Article Text

Abstract
Objective To review the aetiology and antibiotic resistance patterns of community-acquired sepsis in developing countries in infants where no clear focus of infection is clinically identified. To estimate the likely efficacy of WHO's recommended treatment for infant sepsis.
Design A systematic review of the literature describing the aetiology of community-acquired neonatal and infant sepsis in developing countries. Using meta-analytical methods, susceptibility was determined to the antibiotic combinations recommended by WHO: (1) benzylpenicillin/ampicillin and gentamicin, (2) chloramphenicol and benzylpenicillin, and (3) third-generation cephalosporins.
Results 19 studies were identified from 13 countries, with over 4000 blood culture isolates. Among neonates, Staphylococcus aureus, Klebsiella spp. and Escherichia coli accounted for 55% (39–70%) of culture positive sepsis on weighted prevalence. In infants outside the neonatal period, the most prevalent pathogens were S aureus, E coli, Klebsiella spp., Streptococcus pneumoniae and Salmonella spp., which accounted for 59% (26–92%) of culture positive sepsis. For neonates, penicillin/gentamicin had comparable in vitro coverage to third-generation cephalosporins (57% vs 56%). In older infants (1–12 months), in vitro susceptibility to penicillin/gentamicin, chloramphenicol/penicillin and third-generation cephalosporins was 63%, 47% and 64%, respectively.
Conclusions The high rate of community-acquired resistant sepsis—especially that caused by Klebsiella spp. and S aureus—is a serious global public health concern. In vitro susceptibility data suggest that third-generation cephalosporins are not more effective in treating sepsis than the currently recommended antibiotics, benzylpenicillin and gentamicin; however, with either regimen a significant proportion of bacteraemia is not covered. Revised recommendations for effective second-line antibiotics in neonatal and infant sepsis in developing countries are urgently needed.
- Tropical Paediatrics
- General Paediatrics
- Neonatology
- Infectious Diseases
- Microbiology
Statistics from Altmetric.com
What is already known on this topic
-
Sepsis in neonates causes about half a million deaths per year.
-
WHO recommends penicillin/ampicillin and gentamicin as treatment for neonatal sepsis.
-
Many countries use third-generation cephalosporins to treat neonatal and infant sepsis.
What this study adds
-
The commonest causes of neonatal bacteramia are: Staphylococcus aureus, Escherichia coli and Klebsiella spp., and in older infants, S aureus, Streptococcus pneumoniae, Klebsiella and E coli, and non-typhoidal Salmonella.
-
Among community-acquired neonatal bacteraemia, resistance or reduced susceptibility to the combination of penicillin and gentamicin and to third-generation cephalosporins occurs in more than 40% of cases.
-
Among community acquired bacteraemia in infants 1–12 months, resistance or reduced susceptibility to the combination of penicillin and gentamicin and to third-generation cephalosporins occurs in more than 35% of cases.
Introduction
Between 30% and 50% of all deaths in children under the age of 5 years occur in the first month of life. Neonatal sepsis, the third most common cause of death in this age group, results in half a million deaths each year, the vast majority of which are in developing countries.1 Outside the neonatal period, the period up to 12 months carries the highest risk of death from sepsis. WHO recommends the use of clinical ‘danger’ and ‘priority’ signs to identify neonatal and infant sepsis, and empiric antibiotics to treat infants with suspected serious bacterial infection.2 So that evidence-based management recommendations can be refined, accurate information is required about the aetiology and antibiotic susceptibility of neonatal and infant sepsis, derived from studies using uniform methodologies and case definitions, from developing countries that are representative of those in their region.
WHO's Pocketbook of Hospital Care for Children, which provides clinical guidelines for the management of children in hospitals where resources are limited, particularly district hospitals, currently recommends treatment with ampicillin (or penicillin) and gentamicin for young infants (0–2 months) and benzylpenicillin plus chloramphenicol for older infants with suspected sepsis. If the infant's response is poor, the current advice is to change to ampicillin and gentamicin after 48 h. Second-line antibiotics include flucloxacillin where staphylococcal infection is suspected, and third-generation cephalosporins.2 With the reduction in price and more widespread availability, in many developing countries, third-generation cephalosporins are now used as first-line treatment for severe sepsis.
