Article Text

Abstract
Background: Some victims of sudden infant death syndrome (SIDS) are found with their heads covered with bedclothes, but the significance of this is uncertain. The aim of this review is to describe the prevalence of head covering, the magnitude of the risk and how far the suggested causal mechanisms agree with current epidemiological evidence.
Methods: Systematic review of population-based age-matched controlled studies.
Results: Controlled observations of head covering for the final sleep were found in 10 studies. The pooled prevalence in SIDS victims was 24.6% (95% CI 22.3% to 27.1%) compared to 3.2% (95% CI 2.7% to 3.8%) among controls. The pooled univariate odds ratio (OR) was 9.6 (95% CI 7.9 to 11.7) and the pooled adjusted OR from studies mainly conducted after the fall in SIDS rate was 16.9 (95% CI 12.6 to 22.7). The risk varied in strength but was significant across all studies. In a quarter of cases and controls head covering had occurred at least once previously (pooled adjusted OR = 1.1; 95% CI 0.9 to 1.4). The population attributable risk (27.1%; 95% CI 24.7% to 29.4%) suggests avoiding head covering might reduce SIDS deaths by more than a quarter.
Conclusions: The epidemiological evidence does not fully support postulated causal mechanisms such as hypoxia, hypercapnoea and thermal stress, but neither does it support the idea that head covering is part of some terminal struggle. Head covering is a major modifiable risk factor associated with SIDS deaths and parental advice to avoid this situation should be emphasised.
Statistics from Altmetric.com
In cases of sudden infant death syndrome (SIDS) the significance of finding the head or face of the infant covered by bedclothes remains uncertain in spite of its emergence as a putative risk factor. Prior to the acceptance of the label SIDS in the 1960s, it was common to attribute these unexpected deaths to “accidental mechanical suffocation” because the sleeping infant was often found with the face down in the bedclothes, the face covered by bedclothes or next to a sleeping parent.1 2 The assumption of smothering was criticised at the time, not least for the lack of evidence when apportioning blame to parent–infant care practices.3 Post mortem investigation of suspected asphyxial deaths were then, as now, largely inconclusive and anecdotal reports of attempts to reproduce the same conditions using ordinary bedding among live infants failed to induce hypoxaemia.4 5 Neither did the emerging epidemiological profile of SIDS deaths from the United States fit with the theory of suffocation as the peak age of deaths was not during the vulnerable first few weeks after birth but at 3 months of age and although there was a winter preponderance the highest incidence occurred among the black population in the warmer southern states where infants used fewer or lighter bedclothes.4
After many years of research there is growing evidence that SIDS is more likely to be a consequence of a wide range of infant and environmental interactions than due to one particular cause. Head covering may be part of a chain of events for some of these deaths and suggested causal mechanisms include mechanical occlusion of the airways, rebreathing of expired air (both of which could lead to hypoxia or hypercapnoea) and thermal stress (leading to generalised or localised hyperthermia). This is a systematic review of the prevalence of head covering among victims of SIDS and age-matched control infants and an evaluation of how far the associated risk agrees with the epidemiological evidence.
METHODS
We have attempted to follow the MOOSE guidelines for systematic reviews.6 Customised databases at both collaborating research centres were utilised along with PubMed, which includes Medline and Old Medline citations. The primary search used the term SIDS with words describing the risk factor (“head”, “cover” or “bedclothes”) or using the generic term “risk factor” for different study designs (“case-control”, “cohort”, “case-series”, “review”). A secondary search of all the references from the relevant papers was also conducted. Potential studies written in languages other than English were included and read for any reference to head covering. Attempts to gain access to unpublished data were made at international conferences within this field and members of the International Society for the Study and Prevention of Infant Death (ISPID), who come from many different countries, were asked if there were additional studies we had not identified. Authors of included studies were contacted if specific numerators or denominators were missing from the published manuscripts.
Over 600 papers were identified along with more than 100 epidemiological investigations. Pre-existing criteria were used for inclusion in the meta-analysis: head covering had to be reported, distinct from other forms of facial occlusion and analysed across the study population, and the study had to be controlled with observations of age-matched infants and conducted between January 1950 and May 2007.
