Article Text

Abstract
Background: Persisting neurological and cognitive impairments are common after cerebral malaria. Although risk factors for gross deficits on discharge have been described, few studies have examined those associated with persistent impairments.
Methods: The risk factors for impairments following cerebral malaria were determined by examining hospital records of 143 children aged 6–9 years, previously admitted with cerebral malaria, who were assessed at least 20 months after discharge to detect motor, speech and language, and other cognitive (memory, attention, and non-verbal functioning) impairments.
Results: The median age on admission was 30 months (IQR 19–42) and the median time from discharge to assessment was 64 months (IQR 40–78). Thirty four children (23.8%) were defined as having impairments: 14 (9.8%) in motor, 16 (11.2%) in speech and language, and 20 (14.0%) in other cognitive functions. Previous seizures (OR 5.6, 95% CI 2.0 to 16.0), deep coma on admission (OR 28.8, 95% CI 3.0 to 280), focal neurological signs observed during admission (OR 4.6, 95% CI 1.1 to 19.6), and neurological deficits on discharge (OR 4.5, 95% CI 1.4 to 13.8) were independently associated with persisting impairments. In addition, multiple seizures were associated with motor impairment, age <3 years, severe malnutrition, features of intracranial hypertension, and hypoglycaemia with language impairments, while prolonged coma, severe malnutrition, and hypoglycaemia were associated with impairments in other cognitive functions.
Conclusions: Risk factors for persisting neurological and cognitive impairments following cerebral malaria include multiple seizures, deep/prolonged coma, hypoglycaemia, and clinical features of intracranial hypertension. Although there are overlaps in impaired functions and risk factors, the differences in risk factors for specific functions may suggest separate mechanisms for neuronal damage. These factors could form the basis of future preventive strategies for persisting impairments.
- ABM, acute bacterial meningitis
- BCS, Blantyre coma score
- CM, cerebral malaria
- IQR, interquartile range
- risk factors
- persisting neurological and cognitive impairments
- cerebral malaria
Statistics from Altmetric.com
Worldwide, Plasmodium falciparum malaria is a leading cause of ill health. About 2 billion people are exposed to P falciparum malaria annually, resulting in over 500 million clinical attacks and about a million deaths, predominantly in children less than 5 years living in sub-Saharan Africa.1
Cerebral malaria (CM) is the most severe neurological complication of malaria. Even with appropriate anti-malarial treatment, 18.6% of patients die and 11% have gross neurological deficits detectable on discharge.2 Due to the high mortality and limited means of detecting impairments in many resource-poor settings, the long term effects of the disease have been poorly documented. However, given the magnitude of the problem, an enormous number of children may be at risk of impairments, with adverse educational and social consequences.3–5 Indeed our recent studies in Kenyan children described persistent neurological and cognitive impairments in 24% of those who survived CM up to nine years after the episode.6,7
Risk factors for the development of neurological and cognitive deficits have been described.3,8,9,10,11,12 However, these studies have generally not differentiated between impairments of different functions but classified patients as either having impairments or not. Analysis of risk factors for impairments has not examined the possibility of differences in impaired functions, whereas an alternative strategy of examining risk factors for individual functions may help elucidate the pathogenesis of impairments. In this study, we used a cohort of Kenyan children (who had been exposed to CM and been assessed for long term impairments) reported previously6,7 and examined clinical characteristics during hospital admission that are predictive of persistent impairments in motor, language, and other cognitive functions.
METHODS
Study design
We compared a cohort of children who had survived the acute stage of CM to a similar group of children unexposed to severe malaria. This was part of a larger study investigating the effects of severe falciparum malaria on the neurological and cognitive functioning of children. Unlike earlier reports from this study,6,7,13 we examined some of the antecedent events that may constitute risk factors for impairments.
