Article Text

Abstract
Paediatric intensive care (PIC) services have been centralised to a significant extent in Britain in the past two decades. As part of centralisation, PIC retrieval teams were developed to transport critically ill children from district general hospitals to regional paediatric intensive care units. This review aims to summarise the current state of retrieval in Britain, with reference to the past and possible directions for the future. While significant progress has been achieved, and PIC retrieval has now become a clinical service in its own right, the coming years present unique opportunities as well as challenges for the specialty.
Statistics from Altmetric.com
Paediatric intensive care (PIC) retrieval teams have evolved over the past two decades in response to greater centralisation of PIC services. This review aims to provide a summary of the past, present and the future of PIC retrieval in Britain.
The past
Two major principles shaped the development of retrieval services in Britain: (A) centralisation of PIC services results in better outcomes for patients and (B) the use of specialist retrieval teams to transport critically ill children is associated with reduced patient morbidity.
Centralisation of PIC
By the 1990s, there was a growing body of scientific evidence to support the view that centralisation of PIC services at fewer, larger centres was associated with improved patient outcomes.1,–,3 There was also general consensus that practitioners working at centres that cared for critically ill children on an infrequent basis would find it difficult to maintain their skills in intensive care.4 In 1993, a report from the British Paediatric Association showed that critical care for children was provided in over 100 different hospitals in a multitude of settings, such as general wards and adult intensive care units (ICUs); only 51% of critically ill children were cared for in a dedicated paediatric unit.5 A national working party was subsequently established to review PIC service delivery in Britain. In 1997, in a landmark publication titled Paediatric Intensive Care: A Framework for the Future, the NHS Executive proposed centralisation of PIC services and the formation of regional clinical networks with designated 'lead centres'.6 In this model of care, the majority of critically ill children within each geographical area would be managed at regional PICUs, and lead PIC centres were responsible for outreach (education, feedback and support for local high dependency care) and provision of a retrieval service to stabilise and transfer critically ill children from DGHs.
Use of PIC retrieval teams
PIC retrieval teams are made up of staff trained in intensive care and aim to provide a quality of care during interhospital transport similar to that available on a PICU. In the 1990s, studies from different healthcare systems showed a high incidence of preventable technical and physiological adverse events when non-specialist teams performed critical care transfers, and much lower patient morbidity when specialist teams were used.7,–,11 Paediatric Intensive Care Society standards as well as the PIC Framework recommended that critically ill children were transported by specialist PIC retrieval teams, and funding was provided to lead centres to establish a retrieval service with 24-hour availability within their region.
The present