Thus far, the evidence for empirical antibiotics in infant sepsis has been limited by a lack of data on common bacterial pathogens and antimicrobial resistance, especially at the community and rural or district hospital levels in developing countries.3 Most studies of the aetiology of neonatal infections have been from tertiary hospital neonatal units where nosocomial infections and resistant organisms are common, and many studies have not distinguished between hospital- and community-acquired sepsis. Many studies of sepsis in older infants have been on cases with a septic focus, such as pneumonia or meningitis.4 ,5
This review evaluates the aetiology and antibiotic resistance patterns for community-acquired sepsis in infants where no clear focus of infection is clinically identified, using data published since 1996. From this the likely efficacy of WHO's recommendations can be estimated.
Methods
Search strategy
The search was conducted using Embase, Medline and the Cochrane Library database, employing the search terms described in online supplementary table A1. These terms were entered to capture primary data on aetiology and antibiotic susceptibility in infant sepsis in low and middle income countries, with the search terms varying slightly for each database. Only articles in English were reviewed. Letters, commentaries and case studies were excluded. The reference lists of relevant articles were accessed to broaden the search. The definition of low and middle income countries was in accordance with that of the World Bank and WHO.6 ,7
Sepsis was defined as a positive blood culture in studies where an inclusion criterion was clinical sepsis. The manifestations of clinical sepsis include: fever with no obvious focus of infection plus signs of systemic upset (eg, inability to drink or breastfeed, convulsions, lethargy or vomiting everything), cyanosis and fast breathing, purpura, cold skin with poor peripheral perfusion, low blood pressure, or pulses that are hard to detect.8–10
Studies that investigated the aetiology of infection with a clear focus (eg, pneumonia or meningitis) were excluded, as the management approach to these children will be different to that for the septic child with no clear focus. The full texts of all potentially relevant studies were retrieved and read. Studies that reported the recruitment of infants with sepsis that was likely to be hospital-acquired were excluded (see online supplementary box A1)
Box 1 Exclusion criteria
-
Studies reporting on hospital-acquired infections
-
Children with an identified focus of infection
-
Culture performed after day 2 of admission
-
Recruitment included infants admitted to a health facility for other reasons than suspected sepsis
-
Studies set in intensive/critical care units
-
Studies exclusively recruiting immune-compromised, low birth weight or malnourished children.
-
Studies of prophylactic antibiotics e.g. for neonates of mothers with infection
-
Studies performed prior to 1996
-
Studies that do not report disaggregated results for neonates or infants from older children and adults
-
so that only studies of community-acquired sepsis would be selected.
Analysis
Results were extracted from each study and entered into a spreadsheet. Studies were summarised by extracting the study setting, design, inclusion criteria and methods of sampling and culture. Data collected from each study included the number of infants who had blood cultures sampled, the number who had positive cultures for a bacterial pathogen, the frequency of all isolates, and the isolate-specific antibiotic susceptibility where this was reported. Using random effects meta-regression, an extension of the standard meta-analysis,11 we calculated the proportion of bacteraemia due to different pathogens. This method weighs the proportions found in individual studies according to study sample size, and estimates the extent to which heterogeneity between the results of multiple studies can be related to one or more characteristics of the studies.
The studies were evaluated for the quality of bacterial isolation methods and antibiotic susceptibility testing using specific criteria (see online supplementary).
To determine the efficacy of WHO's currently recommended antibiotics, aetiology and susceptibility data were combined. The susceptibility of individual pathogens to specific antibiotic combinations was calculated using random effects meta-regression,11 weighting for number of isolates tested in each study. These proportions were described for each of the antibiotic combinations currently recommended by WHO: (1) benzylpenicillin/ampicillin and gentamicin, (2) chloramphenicol and benzylpenicillin, and (3) third-generation cephalosporins as a single agent. Only combinations 1 and 3 were evaluated for neonates, as chloramphenicol is not recommended by WHO as treatment for neonatal sepsis. These weighted proportions were multiplied by the weighted proportions of all cases of sepsis caused by that pathogen. This resulted in a data set that describes the proportion of infant sepsis attributable to a pathogen that is susceptible to recommended antibiotics. The sum of these values indicates the total proportion of infant sepsis that is susceptible to each of the antibiotics or antibiotic combinations analysed.
