Article Text

Abstract
Background Morbidity and mortality remain high following infant cardiac arrest. Optimal cardiopulmonary resuscitation (CPR) is therefore imperative.
Objective Comparison of two-thumb (TT) and two-finger (TF) infant chest compression technique compliance with international recommendations.
Design Randomised cross-over experimental study.
Methods Twenty-two certified Advanced Paediatric Life Support (APLS) instructors performed 2 min continuous TT and TF chest compressions on an instrumented infant CPR manikin. Compression depth (CD), release force (RF), compression rate (CR) and duty cycles (DCs) were recorded. Quality indices were developed to calculate the proportion of compressions that complied with internationally recommended targets, and an overall quality index was used to calculate the proportion that complied with all four targets.
Results Mean CD was 33 mm and 26 mm (p<0.001; target ≥36.7 mm), mean RF was 0.8 kg and 0.2 kg (p<0.001; target <2.5 kg), mean CR was 128/min and 131/min (p=0.052; target 100–120/min) and mean DCs was 61% and 53% (p<0.001; target 30–50%) for the TT and TF techniques, respectively. With the exception of RF, the majority of compressions failed to comply with targets. The TT technique improved median CD compliance (6% vs 0% (p<0.001)), while the TF technique improved median DC compliance (23% vs 0% (p<0.001)). Overall compliance with all four targets was <1% for both techniques (p=0.14).
Conclusions Compliance of APLS instructors with current international recommendations during simulated infant CPR is poor. The TT technique provided improved CD compliance, while the TF technique provided superior DC compliance. If this reflects current clinical practice, optimisation of performance to achieve international recommendations during infant CPR is called for.
- Resuscitation
- chest compression
- infant
- manikins
Statistics from Altmetric.com
What is already known on this topic
-
Outcome of infant cardiopulmonary resuscitation (CPR) remains poor.
-
Manikin studies demonstrate a superior compression depth quality with the two-thumb technique and rapid compression rates for two-thumb and two-finger techniques.
-
Chest release forces, duty cycles and compliance of chest compression during simulated infant CPR against international targets are unknown.
What this study adds
-
With the exception of release forces, chest compressions failed to comply with internationally recommended targets.
-
The two-thumb technique improved compression depth compliance, while the two-finger technique improved duty cycle compliance.
-
Each technique rarely complies with all four chest compression targets.
Introduction
Current cardiac arrest outcomes in the infant population continue to exhibit undesirably high morbidity and mortality.1 ,2 Since effective closed chest cardiopulmonary resuscitation (CPR) achieves only 50% cerebral and 15–25% coronary baseline blood flow levels,3–5 the provision of quality chest compressions to maximise cardiac output is essential to its success. To improve infant survival rates, current European (ERC) and UK Resuscitation Council (UKRC) guidelines recommend the delivery of high-quality chest compressions during infant CPR using either the two-thumb (TT) or two-finger (TF) chest compression technique.6 ,7
Fundamental to providing quality chest compressions are the four quality measures identified by the internationally agreed guidelines for the uniform reporting of the measured quality of CPR: chest compression depth; chest release force; chest compression rate; and compression duty cycles (ie, the proportion of each compression cycle with active chest compression).8 Previous studies have attempted to compare TT and TF technique quality by simulating chest compressions on instrumented infant CPR training manikins.9–14 Although the majority conclude that the TT technique is statistically superior overall,9–13 only the quality of chest compression depths and compression rates were characterised. As neither chest release forces nor compression duty cycles were evaluated by any study, it remains unclear whether the TT chest compression technique is in fact superior.
The aim of this study was to assess Advanced Paediatric Life Support (APLS) instructor performance during simulated infant CPR on an instrument CPR manikin. The study was designed to compare the differences between TT and TF technique, assessing chest compression compliance with all four internationally recommended chest compression quality measures.
Methods
Infant manikin design
A commercially available CPR training manikin (Laerdal ALS Baby; Laerdal Medical, Stavanger, Norway), representing a 3-month-old 5 kg male infant, was instrumented with a linear potentiometer. Sensor output was recorded via a data acquisition card (National Instruments, Austin, Texas, USA) at a sample rate of 50 Hz, and transferred to a custom LabVIEW software programme (National Instruments) on a laptop to record output voltage. The manikin instrumentation was calibrated to measure chest deflections and chest compression forces at the lower third of the sternum (error ±0.07 mm and ±0.07 kg), and calibration was checked before and after testing, demonstrating no change in measurement errors. Finally, the external diameter of the manikin thorax, between the most anterior and posterior aspects of the thorax at the lower third of the sternum, was measured as 110 mm.
