Article Text

Abstract
Objective Most primary care clinical guidelines recommend restrictive antibiotic use for childhood infections. We investigated antibiotic prescription rates over time for oral and topical antibiotics for children (≤12 years) in the period 2000–2010.
Design, setting and patients Longitudinal observational study among children (≤12 years) in a large Dutch general practice database in the period 2000–2010.
Main outcome measures Oral and topical antibiotic prescribing rates per year and independent factors influencing antibiotic prescriptions.
Results We analysed 108 555 patient-years during 2000–2010. At least one chronic disease was recorded in 15.8% of patient-years, with asthma most commonly registered. In 14.8% of the patient-years at least one antibiotic was prescribed, while 26.3% of these received two or more prescriptions. Young age and chronic disease had a significant effect on antibiotic prescriptions. Prescriptions for oral and topical antibiotics increased 4.9% and 1.8%, respectively, during 2000–2005 (p<0.001). Prescription rates for oral antibiotics decreased 3.3% during 2006–2010 (p<0.001), while topical prescribing rates remained stable.
Conclusions One in six children received at least one oral antibiotic prescription per year during 2000–2010. While topical prescription rates steadily increased during 2005–2010 and remained stable during 2006–2010, prescription rates for oral antibiotics increased significantly during the period 2000–2005 and then significantly decreased during the period 2006–2010. As clinical guidelines remained the same over this period, the effects could be contributed to the initiation of the Dutch nationwide pneumococcal vaccination campaign in 2006.
- Antibiotics
- Children
- Primary Care
Statistics from Altmetric.com
What is already known on this topic
-
The majority of antibiotics for childhood infections are prescribed in primary care.
-
Prudent antibiotic use is promoted in most primary care clinical guidelines for childhood infections in an attempt to contain antibiotic resistance.
-
There are limited studies investigating trends in oral antibiotic prescription rates for children in general practice and no studies looking at topical antibiotic prescribing rates.
What this study adds
-
One in six children received at least one oral antibiotic prescription per year during 2000–2010.
-
Prescription rates for oral antibiotics first increased during 2000–2005 and then decreased during the period 2006–2010.
-
Topical antibiotic prescribing rates increased during 2000–2005 and then remained stable.
Introduction
In most developed countries the majority of antibiotics for childhood infections—including infections of the respiratory tract (as well as ear infections), urinary tract and skin—are prescribed in primary care.1 Consultations for symptoms related to childhood infections constitute an extensive workload for general practitioners (GPs) in which they are often faced with difficult decisions on the necessity of antibiotic treatment. While most respiratory infections are self-limiting, a small minority of children have a serious infection with a complicated course if left untreated. Clinicians’ diagnostic uncertainty combined with parental worries and expectations may lead to overuse and misuse of antibiotics. This can contribute to antibiotic resistance in the community and unwanted drug-related side effects. In addition, parents receiving antibiotics after an initial consultation at which antibiotics were not prescribed were less satisfied with care.2
Prudent antibiotic use is promoted in most primary care clinical guidelines for childhood infections, including those issued by the Dutch College of GPs, in an attempt to target antibiotics at those children who need them and to contain antibiotic resistance. However, there are limited studies investigating trends in oral antibiotic prescription rates for children in general practice. The current available evidence shows that countries with the highest paediatric prescription rates like Italy and Canada have a fourfold higher rate than countries with lower prescription rates like Denmark.3 The Netherlands generally range among the lowest prescribing countries in studies comparing overall outpatient antibiotic prescribing. Yet, besides limited evidence on antibiotic prescribing in children, until now there are no studies on GP prescribing of topical antibiotics. This is striking as topical antibiotics are frequently used for common paediatric skin and eye infections in general practice.4 Monitoring trends in antibiotic prescribing is important to assess the necessity of interventions aimed at antibiotic use for the paediatric population.
In this paper, we investigate prescription rates over time and for different age categories for oral and topical antibiotics among children (≤12 years) in the period 2000–2010 using data from a large GP database.