A number of assumptions were made in this methodology: first, the combined efficacy of two antibiotics is equal to that of the more efficacious of the two12; second, age did not significantly affect antibiotic susceptibility, as some studies of susceptibility included children older than 1 year; and third, benzylpenicillin and ampicillin are equivalent for the purpose of the analysis, because these antibiotics are generally interchangeable in WHO recommendations.
Results
The search retrieved 615 published studies in Medline, 229 in Embase and 373 in the Cochrane database. Of these, 61 studies identified in the Medline search and 28 studies identified in the Embase search were potentially relevant, with six studies identified in both databases. One additional relevant study was published since the literature search was conducted, and this was included.13 Therefore, the full texts of 84 (90 minus 6) studies were sought. There were Cochrane reviews that were potentially relevant, but these were eventually excluded: two were not set in low and middle income countries, one had no measurable outcome, and one was in protocol form only.14–17
Of the 84 articles retrieved, 63 were excluded (figure 1). One further study reported data that were duplicated by a larger report included in the review (the Gambian component of the multi-country Young Infant Study18) and another19 reported data contained within a more recent study from the same site in Malawi.12 This left 19 studies from 13 countries.

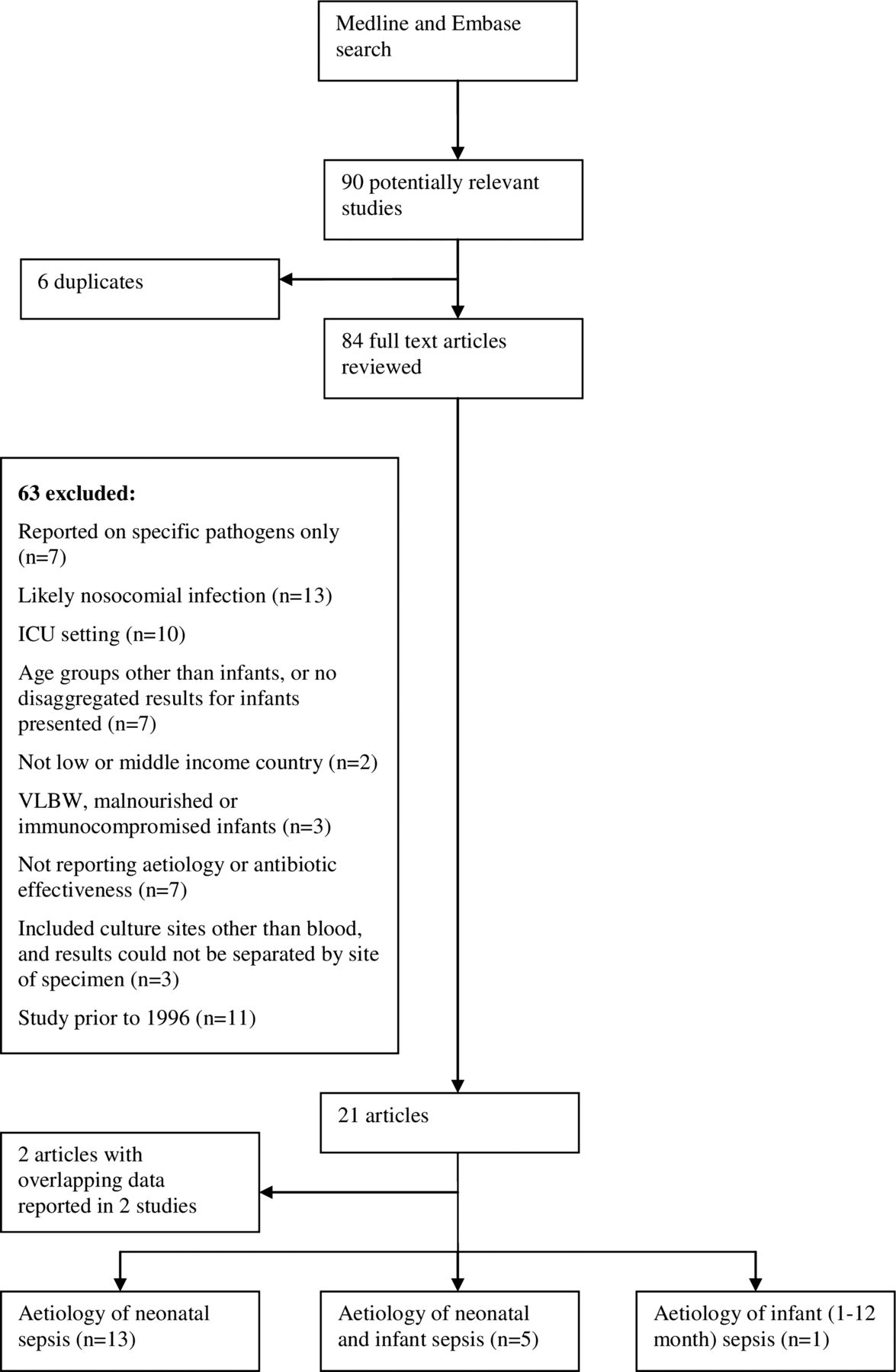{kind=link}
Retrieval strategy and reasons for study exclusion, ICU, intensive care unit; VlBW, very low birth weight .
Description of included studies
Of the 19 studies identified, nine were from Africa, eight from Asia, one from Iraq and one (the WHO Young Infant Study) was a multi-country study that included hospitals and clinics in Gambia, Ethiopia, Philippines and Papua New Guinea.20 One study was based on community surveillance, three studies were from rural district or provincial hospitals, 14 studies were from tertiary or referral hospitals, and the Young Infant Study included primary to tertiary health facilities.
Sixteen studies were prospective. These studies investigated the aetiology of positive blood cultures in either all infant admissions,21 infants admitted with fever without localising features22 ,23 or infants admitted with signs of severe illness or suspected sepsis.12 ,13 ,24–36 (table 1). One study, a retrospective review of laboratory records from a tertiary hospital neonatal ward, reported data from positive cultures of neonates admitted with suspected sepsis.35
