal access techniques.11 ,12 Nevertheless, there is a recognition that surgery for Crohn's disease is associated with a high rate of surgical morbidity, with reported long-term complication rates of up to 77%.7
Over recent years, childhood Crohn's disease in our region has been increasingly managed at our regional referral centre by a specialist team of paediatric gastroenterologists and paediatric surgeons, rather than in district general hospitals. We have accumulated a large institutional experience over the last 10 years, in the context of the centre serving a population of three million, and 10 general hospitals with 50–60 new cases of inflammatory bowel disease presenting each year. We, therefore, undertook a review of our surgical experience in order to report outcomes.
Materials and methods
Patients under 18 years of age undergoing surgery for Crohn's disease in our unit between January 2002 and December 2012 were identified from a prospectively collected departmental database. Patients’ medical management favoured exclusive enteral nutrition over corticosteroids, immune suppression was used as indicated.13 All patients were investigated using standard criteria (Porto).14 We excluded patients who were not diagnosed and managed exclusively at our regional paediatric gastroenterology unit. Patients with indeterminate colitis were excluded. Decisions about surgical intervention were made by a multidisciplinary team including specialist paediatric gastroenterologists, radiologists and paediatric surgeons. All patients undergoing elective intra-abdominal surgery underwent preoperative barium follow-through. MRI scans were used with increasing frequency during the later part of this experience.
Surgery was undertaken by six specialist paediatric surgeons; two surgeons with an interest in Crohn's disease undertook the majority of the elective operations. The operation performed and the use of laparoscopic techniques was at the discretion of the individual surgeon.
Data were collected from patient records using a standardised proforma. The site of disease at presentation, preoperative and postoperative medical therapy and details of surgical procedures performed were recorded. Height and weight at diagnosis, postoperatively and at latest follow-up were also documented. Early complications were defined as those occurring during the admission in which surgery was performed. Late complications were defined as those occurring after discharge from hospital. Data proformas were verified by a second author.
Data were collated into a Microsoft Excel spreadsheet. Date of diagnosis was taken as the date at which histological confirmation of the disease was made. Height, weight and Body Mass Index (BMI) were converted to SD scores (SDS) using the UK 1990 Growth standards15 by means of the LMS growth programme (Harlow Healthcare, South Shields, UK http://www.healthforallchildren.co.uk). Growth data were compared using a Mann–Whitney U test, with significance considered at p<0.05.
A Pubmed literature search was used to identify studies reporting the outcomes of surgery for paediatric Crohn's disease within the last 10 years. The search terms: Crohn's disease, surgery, child and paediatric/pediatric were used.
Approval was given by local research and development office; ethical board opinion was not required. Results are reported as median (range).
Results
The database contained 286 patients diagnosed with Crohn's disease during the study period, of whom 69 underwent surgery (24%). Procedures performed are summarised in table 1. Intra-abdominal procedures were performed in 58 (84%). Median age at diagnosis was 13.8 years (6.3–17 years). Fifty-seven of 69 patients had ileal involvement at diagnosis, of whom 36 had ileocolic disease.
Table summarising the surgical procedure performed as the primary intervention in this study cohort
Preoperative therapy
Seven of 69 patients had the diagnosis of Crohn's disease made on the day of surgery. Of these, two presented with bowel obstruction, one with a mass, one with a symptomatic stricture, two with anal fistulas, and one with penile Crohn's.
Of the remaining 62 patients, exclusive enteral nutrition with Modulen IBD was commenced at diagnosis in 53 (86%). Thiopurines were used preoperatively in 52 patients (85%) and steroids in 37 patients (60%). Monocloncal anti-TNF therapy (Infliximab) was used in five patients (8%).
Indications for surgery
Extra-abdominal procedures
Ten of the 69 patients underwent surgery for perianal disease. The indications were perianal fistula (5), fistula associated with a perianal abscess (2), a simple perianal abscess (1), vulval abscess with an associated fistula (1) and skin tags treated by excision (1). Two patients with perianal fistulas underwent an MRI scan prior to surgery to define the anatomy. Therapy consisted of an examination under anaesthetic, and a placement of a non-cutting seton suture (8), incision and drainage (1) and excision of skin tags. A seton suture is a rubber sling passed through the fistula track and out through the anus with the intention of allowing healing of the fistula without laying it open, and is employed for fistulas whose tracks pass superior to the anal sphincters. The intention was to leave setons in place until complete resolution of the fistula had occurred. Of eight setons placed during the study, five were removed following resolution of the fistula (63%). The remaining three patients all had the seton in place at transition to adult services or the end of the study period. None of the patients with a perianal fistula were treated with Infliximab during the study period, although one patient has subsequently received it. No patients required a stoma for perianal disease, and no advancement flaps were required for reconstruction.