The pooled univariate estimate of the odds ratio was calculated using the Mantel-Haenszel technique.7 The pooled adjusted odds ratio was calculated using the statistical package Review Manager provided by the Cochrane Collaboration.8 The test for heterogeneity of the odds ratios was conducted using Woolf’s method.7
RESULTS
Included studies
Non-English manuscripts of epidemiological studies were found but did not measure head covering, while unpublished findings were sought but not discovered. Studies that had not separated observations of head covering from other forms of facial occlusion, such as infants found face down in the bedding, were excluded from the meta-analysis along with studies that had only reported observations for subgroups of SIDS infants (n = 8).9–16 A further 10 studies reported a population-based prevalence of head covering among SIDS victims but had not collected similar information from control families and thus were also excluded.17–26 Controlled observations of head covering when the SIDS infants were discovered dead or control infants woke up from a reference sleep were found in 10 studies (table 1).27–36
Prevalence and risk
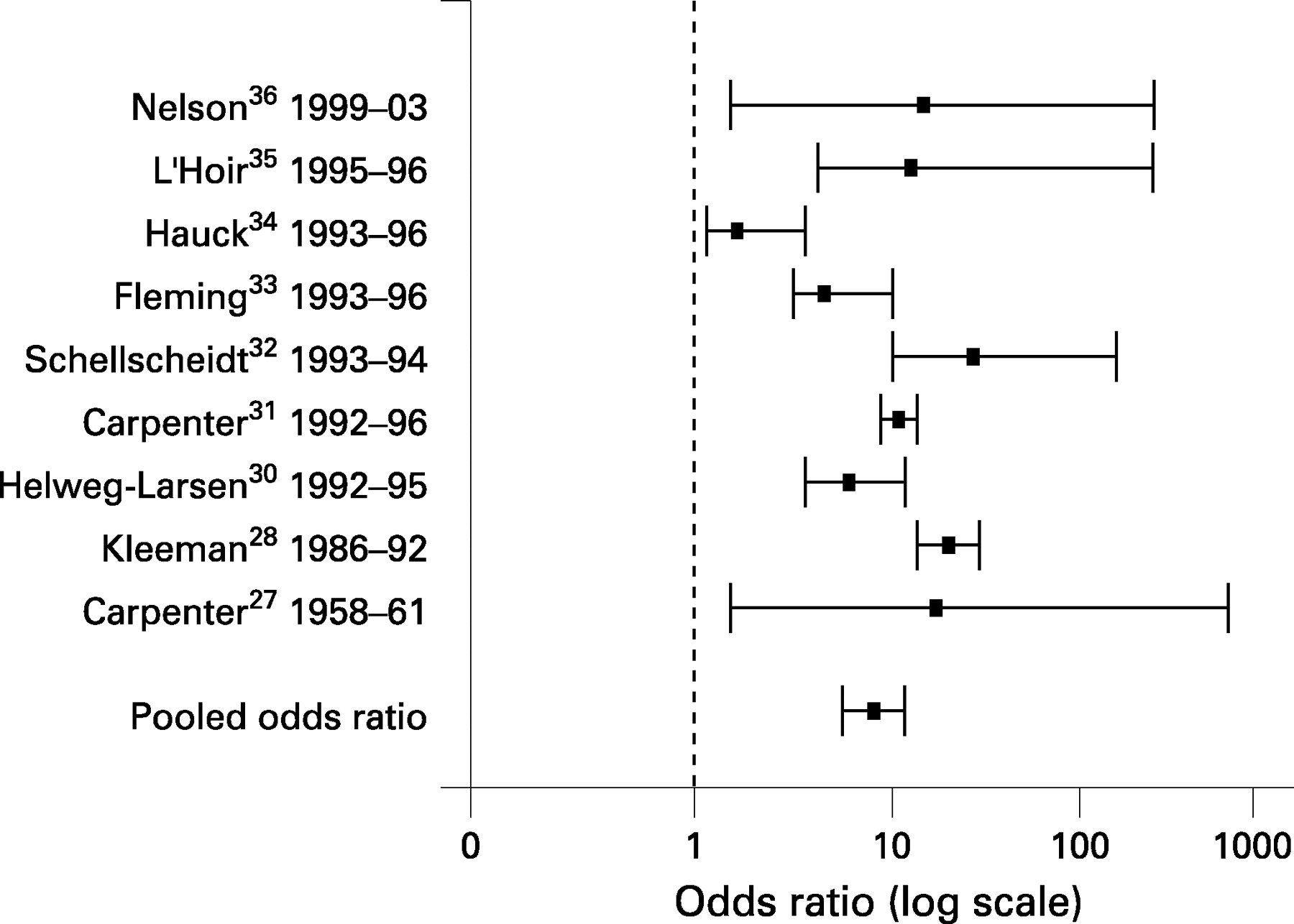
The prevalence of head covering among SIDS victims (table 1) in each study varied from 13% to 48% with a pooled mean prevalence of 24.6% (95% CI 22.3% to 27.1%). The three earliest studies conducted before the major decline in the SIDS rates27–29 reported a higher prevalence of 36.1% (95% CI 30.9% to 41.8%), although head covering remained a consistent feature in subsequent studies with a mean prevalence of 21.0% (95% CI 18.5% to 23.7%). Among the control infants the prevalence of head covering after the reference sleep was much lower, ranging from 0% to 6% with a pooled mean prevalence of 3.2% (95% CI 2.7% to 3.8%).