Materials and methods
We retrieved data from the Dutch Registration Network Family Practices (RNH) in 2000–2010 from children (≤12 years). The RNH is a continuous, computerised and anonymous database from 22 rural and urban general practices in the south of The Netherlands, Limburg.5 The RNH contains information on patient demographics, diagnoses and medication prescription (coded according to the Anatomical Therapeutical Chemical, or ATC classification, from WHO). Diagnoses are registered according to the International Classification of Health in Primary Care and the current Dutch guidelines. Diagnoses are registered as chronic diseases when they are permanent, recurrent, or when they have lasting consequences for the functional status or prognosis of the patient.6
We included the following chronic diseases that were considered to be relevant for children and antibiotic prescriptions: leukaemia (B73), chronic bronchitis (R91), asthma (R96), diabetes mellitus (T90), constitutional eczema (S87), congenital disorders (A90, D81, H80, R89 and U85) and hypertrophic/chronic infections tonsils/adenoid (R90). ATC code J01 was used for all systemic (oral) antibacterial medication (excluding antifungal or tuberculosis medication) with the following classes: tetracyclines (J01A), β-lactam antibiotics, including penicillin (J01C), other β-lactam antibiotics (J01D), sulphonamides and trimethoprim (J01E), macrolides (J01F), aminoglycosides (J01G), fluoroquinolones (J01MA), other quinolones (J01MB), nitrofurantion (J01XE), metronidazole (J01XD), and other systemic antibiotics (J01XX). Finally, D06AX was used for antibiotics for topical use. Current Dutch guidelines for children indicate that there is no indication to prescribe antibiotics from the following specific groups: aminoglycosides (JO1G), (fluor)quinolones (J01MA/B), tetracyclines below the age of 9 years (J01A) and systemic antibacterials other than mentioned in the classes above.
The unit of analysis was patient-year, that is, a patient contributes one patient-year when he or she is registered as a patient at an RNH participating general practice. The annual prescription rate was defined as the number of prescriptions (maximum of one per patient per year) divided by the number of patient-years in a given calendar year. Using multivariate logistical regression analyses, time-trends for annual prescription rates were evaluated controlling for age, gender and chronic disease. Using interaction-terms between year and other determinants, it was assessed whether time-trends were similar or different for specific age groups or other subpopulations. Analyses were performed with the SPSS package V.14.0.2 (SPSS Inc, Chicago, Illinois, USA).
All patients included in the RNH database were informed about the potential anonymous use of their health information. All data in this study are analysed anonymously, and are explicitly not retraceable to individual patients.5 ,6 This study was approved by the Medical Ethics Committee of the Maastricht University Medical Centre (reference number NL12-4-053).