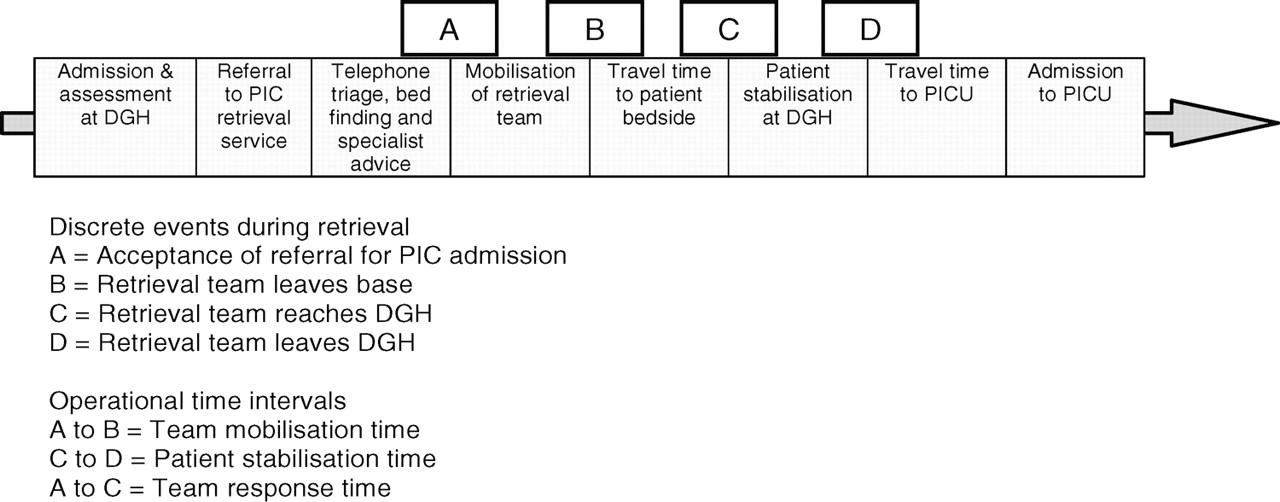
Following centralisation of services and development of retrieval teams over the past two decades, the PIC landscape has significantly changed: the vast majority of critically ill children are now cared for in dedicated PICUs, and of the 5000 children admitted from other hospitals to PICUs in Britain each year, over 80% are transported by PIC retrieval teams.12 The typical patient pathway during a present-day retrieval episode is illustrated in figure 1. Despite significant progress, regional differences in access to a specialist retrieval team in Britain continue to exist, evident from the variation in the proportion of emergency PICU admissions transported by non-specialist teams (table 1).13 Since the traditional retrieval model is for teams to be made up of staff already working on the ICU (PICU-based retrieval), at times of high bed occupancy and staff shortage, units without dedicated medical and nursing staff to run a retrieval team may be unable to consistently provide a 24-hour service. One of the main changes to PIC retrieval in the present era has been a gradual shift in the model of service delivery from small teams based in individual PICUs to large regional retrieval teams staffed separately and independently of the ICUs.

Typical patient pathway during a PIC retrieval episode. DGH, district general hospital; PIC, paediatric intensive care; PICU, paediatric intensive care unit.
Breakdown of retrieved PICU admissions in England and Wales (2005–2008) by type of retrieval team (n=16 875)
Models of retrieval service delivery
Over the past decade, two distinct models of service delivery have emerged. In the traditional PICU-based model, the retrieval service is run from the PICU itself, and the team is usually generated 'on-demand' from staff working on the unit. In regions with relatively low demand (typically less than one retrieval per day or <250 retrievals per year), this model of care can utilise staff flexibly and may be an efficient way to deliver a retrieval service, particularly if a single regional PICU covers a large geographical area. However, with greater demand for retrieval, and/or at times of high bed occupancy and shortage of staff experienced in undertaking retrieval, PICUs may be unable to despatch a team to travel to the DGH and assist local staff in patient stabilisation and transfer. This inherent unpredictability in the balance between supply and demand may result in an ad hoc retrieval service, rather than consistent 24-hour availability. Problems associated with the PICU-based retrieval model have prompted some regions to amalgamate two or three existing PICU-based teams to create one large regional PIC retrieval team in an attempt to increase efficiency with greater retrieval volume. Since regional retrieval teams are staffed separately from the PICU, they are able to mobilise a team independent of PICU bed capacity and staffing constraints. In addition, they offer a single point of contact for DGHs to access specialist advice, bed finding and a retrieval team that can transport the patient to any available PICU bed, in or outside the region.14 A number of such services have been established over the past decade. Some teams perform neonatal as well as PIC retrievals, while some only undertake retrievals into PICUs. Table 2 summarises the current status of PIC retrieval in the UK.