One patient underwent surgery for penile Crohn's disease.
Intra-abdominal procedures
The remaining 58 patients underwent surgery for intra-abdominal disease. The most common indication for surgery was stricturing disease (35 patients). The indications for surgery are summarised in figure 1.

Flow diagram summarising the indications for surgery, and preoperative therapy in this study cohort.
Timing of surgery
Surgery was undertaken at a median of 274 days following diagnosis (−53 days–6.9 years). One patient underwent their first surgical procedure (incision and drainage of a perianal abscess) 53 days before diagnosis. The timing of abdominal operations relative to diagnosis is shown in figure 2. Patients undergoing a second abdominal procedure underwent surgery at a median of 280 days (4 days–6 years). Figure 3 illustrates the risk of further procedure being required at each interval of follow-up for the study cohort.

Histogram showing the number of patients undergoing intra-abdominal surgery in each 3-month interval following diagnosis.
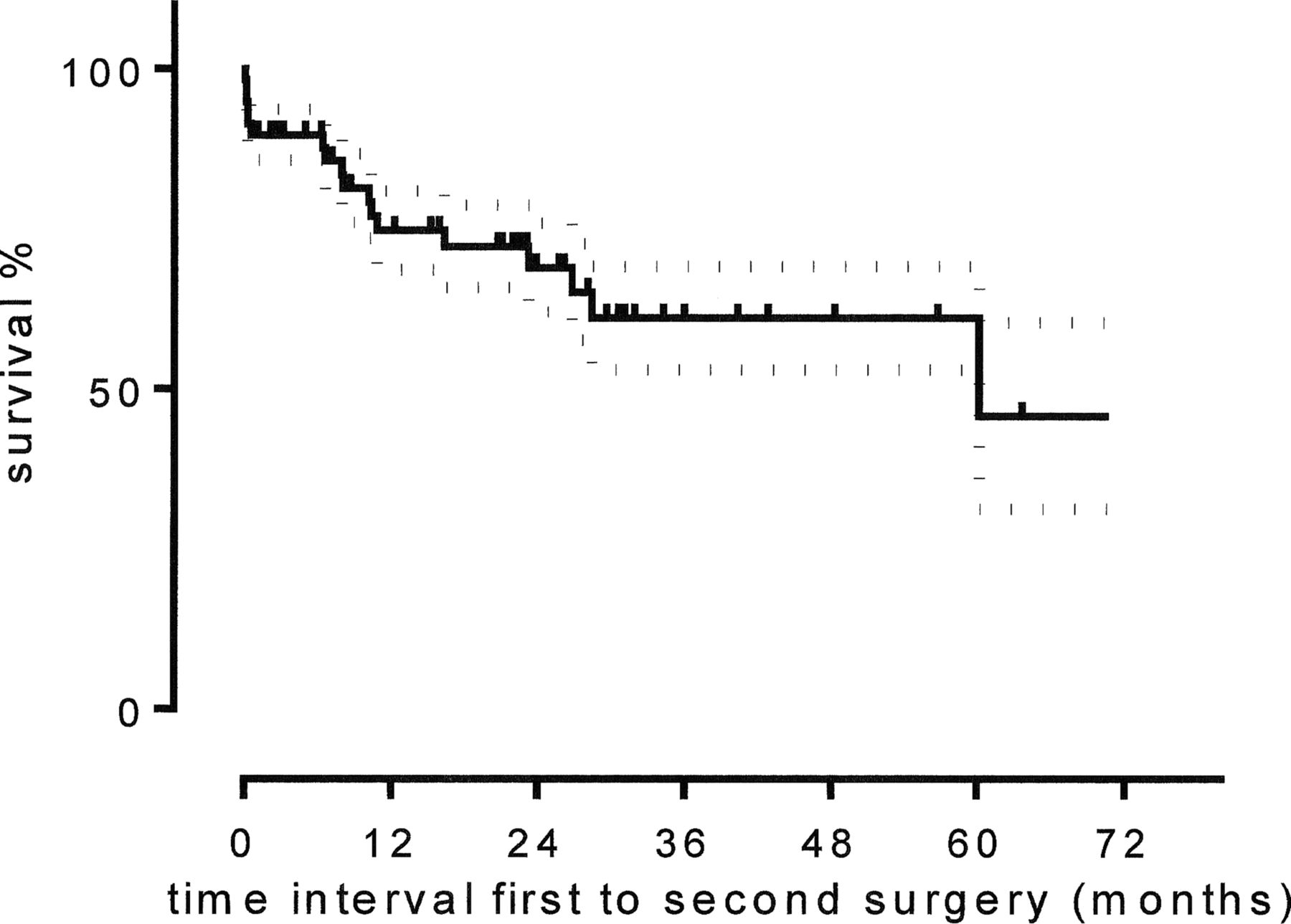
Kaplan–Meier survival curve demonstrating risk of further intra-abdominal surgery being required at each time interval during follow-up. Dashed lines are the SE of the mean, vertical lines are censored data.