Experimental procedure
This randomised crossover experimental study was approved by two local National Health Service health boards in the South Wales region. Twenty-two certified APLS instructors were recruited as participants from two APLS training courses. Before testing, the instrumented manikin was set up in an assessment room, on a flat table, with the laptop and peripheral equipment located securely below. Instructors were randomly assigned to an initial chest compression technique (TT or TF) and instructed to perform continuous chest compressions (ie, no requirement to perform ventilations) for 2 min for each technique (the maximum time for which a resuscitator is expected to perform continuous chest compressions7). Full instructor recovery was permitted between techniques. Manikin chest deflections were continuously recorded throughout, with both the instructor and investigator blinded to performance feedback. Instructors were neither refreshed nor coached on technique, nor briefed about the nature of the observations being made or the study objectives. Individual results were fed back to the instructor after study completion.
Chest compression quality
Chest compression quality measures for this study were adapted from internationally agreed guidelines for the uniform reporting of the measured quality of CPR (figure 1).8 Chest compression depths were defined as the maximum chest deflections measured during the chest compression phase. Chest release forces (kg) were defined as the minimum chest compression forces measured during the chest release phase. Chest compression rates were calculated from the inverse of the time between consecutive chest release forces (and quantified as compressions/min). Compression duty cycles were calculated by dividing the area under the chest deflection curve by the product of compression depth and cycle time for each compression cycle—that is, this combines the compression and the period of release, as demonstrated in figure 1. All quality measures were calculated for each chest compression cycle, which were defined between consecutive chest release forces.

Example chest deflection curves defining chest compression depth (CD), chest release force (RF), chest compression rate (CR) and compression duty cycle (DC). Each chest compression cycle is represented by a dashed line, the circular markers represent the points recorded for each quality measure, the shaded region represents the area under the chest deflection curve for the chest compression cycle, and the dashed and double dotted lined box represents the product of the CD and the chest compression time. CR is calculated by the inverse of the time between consecutive release forces. DC is calculated by the area under the chest deflection curve (shaded region), divided by the product of the CD and the time between consecutive release forces (dashed and double dotted lined box).
To characterise chest compression compliance, quality indices were developed for compression depths, release forces, compression rates and duty cycles, along with a quality index to characterise overall chest compression compliance. For each quality index, the proportion of chest compressions that complied with internationally recommended targets was calculated for each instructor. Chest compression depth and compression rate targets were based on ERC and UKRC guideline recommendations: targeting depths of ‘at least one-third’ the external anterior–posterior (AP) chest diameter (≥36.7 mm for this manikin model) and a rate between 100 and 120 compressions/min.6 ,7 A chest release force target of <2.5 kg was defined to represent the residual chest compression force associated with a clinically significant increase in intrathoracic pressure in infants.15 Finally, a duty cycle target of 30–50% was defined to represent the most effective duty cycle range observed in infant animal surrogates.16–18 Secondary chest compression depth and release force targets were also analysed. Using the ERC and UKRC guidelines, targets of approximated infant chest compression depth targets of 40 mm and a release force of <0.5 kg (<10% of manikin weight) were determined to represent the complete release of the chest.6 ,7 To determine overall compliance, the proportion of chest compressions that achieved all four primary chest compression targets was also calculated for each technique.
Statistical analysis
Median values for all four chest compression quality measures were recorded, along with the five chest compression quality indices, for each instructor. Depending on data normality, study results were reported as either mean±SD or median (IQR). Paired differences between techniques were reported as mean (95% CI). Results were compared statistically by paired Student t test or Wilcoxon's signed rank test as appropriate. The number of instructors that achieved quality index scores of 0%, 0–25%, 25–50%, 50–75%, 75–100% and 100% for each quality measure and for overall compliance was also evaluated for each technique and statistically compared by McNemar tests. Statistical significance was considered at p<0.05 for all tests, and all p values were two-sided. Statistical analyses were performed using the SPSS V.16.0 statistical software package. A minimum sample size of 22 instructors was required to adequately detect a mean paired difference 0.6 times the standard deviation of the differences, assuming data normality, a two-sided significance level of <0.05 and >80% power.