Setting
Participants were recruited from the Kilifi demographic surveillance area on the coast of Kenya. Kilifi District Hospital is the only hospital in the area, where the majority of very sick children are admitted for treatment. The characteristics of the study area have been described elsewhere.14,15
Participants
Study participants were identified from the hospital’s admissions database, born between 1991 and 1995 and living in the study area. The study children had previously been exposed to CM; clinical data were collected prospectively during admission. Exposure to CM was defined as admission to hospital in coma with inability to localise a painful stimulus, a Blantyre coma score (BCS) ⩽2,8 asexual forms of falciparum malaria on a blood smear, and no evidence of pyogenic meningitis on examination of the cerebrospinal fluid.16 As a comparison, we drew a random sample of children unexposed to severe malaria from a census database of children living in the study area.
At the time of assessment, all participants were 6–9 years old. This age group was chosen since the tests we used can assess cognition, speech, and language more reliably above the age of 6 years. All spoke a Mijikenda language as their first language. Children were excluded if they refused verbal assent or their parents refused written informed consent. We obtained ethical permission for the study from the Kenya Medical Research Institute Scientific and Ethical Review Committees and from the Institute of Child Health, UK.
Neurological and cognitive assessment
The neurological and cognitive assessments have been described in detail elsewhere.8 All children underwent the same battery of assessments for motor skills, behaviour, cognition, hearing, and vision. Assessors were blinded to the participants’ exposure status. Cognitive assessment included tests of memory based on the Rivermead Behavioural Memory Test for Children,17 attention (visual search), a parental rating of behaviour problems, and non-verbal functioning (construction tasks such as copying shapes using drawings, blocks, or sticks to assess the coordination of complex cognitive tasks).3 Speech and language assessments covered eight major areas of language: receptive grammar and vocabulary, lexical semantics (expressive vocabulary), syntax/morphology, pragmatics (language use), phonology, higher level language, and word finding.7,18 The neurological assessment comprised a measure of motor skills based on a system for classifying motor function in children with cerebral palsy.19 This is a five-level grading of motor deficits developed for use in clinical practice, research, and teaching and comprises an assessment of cranial nerve function and motor function (using a hierarchical classification of spasticity, ataxia, and fine motor dysfunction). Hearing was tested with a Kamplex screening audiometer (P.C. Werth, London, UK), and vision was tested using a Sonksen-Silver chart.20
Nutritional status was assessed using weight for age z-scores (WAZ) calculated using the NutStat program in EpiInfo 2000 (CDC, Atlanta, GA, USA). Socioeconomic status was assessed using mother’s level of education, which is often regarded as a predictor of child health and development,21 and father’s occupation, which has been found to be associated with income level in previous studies on the Kenyan coast.22
Data management
Standard clinical classifications were used to ascertain levels of impairment in neurological, hearing, and visual assessments.17,19,20 The scoring system of the behaviour questionnaire was used in a previous study.3 Language, memory, and non-verbal functioning assessments were not standardised on the local population, therefore impairment was classified using a commonly accepted classification of ability levels.23 An estimate more than 2 standard deviations below the age specific unexposed group mean or the 2.0 centile of the unexposed group results was adopted for normally distributed and skewed data respectively. A classification of “speech and language impairment” was defined as an impairment level score on two or more of the language assessments, while a designation of “impairment in other cognitive functions” described children with impairment level performance in any one of memory, attention, or non-verbal functioning.6,7
Statistical analysis
Statistical analysis was carried out using SPSS version 11.5 (Chicago, IL, USA). Patients were classified as impaired or non-impaired. For univariate analysis, admission clinical characteristics of children defined to have impairments were compared to those without impairments to identify risk factors for any impairment. Categorical variables were compared using Pearson’s χ2 or Fisher’s exact test (two tailed) as appropriate. The means of normally distributed data were compared with Student’s t test and the median used for skewed data. All variables with a p value <0.25 at univariate analysis were included in a logistic regression analysis to identify risk factors independently associated with persisting impairments; only those with a p value <0.05 were retained in the model. An a priori decision was made to include age in each model due to possible confounding effects of age at which the child was exposed to CM on the risk of neuronal damage: children were categorised as aged <3 or ⩾3 years at the time of exposure. Separate regression analyses were then performed for motor, speech and language, and other cognitive impairments to identify risk factors independently associated with each function. Similar analyses were performed to identify risk factors for impairments in memory, attention, or non-verbal functioning. The Bonferroni correction was performed to allow for multiple corrections.