Intra-abdominal procedures (N=58)
The majority of patients underwent right hemicolectomy. Surgical procedures performed are summarised in table 1. Forty-nine patients underwent a bowel resection, with a median length of resection of 23 cm (2–50 cm). Of these, 42 patients underwent a primary anastomosis and seven had a stoma formed. Complete macroscopic resection of Crohn's disease was achieved in 42 patients. Microscopic pathology was examined in all patients undergoing right hemicolectomy (40 patients). Of these, 18 had no evidence of disease at the resection margin, 17 had evidence of disease at the resection margin. No comment was made in the remaining 5. No difference in outcome was observed between these groups.
Ten abdominal operations were started using a laparoscopic-assisted approach, with the bowel mobilised intra-abdominally and an extracorporeal resection and anastomosis performed. Of these patients, three required conversion to a formal laparotomy because of an adherent mass which was not amenable to laparoscopic mobilisation. All three of these patients required a stoma.
No strictureplasties were performed in this series.
Postoperative course
In patients undergoing intra-abdominal surgery, oral fluids were restarted on the second postoperative day (1–14 days), and diet was started on the fourth postoperative day (1–15 days). Length of stay was 6 days (1–55 days).
The majority of patients (63, 91%) were recommenced on thiopurine medication in the immediate postoperative period, and six required treatment with biologic agents (Infliximab in all patients).
Complications of intra-abdominal procedures
Overall, 17 patients had at least one complication of their surgery (29%). Thirteen patients experienced an early complication (22%). Seven (12%) patients had a postoperative infection. An anastomotic leak occurred in four patients, representing 9.5% of the 42 patients in whom a primary anastomosis was performed. One leak followed a laparoscopic resection. One patient had postoperative bleeding requiring further surgery.
Late complications occurred in five (8.6%) patients. Adhesional obstruction occurred in two and there was one anastomotic stricture which was successfully treated with balloon dilatation complicated by an episode of bleeding.
Two patients had a prolonged postoperative course with dependence on parenteral nutrition. Both had significant additional comorbidities. One of these patients experienced posterior reversible encepholophathy syndrome following a transfusion (resolved), and the other a haemophagocytic lymphohistiocytosis-type syndrome (resolved).
Recurrence and further surgery
Seven of 58 (12%) patients required further unexpected intra-abdominal surgery to treat complications of their initial operation, rather than for disease relapse or to close a stoma.
Nine patients (16%) who had undergone abdominal surgery had relapse of their disease following surgery, within a median follow-up of 1.8 years (27 days–6 years), of whom five required further surgery. Relapse was diagnosed at a median of 273 days following surgery (56 days–5.7 years).
In total, 12 children (21%) required a second unplanned intra-abdominal procedure. Figure 3 shows time from first to second surgery for all (unplanned and planned) procedures.
Height and weight
Height and weight SDS at diagnosis, in patients undergoing intra-abdominal surgery, revealed a low median height; SDS −0.5 (−3.4–2.1). BMI was also low; SDS −1.0 (−6.3–1.5). Fifteen children had a BMI SDS <−2. At follow-up, a median of 1.8 years (27 days–6 years) after surgery, height SDS was −0.4 (−3.0–1.1), and BMI SDS −0.3 (−3.3–2.0). At this point, only three children had BMI SDS <−2. BMI SDS significantly improved between preoperative and postoperative measurements (p<0.01), but height SDS did not (p=0.70; figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scatter plot demonstrating patients’ height SD scores (SDS) and Body Mass Index (BMI) SDS at diagnosis, and at latest follow-up for patients in the study cohort. Height SDS was not significantly increased, but BMI SDS was. (*p<0.05, Mann–Whitney U Test).
Discussion
These data reflect the experience of a regional centre over a 10-year period, representing one of the largest paediatric series of surgically managed Crohn's disease reported in the literature to date. The age at presentation (13.8 years) and disease location at diagnosis are both in keeping with previous literature.3 ,4 Intra-abdominal surgery most commonly involved a right hemicolectomy to treat stricturing disease at the ileocaecal valve.