Results
The study population comprised a total of 108 555 patient-years equally distributed across age and gender in the period 2000–2010. At least one chronic disease was recorded in 15.8% of patient-years with asthma (47%) being most common, followed by constitutional eczema (46%) and hypertrophic/chronic infections tonsils/adenoid (11%).
In 14.8% (n=16 091) of the patient-years at least one oral antibiotic was prescribed. In one out of four of these patient-years (26.3%; n=4229) two or more oral antibiotics were prescribed. In 5.3% (n=5797) of the patient-years at least one topical antibiotic was prescribed.
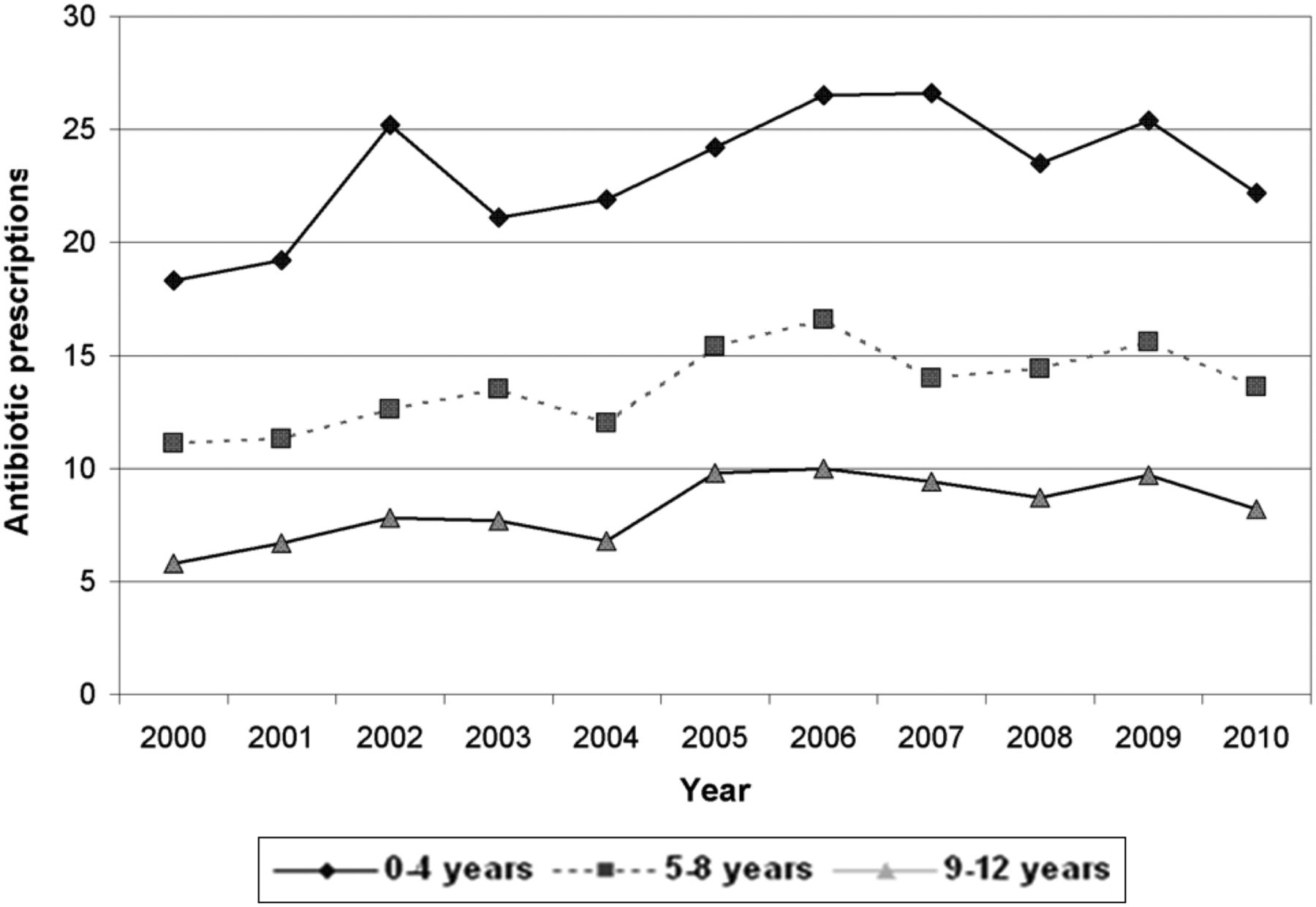
During 2000–2005, a significant increase of 4.9% (p<0.001) in the prescription rates was observed for both systemic and topical antibiotics (figure 1). Conversely, between 2006 and 2010 an average decline of 3.3% (p<0.001) in the oral antibiotic prescription rates was noted, varying from 4.3% in children aged 0–4 years, 3.0% in children aged 5–8 years and 1.8% in children aged 9–12 years (figure 2). Topical antibiotic prescription remained stable between 2006 and 2010. Table 1 shows factors associated with antibiotic prescriptions.
Multivariate analysis of factors influencing oral antibiotic prescriptions

Prescription rate (%) for topical and oral antibiotics 2000–2010.
{kind=link}
{kind=link}
Oral antibiotic prescription rate (%) per age category from 2000 to 2010.
The percentage of oral prescriptions decreased significantly with age (p<0.001), ranging from 27.7% for 1-year-olds to 6.2% for 12-year-olds. However, we observed a significant interaction between age and gender (p<0.001). In the youngest category boys received more antibiotics, and in the older categories girls received more antibiotics. Furthermore, patients with a recorded chronic disease received more antibiotic prescriptions (18.3%) than in those without a recorded chronic disease (14.2%, p<0.001).
The most frequently described antibiotic drugs were penicillin (86%), followed by macrolides (18%) and trimethoprim (3%) (table 2). Antibiotics for which there is no indication in children in general practice were only incidentally prescribed. For example, in the whole cohort fluoroquinolones were prescribed only 22 times in total to children of different ages and tetracyclines were prescribed only 11 times to children younger than 9 years in the years 2000–2010.
Top five prescribed oral antibiotic groups
Discussion
This large paediatric cohort study shows that almost one in six children received at least one oral antibiotic prescription per year during the period 2000–2010. Of these children one in four received two or more antibiotic prescriptions in a year. We observed a steadily significant increase in prescriptions during the period 2000–2005. However, during the period 2006–2010, a slight but significant decrease in prescriptions for oral antibiotics was observed.