RESULTS
General description of study subjects
Two hundred and forty four children who fulfilled the criteria for CM, and 273 children unexposed to severe malaria were identified from the databases. Of these, 20 children (14 (5.7%) CM and 6 (2.2%) unexposed, p = 0.037) had died. Eighteen children (6 CM and 12 unexposed) did not fulfil the age requirements and were excluded (dates of birth reported at the time of admission were erroneous). One hundred and forty eight children (72 CM and 76 unexposed) had migrated out of the study area. A total of 331 (152 CM and 179 unexposed) children were eligible for recruitment.
Of the eligible children exposed to CM, those with incomplete records, who presented with evidence for other causes of the encephalopathy or significant developmental impairments before the admission with CM were excluded (a total of nine children). These included one child with hemiplegia and delayed speech following birth asphyxia, four with incomplete records, and four with evidence of other encephalopathies. Of the remaining 143 children, 74 (51.7%) were male. The age and sex distribution of children in the two groups was similar. The median age at which the children were admitted with CM was 30 months (IQR 19–42) and the median time from discharge to assessment was 64 months (IQR 40–78).
Prevalence and types of impairments
Thirty four children exposed to CM (23.8%) and 18 unexposed children (10.1%) were defined to have impairments in at least one function. Of those functions measured, persisting impairments were most common in motor, speech and language, and memory functions (table 1).
Prevalence and types of persisting neurological and cognitive impairments following cerebral malaria
Overlap of impaired functions in children exposed to cerebral malaria
Some children with impaired functions had deficits in more than one function; 15 (42%) of the CM children with impairments had two or more impairments compared to 4 (22%) of the unexposed children. Multiple impairments were observed in clusters of language, memory, and/or motor functions (fig 1). Non-verbal functioning and behaviour were less often impaired relative to other functions in children with CM. Multiple impairments were particularly common among those who also had active epilepsy. Details of these impairments are described elsewhere.6,7,13

Overlap of impaired functions among 34 children defined to have persistent impairments following cerebral malaria.
Risk factors for persistent impairments after cerebral malaria
We compared the past medical history and the clinical characteristics at the time of admission of children exposed to CM defined to have impairments to those without impairments. In both groups, the median duration of illness was 3 days. There were no differences between children who developed impairments and those who did not in mother’s years of formal education, father’s income, sex, or head circumference. Univariate analysis showed that a history of previous seizures, deep coma, hypoglycaemia, partial or multiple seizures in the ward, prolonged coma after admission, or neurological deficits on discharge were significantly associated with impairments (table 2).
Clinical characteristics of study participants at the time of admission with cerebral malaria
Although the mean admission temperatures were similar, a higher proportion of children defined to have impairments were admitted without a history of fever. The risk of impairments was increased in those with deeper coma: 5/6 (83%) children with a BCS = 0 had impairments compared to 5/18 (28%) of those with a BCS = 1 and 24/119 (20%) of those with a BCS = 2. The mean serum sodium was also higher in those with impairments, even though there was only one child with hypernatraemia. Children with impairments had a slower recovery from coma, with a median time to full consciousness about 8 hours longer than those without impairments.
Independent risk factors for any impairment
In a logistic regression analysis, previous history of seizures, deep coma at admission, focal neurological signs, and neurological deficits at discharge were identified as factors independently predictive of any impairment (table 3).
Risk factors independently associated with persisting neurological and cognitive impairments following cerebral malaria
-
Motor impairment. Previous admissions, focal neurological signs, and multiple seizures during the course of admission were independently associated with persisting motor impairments.
-
Speech and language impairment. Age <3 years, previous history of seizures, brain stem and fundoscopic evidence of raised intracranial pressure, hypoglycaemia, and prolonged coma after admission were independently associated with persisting language impairments.