Included studies of the aetiology of sepsis in young infants
One study reported data from two centres in India: a neonatal intensive care unit and a rural district hospital. In line with this review's inclusion criteria, data were only extracted from the rural district hospital for this review.13
The number of positive cultures included in each study varied from 3030 ,31 to 784.12 Five studies (four from Africa and one from India) provided data for 72% of all positive isolates included in the review (2914 of 4049).12 ,21 ,23 ,28 ,35
Quality of included studies
The review aimed to focus on community-acquired sepsis. We excluded studies which were identified as being from intensive care units. Not all studies were explicit on the proportions of infections that were community-acquired and nosocomial. The quality of laboratory methods was assessed using a systematic approach (see online supplementary box 1 for method, and online supplementary table A2 for study-level assessment). Most studies reported on blood culture collection methods (17/19), described fully the biochemical identification methods (14/19) and reported antibiotic susceptibility (17/19). The reporting of laboratory methods for bacterial identification was optimal in six of 19 studies. Eleven studies did not describe either how contaminants were distinguished from pathogens, whether biochemical identification was carried out, or what quality assurance methods were used. In two studies bacteriological methods were not described. Eight of 19 reported that a reference method for susceptibility testing was used.
Aetiology
In the 19 studies there were a total of 4049 positive blood cultures: 76% of the positive cultures were in neonates (3077 of 4049 cultures) and 24% (972 of 4049 cultures) in infants aged 1–12 months (table 2). All but three studies12 ,20 ,34 reported the number of total blood cultures tested. When it was reported, the range of prevalence of bacteraemia in infants for whom a blood culture was performed was 3–16% in studies from community surveillance or first-referral (including rural and district) hospitals, and 20–60% in studies from tertiary hospitals.
Bacteria isolated and prevalence weighted for study sample size
Using meta-analysis to weight for study size, among neonates, Staphylococcus aureus, Klebsiella spp. and Escherichia coli accounted for 55% (39–70%) of bacteraemic sepsis. These three pathogens, plus unidentified Gram-negative organisms, accounted for 62% (43–79%) of bacteraemic neonatal sepsis.