A test for heterogeneity of the odds ratios between studies suggests the risk associated with head covering was significantly different (p<0.01), although this was in strength rather than direction; the univariate odds ratio varied between two-fold and almost 50-fold but denoted a significant risk in all of the studies (fig 1). The pooled univariate estimate was 9.6 (95% CI 7.9 to 11.7). In seven of the 10 studies the odds ratios for head covering were adjusted for other factors associated with SIDS (all but one of these studies were conducted after the dramatic fall in SIDS rates). The number of adjusted factors and how these were defined varied between studies (see footnote in table 1), but the multivariate risk estimates for head covering remained highly significant in each investigation (fig 2). The pooled adjusted odds ratio was 16.9 (95% CI 12.6 to 22.7). Assuming that head covering is causally related to SIDS, the data from these studies suggest the population attributable risk would be 27.1% (95% CI 24.7% to 29.4%).


Four studies21 24 33 37 also included questions to the parents regarding whether their infant had ever been found previously with bedclothes covering the face or head (table 2). Over a quarter of SIDS and control parents responded that this had occurred at least once prior to the death or reference sleep (26% SIDS vs 27% controls), although for both sets of infants head covering was not described as a common event. The pooled univariate odds ratio for the four studies was 1.0 (95% CI 0.8 to 1.3), while the pooled adjusted odds ratio from just two studies was 1.1 (95% CI 0.9 to 1.4), suggesting no difference in previous instances of head covering between the two groups (fig 3).

{kind=link}
{kind=link}
{kind=link}
Head covering as part of an agonal event
Parental narrative accounts of the deaths and the wider epidemiological evidence do not lend support to the idea that head covering is simply a consequence of some terminal struggle. Although SIDS deaths are mostly unobserved events, it is not uncommon for the parents to be in the same room as the infant and very rare that parents are woken or alerted to the unfolding tragedy. A review of 300 detailed narrative accounts from our own SIDS deaths in Avon over the last 20 years suggests that any change in position is minimal, often described in terms of infants rolling to the prone position or moving down under the bed covers. Reports of observations at the time of death by Gormally and Matthews in Ireland showed that the bedding was undisturbed in over two thirds of SIDS cases.22 These were uncontrolled observations but confirmed by the large European study by Carpenter et al: 71% of the SIDS infants showed no movement between being put down and discovered compared to 70% of the control infants.31 Prospective data of sleep recordings among infants who eventually died of SIDS have shown a reduced number of body movements during sleep, a decreased propensity to arouse from sleep and a lowering of cardiac variability.38 Further data of SIDS infants who actually died while on a monitor show a fall in the heart rate before death and decreased occurrence of partial or complete auto-resuscitation rather than recordings suggestive of an infant struggle.39–41
An alternative explanation might be that head covering is common during infant sleep but the covers are often removed during the process of waking, in which case the lack of movement among SIDS cases may explain the association. However, overnight video recordings in the home setting conducted in New Zealand suggest head covering is rare among infants sleeping in a cot: of 40 infants observed over an 8 h period head covering occurred just once.42
Head covering and the prone sleeping position
In the last 20 years in Avon, England, the proportion of SIDS victims put down to sleep in the prone position has fallen from 89% to 24%, while the SIDS rate has decreased from over 2 to less than 0.5 per 1000 live births.43 The concomitant fall in the use of the prone position may partly explain the slightly reduced prevalence of head covering as some studies have reported that head covering was more common among infants found in the prone sleeping position.29 32 As Beal points out, when older infants start to “crawl” in the prone position, they often move backwards rather than forwards for the first few weeks.44 L’Hoir et al demonstrated that head covered SIDS infants tended to be older and to have moved down under the covers compared to the cases found uncovered,35 an observation confirmed by the study of Fleming et al which also showed that this downward movement was much more common among the covered SIDS infants compared to the covered controls.33 Intriguingly, a recent analysis from New Zealand suggests head covering was associated with a decreased risk for SIDS among prone sleeping infants found face straight down in the mattress.45