-
Impairment in other cognitive functions. Previous seizures, deep coma on admission, and prolonged coma after admission were independently associated with the development of impairment in other cognitive functions. When we examined risk factors for impairment in different functions, deep coma (adjusted OR 40.6, 95% CI 2.8 to 583, p = 0.006) and severe malnutrition (WAZ <−3.0, adjusted OR 23.0, 95% CI 2.2 to 245, p = 0.009) were found to be independently associated with impaired attention. Lack of a history of fever (adjusted OR 7.9, 95% CI 1.3 to 49.6, p = 0.028), deep coma (adjusted OR 16.1, 95% CI 2.3 to 112, p = 0.005), and prolonged coma after admission (adjusted OR 6.4, 95% CI 1.6 to 25.1, p = 0.008) were associated with memory impairment. Hypoglycaemia was associated with impairment of non-verbal functioning (adjusted OR 1.1, 95% CI 1.0 to 1.2, p = 0.015). No association was observed between impairment in these cognitive functions and either focal neurological signs or neurological deficits at discharge.
When the Bonferroni correction was applied to adjust for multiple comparisons, motor impairment was still associated with multiple seizures, language impairment with previous seizures, severe malnutrition, and hypoglycaemia, while impairments in other cognitive functions were associated with deep coma.
DISCUSSION
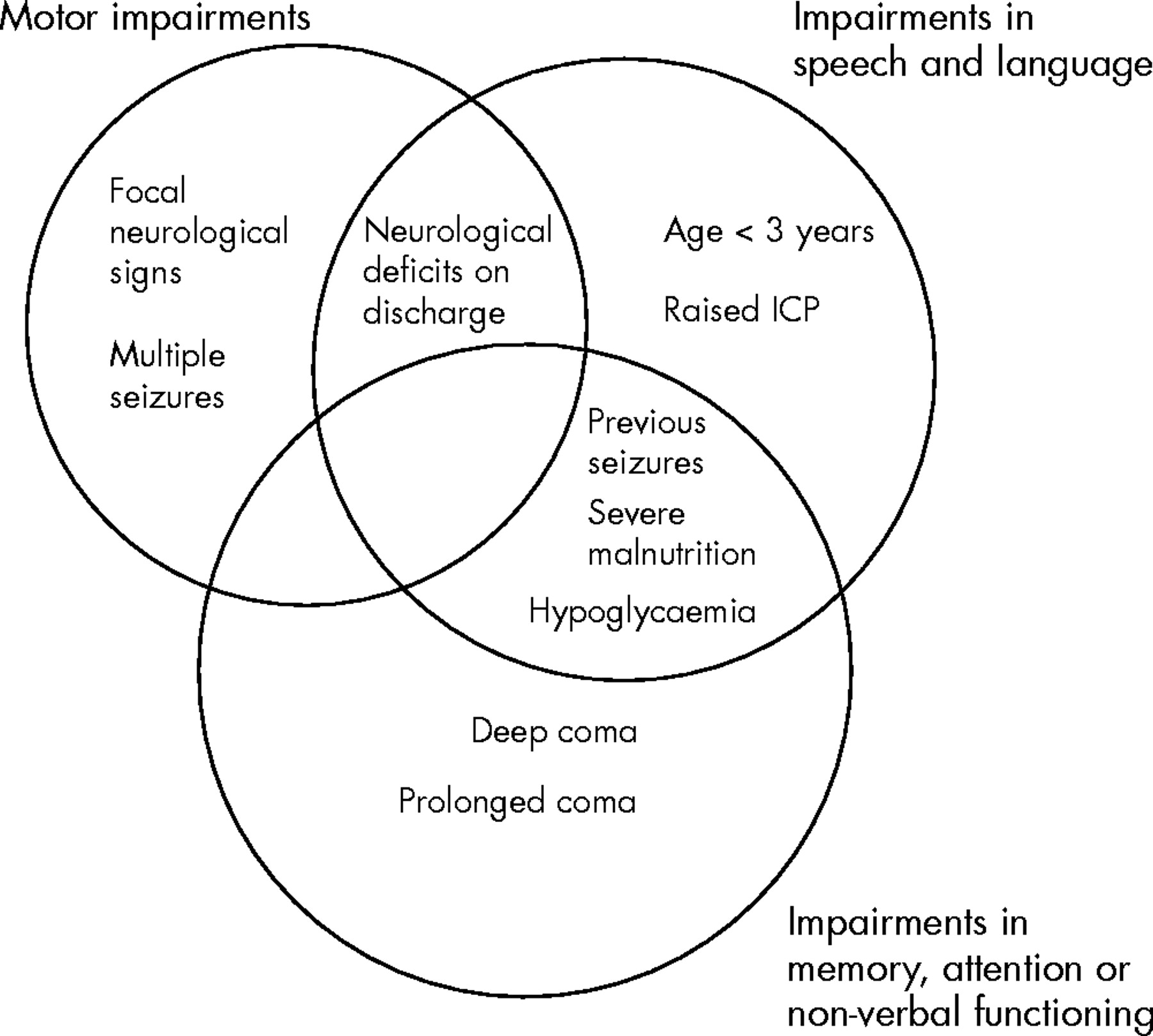
The aim of this study was to describe clinical risk factors during the acute phase of CM that are predictive of different types of persistent neurological and cognitive impairments. We found that previous seizures, deep coma on admission, focal neurological signs during hospital admission, and neurological deficits on discharge are predictive of the development of persistent impairments after CM. In addition, age <3 years, previous admissions, multiple seizures, hypoglycaemia, raised intracranial pressure, and prolonged coma are associated with specific impairments. These risk factors differed according to the function impaired (fig 2).

{kind=link}
{kind=link}
Risk factors associated with persisting motor, speech and language, and other cognitive impairments.
Risk factors for long term impairments following cerebral malaria
We were unable to locate almost 30% of the children identified from the hospital’s database, mostly as a result of migration. It is possible that some died, especially those who had severe impairments.5 Despite this, risk factors for impairments in specific functions could be identified.
Risk factors for impaired motor function