Results
The 22 study participants (eight male) were certified APLS instructors: 12 doctors, seven resuscitation officers and three registered nurses. Overall, 5180 and 5600 chest compression cycles were recorded, without interruptions, for the TT and TF techniques, respectively.
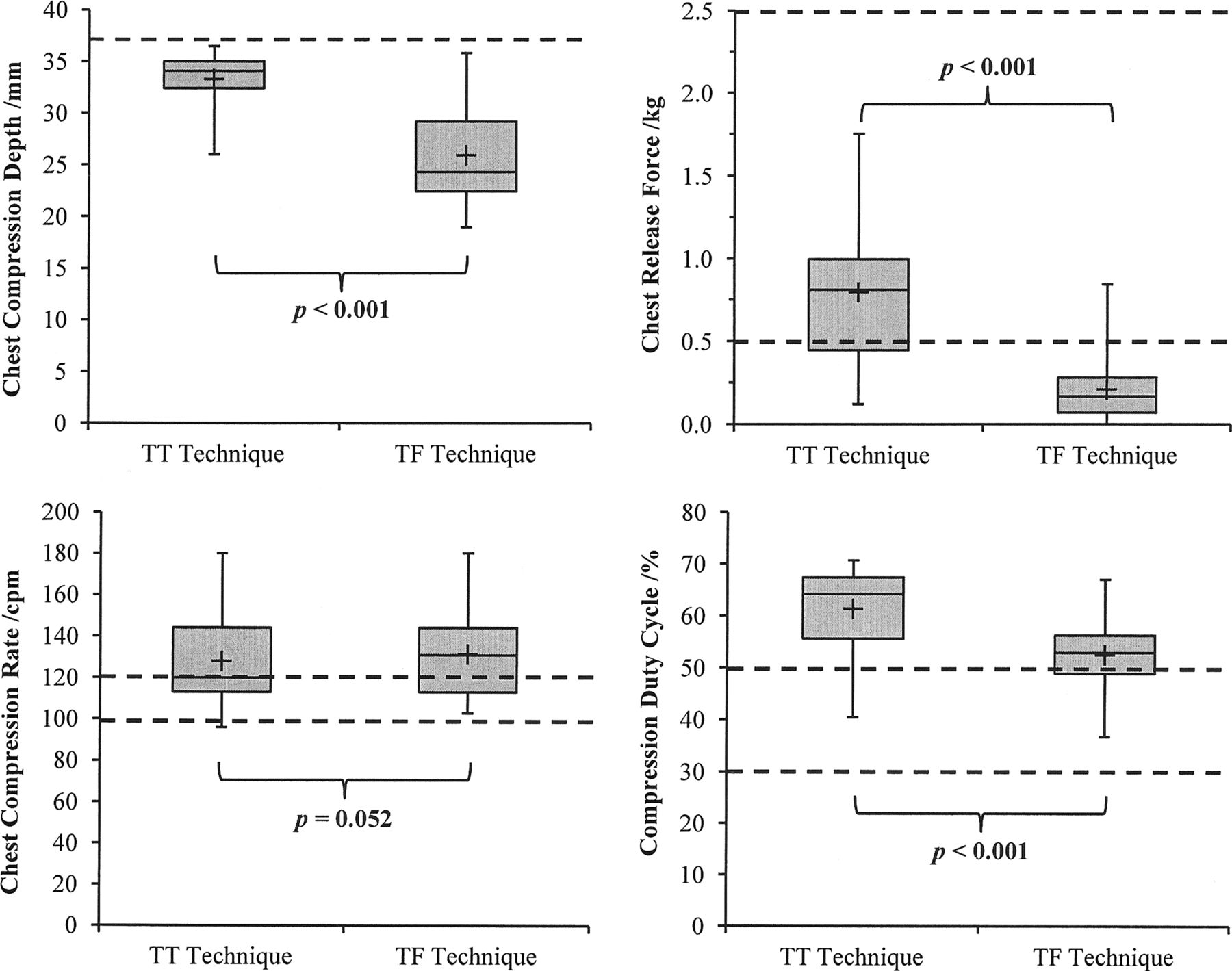
Simulated chest compression quality measures and indices are summarised in table 1 and illustrated against their internationally recommended targets in figure 2. Instructors achieved greater mean compression depths with the TT technique (TT: 33±3 mm vs TF: 26±5 mm (p<0.001); target ≥36.7 mm), while releasing the chest further (TT: 0.8±0.4 kg vs TF: 0.2±0.2 kg (p<0.001); target <2.5 kg) and reducing the compression duty cycle (TT: 61±8% vs TF: 53±8% (p<0.001); target 30–50%) with the TF technique. Mean chest compression rates were observed to exceed recommended targets for both techniques (TT: 128±21/min vs TF: 131±21/min (p<0.052); target 100–120/min).