Among infants outside the neonatal period, the most prevalent pathogens were S aureus, E coli, Klebsiella spp., Salmonella spp. and Streptococcus pneumoniae, accounting for 59% (26–92%) of positive sepsis in infants older than 1 month on weighted analysis. Of the 103 isolates of Klebsiella spp., 90 were reported by one study from India.28
Antibiotic susceptibility
Fifteen studies reported aetiology-specific antibiotic susceptibility data.12 ,13 ,21 ,23 ,25–36 One study26 reported antibiotic susceptibility for all isolated bacteria without specifying individual pathogens, and another did not specify the number of isolates tested for susceptibility.35 Studies reported aetiology-specific antibiotic susceptibility for neonates,12 ,13 ,25–27 31–36 infants up to 12 months of age,28 and children up to 1521 and 18 years of age.23 Susceptibility data for individual pathogens, weighted for the sample size of each study which tested antimicrobial susceptibility to that bacterium, are summarised in table 3. There were high rates of resistance among most species of enteric Gram-negative bacteria to gentamicin, chloramphenicol and third-generation cephalosporins. Similarly, there were high rates of resistance among S aureus to third-generation cephalosporins, and the β-lactamase stable penicillins (oxacillin, cloxacillin and flucloxacillin). table 4 and 5 present susceptibility data weighted for prevalence in neonates and infants over 1 month, respectively. This gives an indication of the proportion of each pathogen that causes bacteraemia which is likely to be susceptible to recommended antibiotics. Among neonates with bacteraemia, the prevalence of susceptible bacteria to the penicillin and gentamicin combination, and to third-generation cephalosporins was 57% and 56%, respectively. Among older infants with bacteraemia, the prevalence of bacteria susceptible to the penicillin and gentamicin combination, to chloramphenicol, and to third-generation cephalosporins was 63%, 47% and 64%, respectively.
Weighted antibiotic susceptibility and number of isolates tested
Antibiotic susceptibility of blood culture isolates in neonates
Antibiotic susceptibility of blood culture isolates in infants aged 1–12 months
Discussion
In developing countries, the high burden of invasive bacterial infections in young children and limitations in diagnostics make it essential that effective empirical antibiotic guidelines and therapy are available. WHO's clinical guidelines for the management of common childhood illnesses take into account the constraints of low-resource settings. For children with signs of sepsis but no localising signs of specific infections such as pneumonia or meningitis, empiric antibiotic therapy aims to broadly cover the most likely causes of septicaemia for the relevant age group.
This review found that a few bacteria cause the majority of infant sepsis, especially in the neonatal age group, where S aureus, Klebsiella spp. and E coli accounted for 55% of all sepsis. In contrast to studies from Western countries,37 there was a much lower proportion of sepsis due to group B streptococcus, an estimated prevalence of only 2%. S aureus, S pneumoniae, Klebsiella spp., E coli and Salmonella spp. were the most important pathogens in older infant (>1 month) sepsis.
We estimated that 57% and 63% of bacterial isolates in neonates and older infants, respectively, were susceptible to the combination of benzylpenicillin/ampicillin and gentamicin. Third-generation cephalosporins are often perceived as superior agents, but these did not provide higher coverage than penicillin/gentamicin. Third-generation cephalosporins had in vitro efficacy against 56% of neonatal pathogens and 64% of older infant pathogens. Among neonates, the gaps in antibiotic coverage with either regimen were mostly in infections due to enteric Gram-negative bacilli, particularly Klebsiella spp. Current empirical antibiotics are inadequate for most isolates of Klebsiella spp., which accounts for one in five cases of neonatal sepsis in developing countries.