Summary of PIC retrievals teams currently in operation in the UK
Staffing and team composition
Traditionally, retrievals in Britain have been undertaken by PICU-trained physician–nurse teams. The physician component of the team usually includes PIC consultants or experienced PIC trainees with a background in paediatrics or anaesthesia. Trainees may either spend a dedicated period of time (3–6 months) on a regional team or undertake occasional retrievals as part of a PICU-based service in order to fulfil competencies within a recognised PIC training programme. Other staffing models, such as the use of advanced nurse practitioners (ANP), respiratory therapists and critical care paramedics are commonplace in the USA and Canada.15 ANPs have been increasingly used in Britain over the past few years in neonatal as well as PIC retrieval, and the development of advanced nursing roles has been significantly accelerated by recent changes to postgraduate medical training, junior doctor working hours and shortage of trainees in high intensity specialties.16 17 The development of ANP roles has the potential to improve staff recruitment and aid retention of experienced nurses in retrieval. Studies have shown comparable numbers of interventions between nurse-led and trainee physician-led retrievals, although detailed and systematic evidence to compare the effect of various team composition models on patient care is lacking.18 19
Transport infrastructure
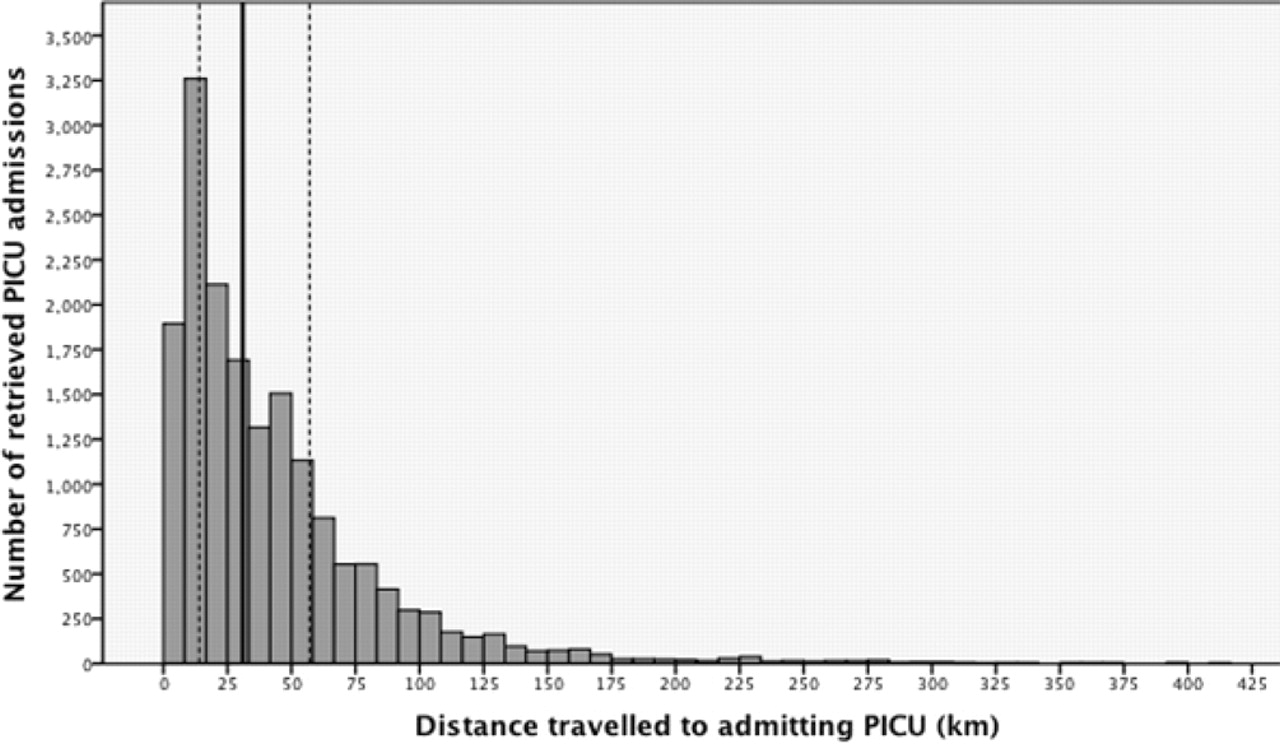
The relatively short distances involved in PIC retrieval in Britain (median 31 km, IQR 14–57 km) have resulted in the predominant use of ground ambulances for patient transport.13 While smaller PICU-based retrieval teams tend to rely on the local ambulance service provider for vehicles (for 'on-demand' use), larger regional retrieval services with a greater volume of activity have dedicated ambulances on-site to minimise delays associated with team mobilisation. The interior of a dedicated ambulance can also be customised to allow staff to deliver intensive care while on the road; improve staff and patient safety by the use of fixtures and clamps to securely fasten patient monitoring, ventilation equipment and infusion pumps and allow sufficient seating to accommodate additional retrieval trainees as well as parents. In contrast to road-based interhospital transport, air retrievals are exceptionally rare in the UK (2% of PIC retrievals in a recent national audit) due to the fact that there is no funded air retrieval service except in Scotland. Although a number of charitably funded air ambulances operate in Britain, their role is generally limited to primary transport of ill or injured patients from home or the roadside to local emergency departments rather than interhospital transport. Analysis of data from the Paediatric Intensive Care Audit Network (PICANet) shows that 4% (∼200 retrieved patients/year) travel more than 150 km to admitting PICUs (figure 2), suggesting that there may be a role for an organised air retrieval service in Britain.