Although Dutch data are limited, one study also showed a increase in prescriptions based on two point estimates from 1987 and 2001 in a cross sectional survey among GPs.7 Another study based on pharmacological database from 1999 to 2005 showed a slightly higher overall prescription rate of 17.8% and did not show an increase over time during the period 1999–2005. However, this study also included adolescents and was not limited to GPs prescriptions.8 An important factor that may have influenced Dutch prescription rates from 2006 onwards is the implementation of the pneumococcal vaccination. All infants in The Netherlands, born after March 2006, received the heptavalent pneumococcal conjugate vaccine at the age of 2, 3, 4 and 11 months to protect them against pneumococcal infections (since spring 2011 10-valent vaccine). A recent Norwegian study showed that implementation of this vaccine led to a reduced incidence of respiratory tract infections and acute otitis media.9 A similar trend may have occurred in The Netherlands contributing to the reduction in prescription rates from 2005 to 2010 we observed. A recent Dutch study on invasive pneumococcal disease also showed a strong decrease in vaccine serotype pneumococcal disease.10 The decrease in prescription rates in older age categories who were not vaccinated may be explained by the so-called ‘herd immunity’ effect, as was also observed in previous studies in the USA.11 ,12
Another notable finding was that in the youngest age category boys received more antibiotics than girls, while this was reversed in the older age categories. This was observed in earlier studies as well, and is potentially caused by a higher incidence of respiratory infections in boys during early childhood. The underlying mechanism for this difference has however not been disentangled.7 ,9 ,13
Prescription rates were significantly higher in children with a chronic disease, of which asthma was the most common. This could be explained by the fact that children with asthma are more prone to respiratory infections. However, it could also implicate that in cases of often self-limiting respiratory infections GPs tend to prescribe more antibiotics in children with comorbidity of asthma. Previous studies have however shown that in these patients earlier treatment with antibiotics does not improve their recovery or risk of complications.14 Still, since the prescription rates in our database are not linked to consultations—being the major limitation of our data source and thus our study—we can only make assumptions.
Finally, results show that GPs seldom prescribe antibiotics for which there is no indication in general practice. For example, the use of tetracyclines in children younger than 9 years of age is contraindicated and prescribed only 11 times in our study. Previous studies showed prescription rates for tetracyclines that were similarly to the findings in our study.7 ,15 As expected according to guidelines, penicillin was the most frequently prescribed oral antibiotic group. Furthermore, the most frequently described and preferential topical antibiotic in The Netherlands is fusidic acid.
This is the first and only study over a period of 10 years which is based on actual GP prescription data to children. Other studies were based on general pharmacological databases or limited to specific diseases or indications. Moreover, this is the first study that provides information on topical antibiotic prescription rates, which is relevant as topical antibiotics are frequently used for common paediatric skin and eye infections in general practice. The key strength of this study is the long study period and the large, representative study population. Reliability of the data is high due to the fact that the database is computerised and GPs and other users of the database are trained on a regular basis. The RNH database has a comparable sociodemographical character to the Dutch population; therefore, the data are highly generalisable.5 This study does however have some limitations. As previously stated, the most important limitation is that the database does not allow us to match prescription data to diagnostic labels. Another study based on The Netherlands Information Network of General Practice and limited to ear, nose and throat problems stated that incidence rates, antibiotic prescriptions and referrals of common ear, nose and throat problems remained stable in a period from 2002 to 2008.16 On the contrary, another recent study showed that primary care rates in consultations for respiratory tract infections increased considerably from 1995 to 2005.17 An increased consultation rate could attribute to the increased prescription rates we observed from 2000 to 2005, and this should be taken into account when cautiously trying to frame these results in the existing literature.
In summary, this study showed that oral ntibiotic prescription rates significantly increased during the period 2000–2005 and significantly decreased during the period 2006–2010 for all age categories of children <12 years. Moreover, we presented that in 5.3% of the patient-years at least one topical antibiotic was prescribed. With no existing data on topical antibiotic prescribing rates in children, this finding calls for international comparison.
Acknowledgments
The authors would like to thank Alfons Schroten for data support and the GPs of the RNH practices.
References
Footnotes
-
Contributors JC conceived the idea for the study. EB performed the data analysis and wrote the first draft of the manuscript. All authors (EB, IL, NDM, CB, CJH, GD and JC) interpreted the data and findings and all authors commented on the first draft and all further revisions. The corresponding author (EB) had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. EB and JC are the guarantors for the overall content of this study.
-
Funding None.
-
Competing interests None.
-
Ethics approval Maastricht University Medical Centre (ref. number NL12-4-053).
-
Provenance and peer review Not commissioned; externally peer reviewed.