Article Text

Abstract
Aim: To determine incidence, aetiology, and clinical features of subdural haematoma and effusion (SDH/E) in infancy throughout the British Isles.
Methods: Cases were notified to the British Paediatric Surveillance Unit over 12 months by paediatricians, neurosurgeons, and paediatric and forensic pathologists.
Results: A total of 186 infants (121 boys, 65 girls) aged 0–2 years were identified. Annual incidence of SDH/E for the UK and Republic of Ireland is 12.54/100 000 aged 0–2 (95% CI 10.3 to 14.62) and 24.1/100 000 aged 0–1 (95% CI 20.89 to 28.18). A total of 106 infants suffered non-accidental head injury (NAHI), 7 accidental head injury, 26 a perinatal cause, 7 a non-traumatic medical condition, 23 meningitis, and in 17 the cause was undetermined; 35 infants died. Significant differences were found in injury pattern, body weight, and Townsend score between NAHI and SDH/E from other cause. There were fewer diagnostic investigations in non-NAHI cases. Delay in diagnosis of greater than a week occurred in 48/181.
Conclusion: SDH/E is a significant cause of morbidity and mortality in infancy. NAHI is the predominant cause of SDH/E. SDH/E can present in a non-specific and varied way and must be considered in any infant who is unwell. Determining the cause of the SDH/E in some cases continues to present a diagnostic challenge.
- NAHI, non-accidental head injury
- SDH/E, subdural haematoma and effusion
- subdural haematoma
- subdural effusion
- infancy
- non-accidental head injury
- neurodevelopmental outcome
Statistics from Altmetric.com
Subdural haematoma and effusion (SDH/E) is a significant cause of morbidity and mortality in infancy. Previous UK incidence studies of SDH/E were restricted to smaller geographical areas1,2 and focused principally on non-accidental head injury (NAHI). Although an association between SDH/E and NAHI is well established,3–,7 other causes must be considered. Diagnosis can present difficulties and may be delayed.8 This study aimed to describe the immediate clinical presentation and management of infants up to age 2 years with subdural haemorrhage or effusion from any cause identified by conventional imaging techniques or at postmortem examination.
METHODS
Paediatricians, neurosurgeons, and paediatric and forensic pathologists from the UK and Republic of Ireland were invited to report all cases of SDH/E in children less than 2 years of age at the time of diagnosis. Cases diagnosed in the preceding month were reported using the monthly reporting card through the British Paediatric Surveillance Unit (BPSU), an established system for the surveillance of uncommon and rare paediatric conditions.9 The study period was from 1 April 1998 to 31 March 1999. A questionnaire was sent out by the investigators to the reporting clinician on receipt of the notification by the BPSU requesting details of history, clinical presentation, diagnosis, and management.
Information was sought regarding the following investigations recommended in SDH/E:1 full multidisciplinary social investigation, examination by an ophthalmologist, skeletal survey, coagulation screen, and radiological assessment by computed tomography (CT) or magnetic resonance imaging (MRI). The doctor was asked, “Taking all the information into consideration, what was judged to be the aetiology of the SDH/E?”. Cases including duplicate notifications were uniquely identified by initials, postcode, and date of birth. Additional checks for deceased infants were made with the Office of National Statistics (ONS), and where appropriate, information including postmortem reports was sought from the local coroner. No contact with the family was made. Ethical approval was obtained via the investigator’s local ethical committee.
Postcodes were used to derive Townsend scores.10 Weight standard deviation scores (SD) were calculated using “L Grow” software11 derived from British and French standards. Comparison of Townsend scores and weight SD scores for NAHI and the remainder were made using a Mann-Whitney U test and t test respectively. A total population estimate for the population of children aged 0–2 years was obtained for mid-1998 from the Office of National Statistics.
Case definition
The definition used was “any child under 2 years at diagnosis with subdural haemorrhage, haematoma, or effusion (collection of protein rich fluid of greater than CSF density) of any severity, arising from whatever cause and diagnosed on CT, MRI, or ultrasound scan or at postmortem examination”. Radiological reports but not radiographs were sought.