Quality measures and indices for two-thumb (TT) and two-finger (TF) technique chest compressions

Illustration of median instructor two-thumb (TT) and two-finger (TF) technique chest compression depths (CD), chest release forces (RF), chest compression rates (CR) and compression duty cycles (DC) against internationally recommended targets (illustrated by dashed lines). CD targets were ≥36.7 mm, RF targets were <2.5 kg and <0.5 kg, CR targets were 100–120 compressions/min, and DC targets were 30–50%.
For both techniques, instructors were observed to achieve a median release force compliance of 100%, median compression rate and duty cycle compliances of <50%, and a median compression depth compliance of <6%. When techniques were compared, instructors displayed improved compression depth compliance when using the TT technique, and superior duty cycle compliance when using the TF technique. For the secondary analyses, all chest compressions failed to achieve depths of 40 mm, while a greater proportion of compressions achieved complete release (<0.5 kg) of the chest for the TF technique. Despite these improvements, however, overall chest compression compliance remained poor for both techniques, with <1% of all chest compressions complying simultaneously with all four recommended chest compression targets.
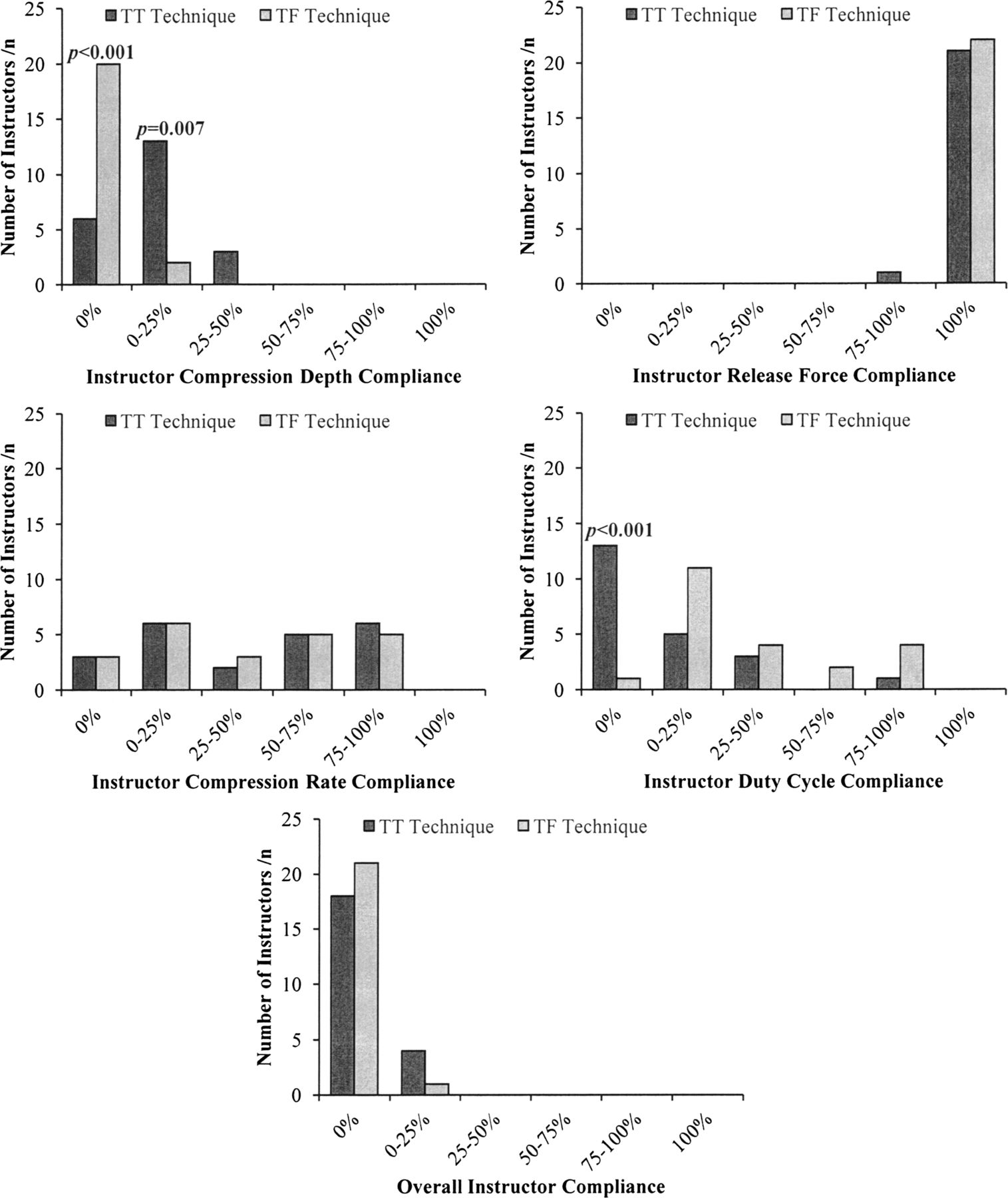
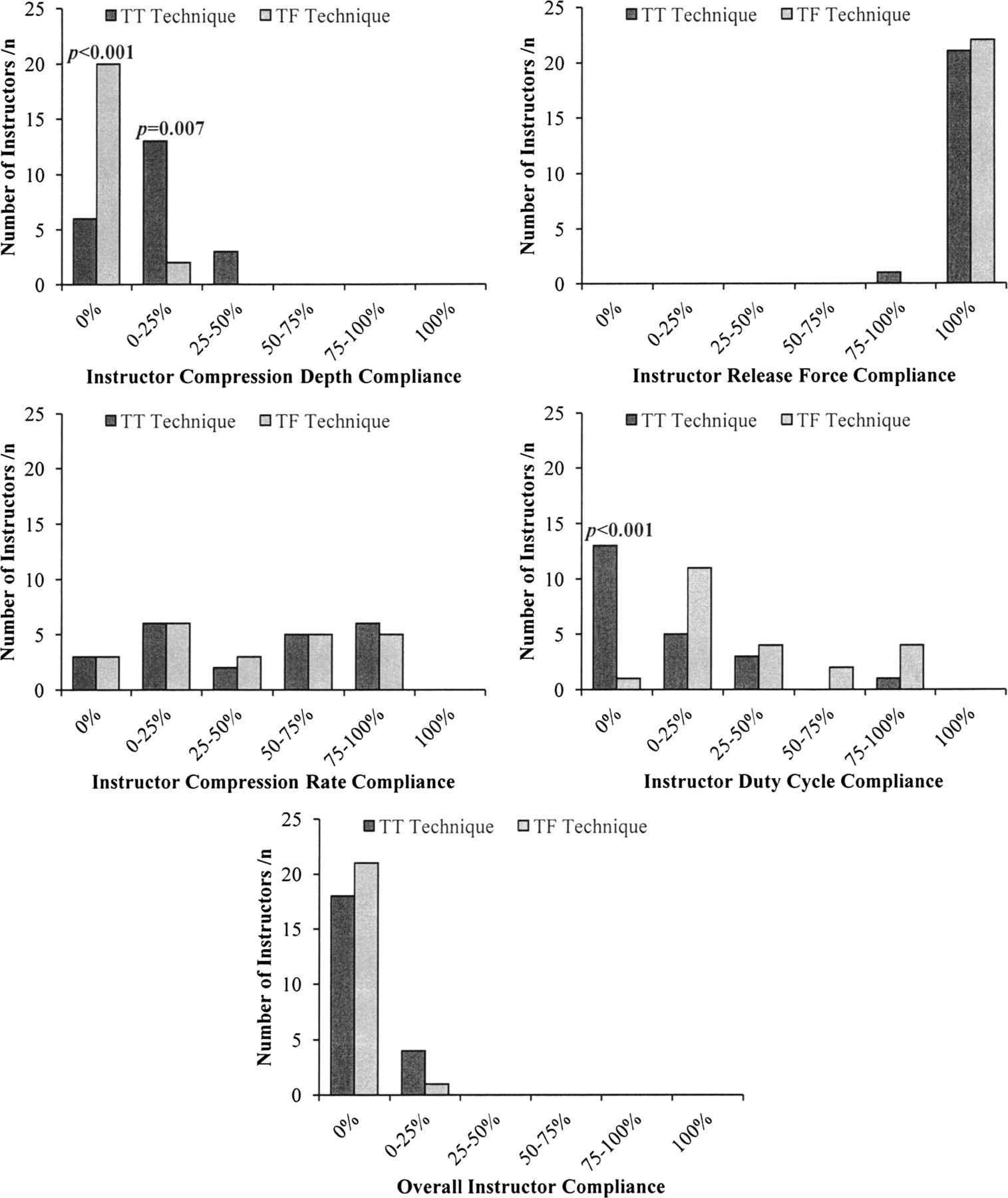
The number of instructors that achieved quality index scores of 0%, 0–25%, 25–50%, 50–75%, 75–100% and 100% are illustrated for each quality index and for the overall quality index in figure 3. For both techniques, no instructor achieved >50% compression depth compliance, while