Study limitations
Limitations of this review include representation and heterogeneity. Although this review includes data from more than 4000 episodes of bacteraemia from 13 countries, this is a minute proportion of the annual global burden of this infection. Studies were of variable size and quality. Heterogeneity occurred at many levels: clinical criteria for enrolment in studies, study settings, study methodology, quality of laboratory methods and reporting. For example, a quality assessment of blood culture collection and processing identified that only eight of the 19 studies had optimal methods and two studies did not describe their blood culture methods.31 ,33 Eleven studies did not report whether they used such standardised susceptibility testing (online supplementary table A2). Use of a standardised reference method (eg, Clinical Laboratory Standards Institute or Eucast criteria) is important to ensure that susceptibility results are reproducible and accurate. When antibiotic choices are made, it is often assumed that in vivo efficacy is closely related to in vitro susceptibility. Where a reference method is not used, it is difficult to be certain of the correlation between in vitro results and in vivo efficacy. While 4049 bacterial isolates were identified in these studies, there was variability in the numbers of isolates which underwent susceptibility testing: 3560 were tested against penicillin/ampicillin, 3377 against gentamicin, 3456 against chloramphenicol and 1624 against third-generation cephalosporins. The efficacy of third-generation cephalosporins may have been under-estimated due to missing data.
An assumption made by this review is that all studies tested for the most important bacterial pathogens causing sepsis in this age group. This is reasonable, as most pathogens grow with standard bacterial culture techniques.
In vitro and in vivo antimicrobial efficacy may differ for some antibiotics and some bacterial pathogens. S aureus is the most common pathogen causing neonatal and older infant sepsis, so resistance has a large impact on overall antibiotic efficacy. S aureus isolates had low susceptibility to third-generation cephalosporins and penicillinase-resistant antibiotics, but the prevalence of in vitro susceptibility to gentamicin was high (80%). These data may overestimate the efficacy of the combination of penicillin and gentamicin in treating S aureus. Gentamicin is not commonly accepted as an appropriate sole effective agent for S aureus. However, previous research has demonstrated that clinically achievable gentamicin concentrations kill S aureus.38 In a previous community-based trial, the addition of gentamicin to cotrimoxazole as treatment for neonatal sepsis markedly reduced mortality,10 so it may be that more S aureus infections are being adequately covered by the currently recommended benzylpenicillin/ampicillin plus gentamicin combination than conventional wisdom dictates.
The estimates have other limitations. Data are more likely to be produced by large tertiary centres, and it can therefore be difficult to be certain that infections were community-acquired. We attempted to account for this by excluding studies performed in highly specialised settings (eg, intensive care units) and excluding studies where infections were acquired after 2 days of hospital admission. As we did not exclude data from tertiary hospitals, we cannot be certain that some studies in neonatal units were not carried out in units with intensive care facilities including, for example, mechanical ventilation.
High levels of resistance or susceptibility reported in a few studies can skew the pooled results, however the meta-analysis process addresses this. Some 72% of the bacterial isolates were identified from five of the 19 publications, four of which were from countries in Africa.21 ,23 ,28 ,35
There was incomplete differentiation in the literature of Salmonella spp. into typhoidal and non-typhoidal Salmonella (NTS), and there are geographical differences in the prevalence of this form of bacteraemia. A total of 297 Salmonella spp. were identified of which 248 (83%) were non-typhoidal Salmonella, 11 Salmonella typhi and 38 were not typed, so it was not possible to classify the susceptibility data on these un-typed isolates. The substantial prevalence of Salmonella spp. in older infant sepsis (8%) is due to the predominance of African studies included in this review.39 WHO's recent recommendation away from penicillin plus chloramphenicol to third-generation cephalosporins for the empiric treatment of sepsis in this age group will result in more effective treatment of non-typhoidal Salmonella in African countries where NTS is highly prevalent.
Implications
The findings in this review have implications for global antibiotic recommendations. For neonates, sepsis due to resistant Gram-negative bacilli is an emerging and substantial problem, and the currently recommended first-line (penicillin/ampicillin plus gentamicin) or second-line antibiotics (a third-generation cephalosporin) do not provide adequate cover. Appropriate second-line treatment for when these bacteria are isolated or suspected needs to be explored and clinical indications for timely second-line therapy need to be developed. Amikacin is effective against most multi-resistant Klebsiella spp. and may be an alternative to gentamicin as second-line treatment in combination with a penicillin. Amikacin is comparable to the cost of gentamicin, a median price of US$0.54 per 100g vial of amikacin, compared to US$0.16 per 40g vial of gentamicin.40 Carbapenems, fluoroquinolones and extended-spectrum penicillins such as piperacillin-tazobactam and ticarcillin-clavulinate are expensive, drive resistance and are not widely available in developing countries.