{kind=link}
{kind=link}
Distance travelled by retrieved patients to admitting PICUs (2005–2008). Distance is calculated from patient's residential postcode to admitting PICU postcode; solid line represents the median; dotted lines represent 25th and 75th centile. PICU, paediatric intensive care unit.
Paediatric critical care networks
Most regions have now established paediatric critical care networks involving the regional PICU (or retrieval service) and referring hospitals. Since the typical patient journey involves acute management at the DGH followed by stabilisation and retrieval to the PICU, an important role of the network is to foster collaborative working between the DGH and the PIC retrieval teams to ensure optimal patient outcome. A recent publication from the Department of Health supported a team approach to the management of the acutely ill or injured child, and recommended the use of common guidelines for the management of emergencies and for drug preparation, standardisation of equipment and sharing of expertise across the network.20 Outreach education is also a key function of a PIC network. Both the 1997 Framework and recent Department of Health guidance encourage regional PICUs to provide outreach education to referring DGHs in order to help maintain their competencies in managing critically ill children. Outreach may take the form of lectures, hands-on skill sessions, simulation-based workshops and case reviews as well as provide opportunities for DGH staff to rotate through the retrieval service. More recently, innovative approaches including the use of videoconferencing (unpublished data from the Children's Acute Transport Service, London) and mobile simulation manikins (Hanna S, personal communication) have been piloted and have the potential to supplement traditional outreach education models.
Concerns have been frequently raised that centralisation of specialist paediatric services such as anaesthesia, surgery and intensive care have resulted in deskilling of DGH staff in the acute management of critically ill children, leading to delays in patient stabilisation until the arrival of the retrieval team.21 22 At least one recent study (albeit limited to a single region in England) did not support this view, instead demonstrating that the majority of airway and cardiovascular interventions had been performed by the DGH prior to the arrival of the retrieval team.23 Since median response times (time from referral to bedside) may be up to 90–120 min for retrieval teams, and even longer at times of high demand such as in winter, PIC networks will need to develop robust operational procedures to ensure that critically ill children can be adequately stabilised and managed locally even when the arrival of a PIC retrieval team is considerably delayed.24 In exceptional circumstances, such as time-critical neurosurgical emergencies (eg, rapidly expanding extradural haematoma), current national guidance recommends that DGH staff transfer the patient directly to the neurosurgical centre to ensure optimal patient outcome.25 This is a rare event for which PIC networks need to develop robust contingency plans, particularly since DGHs, with the least experience in transporting critically ill children, will be required to undertake the most urgent transfers. With increasing demand for PICU beds and limited resources, support for the management of children requiring high dependency unit (HDU) care, and the development of HDU facilities at the DGH, is rapidly becoming an important responsibility of the network.26 It is clear that despite the advent of centralised PIC and the widespread use of retrieval teams, early recognition of critical illness and timely intervention at the DGH are likely to remain important determinants of PICU outcome, emphasising the key role that DGHs play within the networked model.
Standards and performance indicators
PIC retrieval teams are expensive healthcare resources, and clinicians, commissioners and patients rightly expect them to deliver high quality, cost-effective care. Auditing the performance of a retrieval service against national standards is an important step in ensuring the delivery of such care. In this regard, Paediatric Intensive Care Society standards have been recently updated to cover retrieval and transfer of critically ill children in greater detail.27 Other performance indicators such as PICU mortality, occurrence of physiological adverse events on retrieval, mobilisation time and stabilisation time have also been suggested for PIC retrieval, based on practice at the Children's Acute Transport Service from London.14 PICANet has recently extended its dataset to cover retrieval information, which will provide valuable data for national audit and allow comparison of retrieval services across Britain. These data will also facilitate benchmarking against national and international retrieval standards (eg, the US-based Commission on Accreditation of Medical Transport Systems, www.camts.org).