compression rate and duty cycle compliance were inconsistent and varied across the group. When using the TT technique, a greater number of instructors complied with compression depth targets, whereas, when using the TF technique, more complied with duty cycle targets. Overall, no instructor was observed to achieve >2% compliance with all four chest compression targets.
{kind=link}
{kind=link}
{kind=link}
Number of instructors who achieved quality index scores of 0%, 0–25%, 25–50%, 50–75%, 75–100% and 100% for chest compression depth compliance (target ≥36.7), chest release force compliance (target <2.5 kg), chest compression rate compliance (target 100–120/min), compression duty cycle compliance (target 30–50%) and overall compliance. p Values, calculated by McNemar tests, indicate a significant difference between the two techniques, two-thumb (TT) and two-finger (TF).
Discussion
This study is the first to evaluate the compliance of simulated infant CPR chest compressions provided by trained APLS instructors against current international recommendations. The results show that instructors achieved greater chest compression depths with the TT technique, while releasing the chest further and reducing the compression duty cycle with the TF technique. A greater proportion of compressions complied with compression depth targets of ‘no less than one-third the external AP chest diameter’ when the TT technique was used, while a greater proportion complied with compression duty cycle targets of 30–50% when the TF technique was used. Despite these individual improvements, overall quality was poor for both techniques, with <1% of all chest compressions achieving all four chest compression targets.
Despite current ERC and UKRC guidelines emphasising the delivery of high-quality chest compressions during CPR,6 ,7 this study suggests that overall chest compression compliance during simulated infant CPR is poor. Fundamental to this was a combination of shallow chest compressions, excessive compression rates and prolonged duty cycles. This is consistent with clinical reports on both adult and older paediatric populations,19–22 thus it is likely that poor-quality chest compressions remain prevalent during infant CPR.
Increased chest compression depths result in favourable haemodynamic outcomes, such as improved arterial pressures in both infant and adult human subjects, and superior coronary flow and cardiac output in animal surrogates.5 ,23–25 However, shallow chest compressions have been reported during CPR in both adult and older paediatric subjects and during simulated CPR on instrumented infant manikins.9–13 19–22 Despite greater TT technique compression depths being recorded by this study, this tendency to under-compress the chest was also observed. On average, 94% of all chest compressions failed to achieve or surpass target depths of one-third the external AP chest diameter, while all chest compressions failed to achieve guideline-approximated chest compression depth targets of 40 mm. The precise reasons for this are not yet clear, although it is possible that compression was restricted by the manikin design, which does not precisely match the internal diameter of the infant thorax. Other possibilities include reluctance on the part of the providers to over-compress in this simulated scenario.