RESULTS
From 372 notifications, 186 cases were identified (121 boys, 65 girls). Cases excluded comprised 80 duplicate notifications and 54 who presented outside the study period, the child was older than 2 years, or a diagnosis of SDH/E was not confirmed. Fifty two questionnaires were not returned despite repeat requests. The reasons cannot be identified although duplicate notification was felt to be important as it was usual for several consultants to be involved in a case.
The annual incidence of SDH/E for ages 0–1, 1–2, and 0–2 is given in table 1⇓.
The annual incidence of SDH/E in the British Isles*
Table 2⇓ describes key features of the cases grouped according to reporting clinicians’ stated aetiology of the SDH/E. This opinion was based on the clinical history, examination, and investigations which in some cases included a child protection investigation. The causes were NAHI (n = 106), accident (n = 7), perinatal (n = 26), miscellaneous other disease (n = 7), meningitis (n = 23), and undetermined (n = 17). The majority were either dead (n = 4) or severely ill (n = 111) at presentation. However, 65 were well and presented with non-specific symptoms. At presentation 88 were resuscitated. Table 3⇓ describes the presenting symptoms and signs. Carers provided a history of minor injury in 41/97 cases of NAHI and in 2/16 undetermined cases.
SDH/E: aetiology versus various parameters
Symptoms and signs in SDH/E
Evidence of other injury included retinal haemorrhages in 59/168 infants who received a retinal examination (54/168 examined by a paediatrician only and 114 by an ophthalmologist) (table 2⇑). In 46 the haemorrhage was bilateral, in 11 unilateral (6 left, 5 right), and unknown in 2. The distribution and incidence of other injury by aetiology is shown in table 4⇓.
Bruises and fractures in accident, NAHI, and perinatal groups
Mean weight standard deviation (SD) score at diagnosis for 159/186 cases was –0.68 for abuse and –0.25 for non-abuse (p = 0.02). Fourteen of 94 in the NAHI group had weights of −2 standard deviations from the mean, indicating failure to thrive, compared with 5/65 in the non-abused group.
Investigation and diagnosis
Diagnosis was made within one week of initial presentation in 133, while delay of over one week occurred in 48/181. Neuroimaging studies performed were head CT alone (n = 83), head MRI alone (n = 19), head CT and MRI (n = 69), and head ultrasound alone (n = 3). Primary diagnosis at postmortem examination was made in 12. The site of the SDH/E was unilateral (n = 45), bilateral (n = 133), and unknown (n = 8). Radiological reports suggested collections of different ages in 46 infants.
Selected key investigations performed according to aetiology are shown in table 5⇓. Mean haemoglobin level (Hb) for 166 infants was 103 g/l (range 35–197 g/l). Hb was within the normal range in 71 and below 2 standard deviations of the age related mean in 95.12 CSF taps were performed in 117 infants (62 subdural, 55 lumbar). CSF, where reported, was clear (n = 9), bloody (n = 50), xanthochromic (n = 18), and turbid (n = 18). Death occurred in 14 girls and 21 boys, average age 16.9 weeks, median 12 weeks; postmortem reports were available for 24.