Parental and patient experience
The stress to parents and families of children requiring retrieval can be immense, particularly in the context of the knowledge that their child's illness is serious enough to require transfer to PICU at another hospital. Waiting for the retrieval team to arrive can often be a terrifying experience, and the acute change in their child's physical appearance and condition can be traumatic. In this context, there is evidence that most parents desperately want to accompany their sick child during interhospital transport, and the separation anxiety induced at such a critical time is a major stress factor following admission to PICU.28 Practice within Britain is varied with regard to parental presence during PIC retrieval, mainly related to the ad hoc use of local ambulance vehicles in many retrieval services, which can only accommodate two members of the clinical team.29 A number of PIC retrieval services regularly conduct parental surveys to assess satisfaction with the service and the quality of information and support provided by the retrieval team.
Impact on patient outcome
There is a growing evidence base in paediatric retrieval and its impact on patient care. Early studies demonstrated how the use of specialist retrieval teams was associated with safer patient transport and reduced frequency of preventable adverse events.9 11 A survival benefit from the use of specialist retrieval teams was first demonstrated in a single centre study from the USA, which suggested that risk adjusted PICU mortality was higher for patients transferred by non-specialist teams.30 More recently, analysis of PICANet data collected over a 4-year period showed that the adjusted mortality risk for specialist retrieval team transfers into PICUs in England and Wales was nearly 40% lower in comparison with non-specialist team transfers, confirming significant benefits from the use of PIC retrieval teams on patient outcome.13
The future
PIC retrieval has evolved over the past two decades to become a distinct clinical service in Britain. Yet, the future offers even greater opportunities as well as challenges for the specialty.
Workforce and staffing
One of the most significant challenges facing PIC retrieval over the next decade is the availability of a skilled workforce to staff specialist retrieval teams on a 24-hour basis, particularly in the background of increasing demand for interhospital patient transport. The recent rapid expansion of the specialty and the establishment of regional retrieval services have already created a greater demand for trained staff, including PIC consultants, trainees and nurses; yet, the availability of medical and nursing staff has been limited by changes to postgraduate medical and overseas doctor training schemes, and a chronic shortage of trained PIC nurses. The possibility of expanding the workforce by recruiting non-PIC physicians and nurses, or critical care paramedics, to lead retrievals may need to be balanced against the benefits of using specialist teams who are trained to perform vital interventions and offer critical care 'in the field'. Newer models of care including development of senior PIC nurses into ANPs hold great promise, although significant investment in training and career development are required to maximise their potential and maintain a sustainable service.
Remote consultation
Although many PIC retrieval services currently offer telephone advice for DGHs during the management of critically ill children, the use of more advanced remote consultation models (eg, videoconferencing and telemetry) has great potential in the future where rising demand for critical care beds and shortage of trained PIC staff seem inevitable. There are several reports on the creation of successful virtual ICU networks using videoconferencing, where one large tertiary PICU supports numerous satellite hospitals.31 PIC retrieval services, positioned strategically between acute paediatric care and critical care, are ideally placed to adopt such models to complement telephone triage, improve the quality of advice given to DGHs during patient stabilisation, support local HDUs as part of a PIC network and even provide specialist input to relatively inexperienced retrieval teams.
Delivery of early critical care
The defining characteristic of a PIC retrieval team is its ability to deliver advanced critical care to the patient at a remote DGH rather than waiting for them to reach a PICU. There is increasing evidence that better patient outcomes can be achieved from early delivery of critical care treatments (eg, goal-directed therapy for sepsis),32 which PIC retrieval teams are in a unique position to provide. In addition, by means of outreach education and greater support to DGHs, retrieval teams may be able to improve outcomes by promoting early recognition and management of critical illness. However, these benefits remain speculative and the retrieval community has a responsibility to clearly demonstrate these benefits in collaborative studies conducted within a strong research framework.
Conclusions
The field of PIC retrieval has come a long way in Britain since its origins in the past few decades and continues to grow in step with the increasing demand for specialist interhospital transport. The future of the specialty lies in developing a successful model for a sustainable workforce that is capable of delivering early critical care and achieving the best possible outcomes for sick children.
Acknowledgments
We are grateful to Roger Parslow and Philip McShane from PICANet for providing some of the data presented in this article.
References
Footnotes
-
Funding National Health Service funding for the retrieval service.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.