Children with motor impairments were more likely to have had previous admissions with seizures and focal neurological signs or multiple seizures during hospital admission. Seizures are common precipitators of admission: it is probable that each episode cumulatively increases the risk of focal neurological damage and that on subsequent visits, patients present with multiple seizures, focal neurological signs, and motor impairment.10
Risk factors for speech and language impairments
Children who developed language impairments were more likely to have been young (<3 years), or had hypoglycaemia, severe malnutrition, or raised intracranial pressure at the time of admission or neurological deficits on discharge. This would suggest that language impairment develops in children who suffer a more severe encephalopathy (patients with hypoglycaemia or raised intracranial pressure) at a young age and in those who had been exposed to long term nutritional deprivation.24 It is also possible however that, these deficits are a manifestation of global cerebral damage rather than injury to a specific area of the brain given the wide range of risk factors associated with language. Indeed, the overlap of language deficits with impairments in motor and other cognitive functions in some patients supports this suggestion. Impairment in one function may also worsen the outcome in another. Overlap of impairments in language and other cognitive functions (fig 1) therefore could have arisen from the secondary effects of impaired memory and attention (which had sizeable verbal components in terms of instructions, teaching elements, or response formats), while some of the other language difficulties could have been due to impaired motor function.25
Impairments in other cognitive functions
This study confirms previous reports of an association between deep coma on admission or prolonged coma after admission and cognitive impairment after CM.3,26 In addition, it suggests that previous episodes of seizures increase the risk of cognitive impairment. Hypoglycaemia and absence of hyperpyrexia have been associated with impaired cognition.3 Our findings appear to confirm this; hypoglycaemia was associated with impairment of non-verbal functioning but instead of absence of hyperpyrexia, we observed that children who failed to mount a febrile response (no history of fever before admission) had an increased risk of developing memory impairment. A recent study found impaired prostaglandin E2 (PGE2) metabolism in some children with CM and this was associated with poor outcome.27 Prostaglandins are important mediators of fever, macrophage activity, and pro-inflammatory responses to infection. The failure to mount a febrile response that we observed may be due to the impaired PGE2 metabolism in children with CM. It is however not clear which mechanisms are involved in the impaired PGE2 metabolism and impaired cognitive function.