Selected key investigations in SDH/E by aetiology
Family and social details
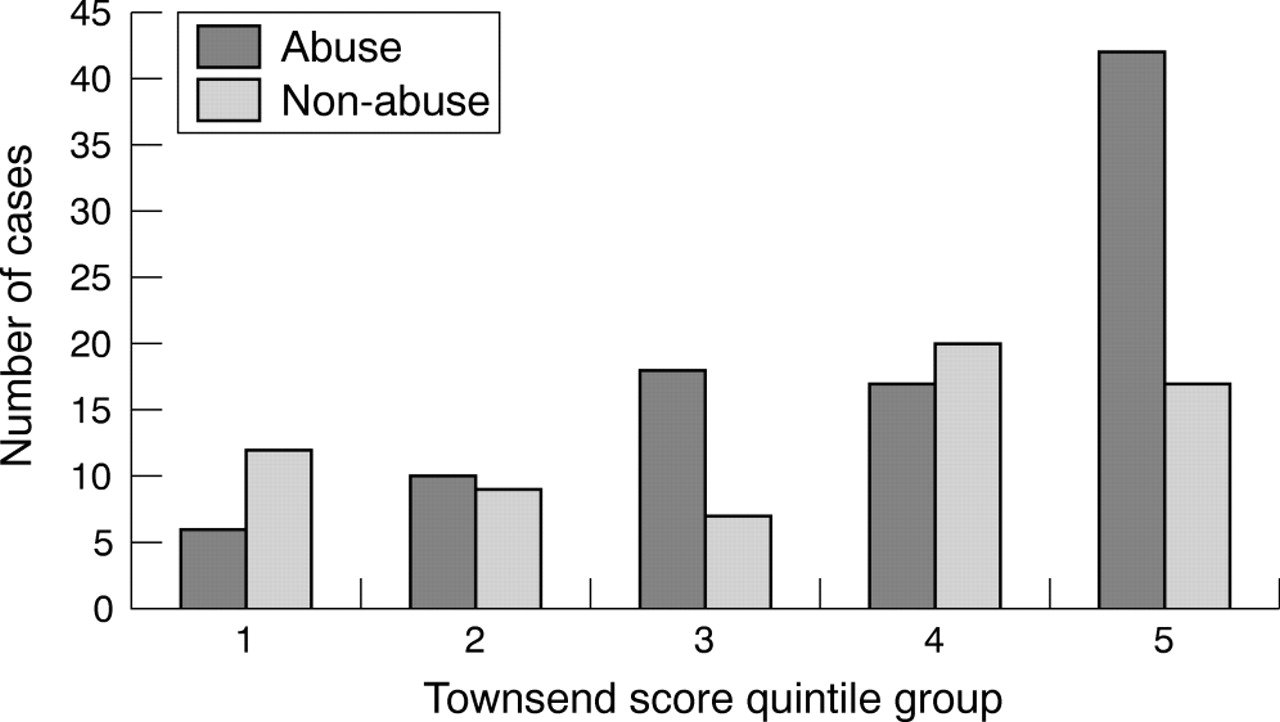
The mean Townsend score for 65/80 non-abuse was 0.3 and for 93/106 NAHI 2.1 (p = 0.007). This indicates that children with NAHI come from a significantly lower socioeconomic group than those with SDH/E from other causes. The distribution by quintile of Townsend scores (158/186) is shown in fig 1⇓.

{kind=link}
Postcode derived Townsend scores for abuse versus non-abuse quintiles (5 = least affluent, 1 = most affluent).
There were 38 families (35 with NAHI) previously known to social services and only six with a child on the child protection register (all NAHI).
DISCUSSION
This is the largest study of SDH/E in infancy in the UK. By including all causes of subdural collections of greater than CSF density including haemorrhage and effusion, the full spectrum of clinical presentation, management, and short term outcome were studied. No attempt was made to separate “haemorrhage” from “effusion”. Accurate definition of the composition of high density intracranial collections by imaging techniques is difficult particularly in chronic cases. It is assumed that as haemorrhage ages it may evolve into effusion. One limitation is that radiological images were not available to the researchers. The data relies on the radiologist’s report and clinician’s interpretations of this.
Reporting by pathologists, neurosurgeons, and paediatricians ensured that cases with varied presentation were included. Occasional fatal cases not reported by clinicians were later identified through the ONS. Once contacted, coroners provided helpful support. It is not possible to be certain how complete ascertainment was. High levels of reporting have been a feature of BPSU studies and by including a range of medical specialists the risk of missing cases was reduced. However, unreturned questionnaires increased doubt about complete ascertainment. We suspect that most represented duplicate notification.
The incidence of SDH/E found in this study (12.54/100 000, 95% CI 10.3 to 14.62, age 0–2 years) is lower than studies1,2 of smaller UK populations. The confidence limits of this study are narrower, however, and there is overlap with these studies. Further there are differences in case definition. In the “Severnside” study1 where neonatal and infection related cases were excluded, the incidence for SDH was 12.8/100 000 aged 0–2 (95% CI 5.4 to 20.2) and 21.0/100 000 (95% CI 7.5 to 34.4) aged 0–1. In the Scottish study2 there were 24.6 cases per 100 000 (95% CI 14.9 to 38.5) aged 0–1 years. However, these authors cited the same figure for incidence of shaken baby impact syndrome and non-accidental head injury, suggesting that they are synonymous.