Although it is often believed that third-generation cephalosporins are superior to older antibiotics, and are preferred as the agent of choice for severe sepsis, this study found this not to be true. Third-generation cephalosporins did not provide increased in vitro susceptibility. Furthermore, at least one controlled trial of treatment of neonatal sepsis using third-generation cephalosporins as first-line treatment has increased rates of resistance among bacterial pathogens in a hospital.41 This study was in tertiary neonatal units in a developed country, but the lessons are important for developing countries where the use of cephalosporins is increasingly widespread and uncontrolled. Third-generation cephalosporins are not more effective against common bloodstream bacterial pathogens than the combination of penicillin and gentamicin, but may be driving antimicrobial resistance among Gram-negative pathogens.
This review excluded studies of pneumonia and meningitis. This will have the effect of under-estimating the prevalence of bacteraemia due to S pneumoniae and Haemophilus influenzae, especially in the age group 1–12 months.
It is important to note clinical situations where these data do not apply. While for bacteraemia there was no advantage in using third-generation cephalosporins over penicillin and gentamicin, third-generation cephalosporins are likely to be more effective at treating Gram-negative meningitis than penicillin and gentamicin. Although there is no randomised trial evidence to support this, the use of cephalosporins for neonatal meningitis in industrialised countries has coincided with a reduction in death rates from this infection, although with no documented decrease in morbidity.42 ,43 The main results of this study therefore apply to non-meningitis sepsis.
The purpose of this paper was to assess whether current WHO guidelines for the empiric treatment of infant sepsis are appropriate. For this reason it was necessary to combine reported antibiotic susceptibility testing results from around the world, since these guidelines have been developed for use worldwide. However, local prevalence and susceptibility results, where available, should be the most important factor guiding local empiric antibiotic choices.
This review raises many questions of global public health importance. These are both technical and programmatic. They include: how to determine clinical criteria for second-line therapy that are implementable in resource-limited settings; how to ensure recommendations are effective but minimise the development of further resistance; how to make available more expensive or higher-generation antibiotics in resource-limited developing countries but ensure their use is based on evidence; and how to address the poor state of bacteriology services in most developing countries and improve local surveillance data.
Conclusion
More than half the cases of neonatal sepsis were due to S aureus, E coli or Klebsiella spp. In older infants, Gram-positive bacteria (S aureus and S pneumoniae), in addition to Klebsiella and E coli and non-typhoidal Salmonella (in some regions), were the most important causes of bacteraemia. More than 40% of sepsis in neonates and more than 35% of sepsis in older infants was due to pathogens that were resistant (or had reduced susceptibility) to the antibiotic combination of ampicillin/penicillin and gentamicin, or the increasingly used alternative, third-generation cephalosporins. Revised recommendations for second-line antibiotics in neonatal and infant sepsis are needed. This task will be complex, but these are issues that the global health community need to address urgently. The methodology used in this systematic review could provide a model for longitudinal surveillance of bacteraemia in infants, which could offer long-term understanding of the aetiology and antibiotic resistance patterns in different regions. Improving bacteriology services in provincial and district hospitals in rural developing countries is essential for representative global data.
Acknowledgments
We are grateful to Dr Susan Donath of the Centre for Epidemiology and Biostatistics at the University of Melbourne for guidance on the meta-analysis methodology.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors All authors had a role in designing the study methodology. LD, RA, RS, JK and TD carried out the literature search, retrieved articles and analysed the data. LD and RA wrote the first draft of the paper, and all authors contributed to subsequent drafts. VC assessed the quality of laboratory methods. TD and JK supervised the study.
-
Funding This research was supported by funding from the AusAID Knowledge Hubs for Health Initiative given to the Centre for International Child Health (CICH), The University of Melbourne. CICH is also a World Health Organization Collaborating Centre for Research and Training in Child and Neonatal Health. Neither agency influenced the publication of these results.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.