Prolonged compression duty cycles, combined with increased compression rates, results in inadequate chest wall relaxation, impeding the venous return of blood to the heart and adversely affecting cardiac output, cerebral perfusion pressures and cerebral blood flow.16–18 ,26 While CPR chest compressions in adult and older paediatric subjects achieve target rates,19–22 the compression rates achieved during simulated CPR in infant manikins have been found to be faster than current targets and vary extensively between providers.10 ,11 ,13 Similar results were observed in this study, with >50% of chest compressions exceeding target rates and a large inter-participant variation. Although compression duty cycles of 33–47% during adult CPR have been reported,19 ,21 ,27 compression duty cycles during paediatric CPR have never been quantified. In this analysis of compression duty cycle compliance during infant CPR, 0% of all TT chest compressions and 23% of all TF chest compressions complied with infant compression duty cycle targets, with neither technique allowing adequate time for full chest recoil.
Incomplete chest release during CPR has been observed to generate increased intrathoracic pressures during the chest release phase, consequently limiting the return of venous blood to the heart and reducing coronary and cerebral perfusion pressures.15 ,27–29 While incomplete release during CPR in older paediatric subjects has been observed in 25–50% of chest compressions,22 ,30 >97% of chest compressions achieved target release forces during CPR in adults.19 The chest release force compliance demonstrated by this study establishes that both techniques during simulated infant CPR achieved >99% compliance with current release force targets. On assessment of the complete release of the chest, however, instructors were found to achieve complete release targets of <0.5 kg (<10% of the manikin weight) more often when using TF technique. As chest release forces of as little as 10% of the body weight of the subject cause a measurable increase in intrathoracic pressure,15 the TF technique may therefore provide a superior return of venous blood to the heart.
This study has three key limitations. First, although infant CPR training manikins have been extensively used for investigating CPR quality, their design is recognised as intrinsically flawed.9–14 For the manikin used in this study, a maximum achievable chest compression depth of 40 mm was defined at an applied force of 26 kg (a force equivalent to double the mean maximum palmar pinch force for the dominant hand of a male adult31). As the mean internal AP thoracic depth of a 3-month-old boy is ∼56.2 mm,32 instructor chest compression depths may have been restricted by the manikin to unrepresentative depths. Second, the chest compression targets developed by this study were derived from a combination of human subject, radiographic and animal surrogate studies. This, however, reflects the current scientific evidence guiding internationally recommended infant chest compression targets, and, with future research, these targets for benchmarking resuscitator performance may be updated. Finally, despite being blinded to the study objectives, the instructors would have been aware of being observed and therefore their performance may have been affected.
To improve the current compliance of infant CPR chest compressions, instructors must be encouraged to achieve target compression depths for both recommended techniques. This may, however, be easier to achieve and maintain with the TT technique, as it performs deeper chest compressions and delays fatigue.10–12 Further improvements may also be achieved by educating resuscitators to allow a greater time for full chest recoil. This would maintain the excellent chest release force compliance observed in this study and may potentially improve compression duty cycle compliance. Finally, improving the quality of compression rates may also be realised through regulation with audiovisual aids. Through targeting improvements in all four chest compression quality measures and using quality indices as a performance benchmarking tool, a future improvement in overall chest compression compliance may be possible.
Conclusions
This study is the first to fully evaluate the compliance of simulated infant CPR chest compressions against current internationally recommended targets. Overall, either technique rarely complied with all four targets, with excessive chest compression rates and prolonged compression duty cycles prevalent. The TT technique demonstrated improved compression depth compliance, while the TF technique provided superior duty cycle compliance. Thus, there remains scope for a considerable improvement in the quality of infant chest compressions. Future work should focus on ensuring that APLS instructors are made aware of their performance against international recommendations.
Acknowledgments
The authors would like to thank the staff and technicians at the Cardiff University Schools of Engineering and Medicine for their help and valuable comments. The authors would also like to thank the APLS training course organisers and NHS Trusts for hosting this research. Finally the authors would like to thank the Engineering and Physical Sciences Research Council, Professor Alison Kemp and the Institute of Primary Care and Public Health for their provision of the funding for this research.
References
Footnotes
-
Contributors PSM: instrumented manikin, conducted all experiments, contributed to writing of manuscript. MDJ: designed study, supervised instrumentation, contributed to manuscript. PST: supervised experimental work, contributed to statistical analysis, contributed to manuscript. SAM: contributed to study design, contributed to manuscript. AMK: contributed to study design, contributed to manuscript.
-
Funding None.
-
Competing interests None.
-
Ethics approval NHS local health boards.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Further detailed analysis of the inter-subject variation is available, as is a detailed breakdown of each individual's results plotted against time. This could be made available if required.