Risk factors for impairments and the pathogenesis of cerebral malaria
Cerebral malaria is a diffuse encephalopathy characterised by sequestration of Plasmodium falciparum in cerebral capillaries.28 Due to the diffuse nature, deficits are likely to involve more than one function3 and survivors of the more severe forms are likely to suffer greater neuronal damage. Children who develop CM in early childhood (before the age of 3 years), during the period of brain development and organisation are likely to suffer more severe and lasting neurological damage.26,29 Differences in risk factors for impairments in each function suggest separate pathogenic mechanisms. Each risk factor may influence different functions with differing degrees of severity (fig 2). In addition, some cognitive functions such as language may be affected by external factors such as the child’s nutritional state at the time of the encephalopathy.30,31
What is already known on this topic
-
Cerebral malaria is associated with persisting neurological and cognitive impairments in children
-
Risk factors for such impairments include deep coma, hypoglycaemia, absence of hyperpyrexia, and neurological deficits on discharge
In a systematic review of neurological and cognitive impairments associated with common central nervous system infections, Carter and colleagues32 found a pattern to suggest a low mortality and morbidity following viral meningitis. Both acute bacterial meningitis (ABM) and CM were associated with high mortality, but those exposed to ABM had a higher prevalence of long term impairments. The risk of impairments after ABM was greatest for, but not confined to, those who had acute neurological complications such as coma. The results of our study suggest that some pre-existing factors, namely previous seizures and admissions, are related to outcome even though children with obvious impairments reported at the time of admission were excluded. However, just like ABM,32,33 the data clearly showed that markers of the severity of CM encephalopathy such as multiple seizures, deep or prolonged coma, hypoglycaemia, or raised intracranial pressure, independently correlated with neurological and cognitive impairments, supporting a causative relation between CM and these impairments. The risk factors we describe are similar to that found in earlier CM studies.3,9,11 The prolonged time to full consciousness in children with impairments points to the severity of the encephalopathy they had been exposed to. Deep coma too was strongly associated with impairment, even though few patients had this level of coma. Over 80% of the patients with deep coma developed cognitive impairment. Higher mortality rates have previously been described among children with deep coma.8,10,16,34 Mortality and poor neurological and cognitive outcomes therefore seem to form a continuum, with surviving patients suffering significant neurological damage leading to long term deficits. The risk factors we have identified in this study may be used to select children at risk of developing impairments so that they are followed up to detect and possibly manage these impairments. The same risk factors may also be used to develop intervention programmes.
The proportion of children with impairments in the unexposed group (10.1%) is comparable to that found in another resource poor country, Bangladesh (7% of 2–9 year olds).35 Although this study cannot completely exclude the effects of insults such as iron deficiency on cognition, the differences we observed are unlikely to be due to iron deficiency at the time of admission since the mean red cell volumes in both groups were similar. There too was no association between haemoglobin level or severe anaemia at admission and long term cognitive impairments.
What this study adds
-
Persisting impairments are in addition associated with a history of previous seizures, young age at the time of exposure, severe malnutrition, multiple seizures, focal neurological signs, or features of raised intracranial pressure observed during admission and prolonged coma
-
There are differences in risk factors for impairment of different functions, suggesting separate mechanisms in the causation of neurological damage
Conclusion
In conclusion, persisting impairments in neurological and cognitive functions are associated with childhood cerebral malaria. Although overlaps exist, specific risk factors can be identified for impairment in each function, suggesting that different mechanisms may be responsible. Children with such risk factors should be followed up to look for persistent impairments. The same risk factors may also be useful in identifying interventions to prevent their development during admission, for example prophylactic anticonvulsants.
Acknowledgments
We thank the assessment team, in particular Joseph Gona, Gladys Murira, Elizabeth Obiero, Khamis Katana, Kenneth Rimba, and Judy Tumaini; and the records officers Ramos Kazungu and Josephene Kazungu. This paper is published with the permission of the director of KEMRI.
REFERENCES
Footnotes
-
Published Online First 2 December 2005
-
Funding: Dr Carter and Professor Newton are supported by the Wellcome Trust (grants 059336 and 070114 respectively)
-
Competing interests: none