A study of healthy infants in the United States put down in the prone position and covered with soft bedding has shown that protective behaviour such as head repositioning strategies were not so much related to infant age as to previous experience of sleeping in the prone position; inexperienced prone sleeping infants tended to nuzzle into the bedding rather than lift or turn their heads.46 A similar study by Skadberg and Markestad showed that the majority of healthy infants sleeping supine and covered with soft bedding used all of their limbs to remove the covers at 5 months old, a quarter achieved the same feat at 10 weeks old, while only one infant out of 23 sleeping prone managed to remove the covers at 5 months old using repeated head movements.47
Head covering and bed sharing
Home studies of healthy infants in New Zealand with overnight video and physiological recordings showed that head covering was more common during sleep among bed-sharing infants than those sleeping alone in a cot, but also that parents tended to adjust the infant covering during the night.42 Data from the UK48 suggest that fewer co-sleeping SIDS infants were discovered head covered (7% vs 19% among solitary sleeping SIDS infants), a finding confirmed by a more recent study in Scotland16 where of 46 SIDS infants sharing the parental bed only three (7%) were found with their head covered. Data from the Scottish study also suggested that previously reported episodes of head covering were less common among both co-sleeping SIDS infants (13%) and controls (20%) compared to the results we report in table 2. This reduced prevalence may indicate a protective effect from the parental presence; a more recent analysis of the UK data suggests twice as many SIDS infants were discovered with the bedclothes covering the head either outside the parental bedroom during the night-time sleep or unsupervised in a room during the day-time sleep.49 Despite these observations bed sharing, particularly among parents who smoke, is strongly associated with SIDS and it would be dangerous to recommend bed sharing as a strategy to reduce the prevalence of head covering.
DISCUSSION
The prevalence of head covering among studies conducted after the fall in SIDS rates suggests that a fifth of SIDS infants are still being discovered with bedclothes covering the face or head. The initial “Back to Sleep” intervention campaign conducted in the UK in 1991 included advice for parents to avoid infant head covering, but this seems to have had far less impact than the campaign’s main message regarding infant sleeping position. The pooled adjusted estimate suggests an almost 17-fold increased risk associated with head covering, five times higher than pooled estimates for prone sleeping50 and maternal smoking51 and eight times higher than estimates for other potential risk factors such as bed sharing,52 bottle feeding53 and infants not being given a pacifier.54 This pooled estimate should be treated with caution because of the lack of homogeneity among the reported odds ratios. There are too few studies to meaningfully explore the differences in estimated risk, but the strength of the findings, all in one direction, suggest the risk associated with head covering is extremely high.
Causal mechanisms
The epidemiological evidence does not give credence to the idea that head covering is just part of a terminal event but neither is it wholly supportive of the currently proposed causal mechanisms. The lack of consensus as to why head covering may put a vulnerable infant at risk is equally applicable to arguments surrounding prone sleeping and perhaps reflects both our limited understanding of infant physiology and the current scarcity of more sensitive or specific pathological investigations.