Intra-abdominal surgery in this cohort was often performed early in the course of disease, with a median interval from diagnosis to intervention of 9 months. This compares with other studies reporting a range of 14.5 months to 3 years (table 2).8–12 16–21
Table summarising the results of studies published in the last 10 years which report outcomes of surgery for children with Crohn's disease (NR=not reported)
The overall complication rate of 20% in those patients undergoing intra-abdominal surgery is consistent with other published series (table 2). Those series reporting lower rates of complication record only the results of selected patients undergoing laparoscopic bowel resection. Our leak rate of 9% is also in line with previous series, with one study reporting a leak rate as high as 19%.7
The rate of 16% relapse at a median follow-up of 1.8 years in this series is also consistent with that reported in the literature to date (table 2), although this is less well documented in surgical studies. These figures should, however, be interpreted in the long-term context; rates of further surgery at 10 years of 29% to 54% have been reported.7 ,18
Growth delay is recognised as a common complication of Crohn's disease in the paediatric population,22 and a mean height deficit of −0.5 SDs at diagnosis has been reported.23 Our data are consistent with these observations, with a median height SDS of −0.5 and a BMI SDS of −1. At latest follow-up, our cohort of patients has a significant improvement in BMI SDS, but not in height SDS. A short-term increase in height velocity after surgery for Crohn's disease in adolescence is well recognised.19 ,24 Interestingly, epidemiological data suggests a growth advantage of early surgery; with a recently published cohort of patients demonstrating better catch-up growth in patients operated on within 3 years of diagnosis.18 However, in long-term follow-up, surgery is not associated with greater improvements in height than medical therapy.20
Additionally, patients undergoing resection within 1 year of symptom onset have demonstrated a delay in recurrence of disease (30% by 8 years v 50% by 4 years).18 This conclusion is supported by the findings of Griffiths et al21 who demonstrated a reduced recurrence rate in patients undergoing surgery within a year of diagnosis.
Preoperative therapy most commonly involved thiopurines and Modulen. Infliximab before surgery was used in a small number of patients. This may reflect the historic nature of this cohort; in the early 2000s, biologic use was not widespread because of concern about an association between the use of these agents and hepatosplenic T-cell lymphoma.25 When looking at this cohort of patients, therefore, the question of whether surgery could have been delayed or prevented by the use of biologic agents is raised. Around 25% of paediatric patients with Crohn's disease, however, will present with stricturing disease.5 In this subset of patients, it is likely that there will develop ‘burnt out’ fibrotic strictures, evidenced by prestenotic dilatation on imaging, which are unlikely to resolve with medical treatment, and more intensive medical therapy may only delay, rather than avoid surgery.
Despite this, it is possible in this cohort of patients that the use of Infliximab might have prevented the formation of strictures later in the course of the disease, or prevented the failure of medical management. The use of Infliximab in children has, however, been associated with a delay in surgery rather than its avoidance.26 An additional issue in relation to the use of biologic agents in young patients with Crohn's disease is the development of antibodies to these medications, and subsequent treatment resistance.27 An argument exists, therefore, that one advantage of surgical therapy is the maintenance of treatment naivety, retaining a useful therapeutic option in the future.
Data from this study is limited due to its retrospective nature. The use of our non-surgically managed patients as a comparative group might have been informative, but this study was deliberately focussed on outcome of our surgical patients who were exclusively managed in our centre, whereas, our departmental database contains the records of all patients with Crohn's disease in whose management we are involved.
Conclusions
We report a large single-centre experience of surgery for childhood Crohn's disease, with an earlier use of surgical therapy than has been described in previous series. Surgery for Crohn's in our centre is associated with a 29% risk of a complication and a 21% risk of further unplanned intra-abdominal surgery before transfer to adult services (9% for relapsed disease and 12% for a complication of the original operation). The risk of relapse is 15% before transfer to adult services. Surgical therapy for Crohn's disease is associated with an improvement in BMI SDS but no significant improvement in height SDS. In the context of decisions taken by a multidisciplinary team, however, surgery remains an important therapy for Crohn's disease, and should not be seen as a treatment of last resort.
References
Footnotes
-
Contributors RMB and MPS conceived the study, which was then designed with contributions from all authors. All authors collected the data, which was then analysed by SCB and AEW. The manuscript was written by SCB, AEW, RMB and MPS. All authors approved the manuscript before submission
-
Competing interests None.
-
Ethics approval Local research and development office.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Further data from this study are available from the authors on request.