Hypoxia is thought to play a role in the deaths of infants found prone with the head down in soft bedding, but the role it plays among SIDS victims found under the bedclothes is less clear. SIDS infants are sometimes found face down and sometimes under the bedclothes, but results from New Zealand suggest infants found both face down and head covered are less common.45 The early claims by Woolley4 and Bowden5 that a child cannot be suffocated by “ordinary bedclothes” has been described as anecdotal55 56 but has yet to be refuted. Permeability tests for airflow through various bedding materials suggest little resistance. Duvets perform slightly better than conventional blankets and although the resistance increased with unwashed and wet bedding, British Standards Institution tests suggest it should not pose a threat to the life of a “normal” infant.57
An alternative, but related, explanation involves the inadequate dispersion of exhaled air around the vicinity of the face of the sleeping infant leading to a significant accumulation of carbon dioxide (CO2). An in depth review is given by Guntheroth and Spiers58 who conclude that current evidence does not make for a credible case. SIDS is associated with soft bedding, but the soft surfaces implicated by Kemp and Thach that may facilitate an accumulation of CO2, such as polystyrene-filled cushions,59 sheepskins60 and ti-tree bark61 mattresses, are not commonly used and any association needs to be demonstrated with controlled observations. The findings by L’Hoir et al of a highly significant interaction between duvets and head covering35 are not supportive of the rebreathing hypothesis, given that duvets are more permeable than conventional blankets. Malcolm et al also found that the presence of a pacifier (dummy) promoted an excess of CO2 in the inspired air, yet the epidemiological evidence suggests pacifiers may lower the risk of SIDS.62
What is already known on this topic
Some SIDS victims are found with their heads covered by bedclothes, but it is not clear whether this is just a consequence of the terminal event or a contributory factor to the death involving potential mechanisms such as hypoxia, hypercapnoea or thermal stress.
What this study adds
The risk associated with head covering has consistently been significant across studies: a quarter of SIDS infants are found with their head under the bedclothes, an eightfold difference compared to age-matched controls.
The epidemiology of SIDS does not fully support one particular causal chain but neither does it suggest that head covering is just part of some agonal event.
If the relationship is causal, approximately one quarter of SIDS deaths might be prevented if head covering was avoided.
Another potential mechanism of causality involves heat stress. Excessive clothing and bedding, warmer rooms, reduced ventilation and infections are all associated with SIDS deaths. A history of profuse sweating has been reported among SIDS victims,63–65 although the patho-physiological basis for heat stress in SIDS remains to be determined. The infant head is the site of 40% of heat production and for an infant up to 85% of total heat loss is through the face or head. Covers rising up over the head could therefore result in acute thermal imbalance with a rise in brain temperature not necessarily accompanied by a rise in body temperature.66 Franco et al have shown among healthy sleeping infants that covering of the infant’s face with a bed sheet, although associated with only mild increases in body temperature, induces significant changes in cardio-respiratory and autonomic parameters.67 In the study by Kleemann et al28 head covered infants tended to show signs of profuse sweating, an association also reported by Carpenter et al,31 which agrees with the interaction found by L’Hoir et al of head covered infants found under duvets35 which may be more permeable57 but have greater heat insulation than conventional covers. Thicker covers are commonly used more often during the colder months, but incongruous to all these findings is the fact that the winter peaks of SIDS deaths have substantially diminished at a time when the prevalence of head covered SIDS infants is still quite high.
Parental advice
In the UK the “Feet to Foot” campaign, advising parents to place the feet of the infant at the foot of the cot to prevent head covering, was launched by the Foundation for the Study of Infant Death in 1997 and has subsequently been endorsed by the American Academy of Pediatrics (AAP).68 Although this advice seems intuitively sensible there is, as yet, no published evidence available that this practice reduces the risk of head covering or lowers the risk of SIDS.69 Findings from the study by L’Hoir et al35 suggest that a lightweight cotton sleeping sack (“trappelzak”) used by the majority of Dutch parents may be protective against SIDS both in terms of preventing the infant from turning prone and avoiding head covering. Further evidence than just this one study may be needed but such a practice deserves closer scrutiny given the continued low SIDS rates in Holland.
SUMMARY
The population attributable risk suggests that more that a quarter of SIDS deaths might be avoided if the possibility of infant head covering were eliminated. Similar to the prone sleeping position, head covering is a modifiable risk factor with a potential for further reducing SIDS deaths despite a lack of a complete explanation for the causal mechanism involved.
Acknowledgments
Dr Peter Blair is funded by the Foundation for the Study of Infant death (FSID) in the UK and Professor Edwin Mitchell is supported by the Child Health Research Foundation in New Zealand.
REFERENCES
Footnotes
Competing interests: None.