The varied aetiology of SDH/E is confirmed. The analysis has used clinicians’ opinion regarding this aspect. As the study was retrospective it was inappropriate to apply specific and accepted criteria with which to define non-accidental and accidental injury, the most contentious area of diagnosis. Also there is no absolute or gold standard by which to define NAHI. However, cases of NAHI were more completely investigated and the diagnosis examined in multidisciplinary settings and courts.
The findings confirm that trauma is the commonest cause of SDH/E in infancy. A total of 141/186 infants (75%) suffered trauma, at birth or postnatally following accidental or non-accidental injury. The diagnosis of NAHI was assisted by the additional presence of bruises and fractures without adequate history in 85% of cases. Bruises are unusual in immobile infants before 8–9 months of age13 and fractures and abuse closely associated under a year.14 Outside the neonatal period, retinal haemorrhages are most commonly associated with shaking injury.15,16
What is already known on this topic
Subdural haematoma/effusion (SDH/E) in infancy most often results from non-accidental head injury. Other causes of SDH/E can be diagnosed in many cases from the clinical history, examination, and radiological and laboratory investigation
85% of cases of SDH/E following non-accidental head injury have additional evidence of trauma in the form of bruises and/or fractures
There was little evidence to support the hypothesis that minor trauma is associated with the development of SDH. There were few “accident” cases and in these the history was of more severe or unusual trauma. For example a 17 month old child developed subdural bleeding related to a dissecting aneurysm some time after a head injury when the father fell onto the child.
Non-traumatic causes of SDH/E included cases of bacterial meningitis where occasionally effusions were bloodstained. Cases designated “undetermined” may represent old injury presenting later with chronic SDH/E and a large head. In one infant with SDH at postmortem examination a diagnosis of sudden infant death syndrome seemed inadequate. This study reveals inconsistencies in the investigation of SDH/E. Paradoxically fewer investigations were performed in the undetermined group than in NAHI. This may reflect a reluctance to initiate child protection investigations when SDH/E is an isolated finding in a well child.
Birth trauma was an uncommon cause of SDH/E with significant mortality. Perinatal cases presented shortly after birth. Occasional asymptomatic cases were detected by scanning for other purposes.
Few children showed signs of neglect, but many were failing to thrive. SDH/E from NAHI is over-represented from more deprived postcodes. Townsend deprivation scores are calculated from data on unemployment, household overcrowding, housing tenure, and car ownership using the 1991 UK Census.17 It should be noted that measuring summary characteristics of a population residing in an area, however restricted in size, does not necessarily represent the condition of any single individual.18 However, it has been suggested that census based investigations are a reasonable method of investigating the risk of disease in relation to population characteristics.19 The results are consistent with NAHI occurring in all social classes and with greater frequency in the most deprived group. Reporting bias of NAHI in less socioeconomically privileged groups is described.
Mortality at presentation was 19%, but many survivors are likely to sustain neurodevelopment impairment.20 Short term follow up data has been collected on the cohort and will be presented in a subsequent publication.
The findings reinforce the well known, varied and often subtle symptoms and signs of SDH/E. Boys are more frequently affected. Most cases present before 6 months with frequent delay in diagnosis, which compares with other authors’ experience.8 This reflects the difficulties of contemplating a diagnosis, especially of NAHI. Once considered, SDH/E is easy to detect by neuroimaging. Failure to diagnose may lead to avoidable injury, disability, and death.
What this study adds
The full spectrum of aetiology of SDH/E in the age range 0–2 years includes accidental and non-accidental head injury, perinatal, miscellaneous medical condition, and bacterial meningitis. SDH/E arising from non-accidental head injury occurs to children from all social classes although cases from the least affluent socioeconomic group are over-represented
Cases of SDH/E arising from non-accidental head injury when compared with cases from other causes have poorer weight standard deviation scores
Acknowledgments
We are grateful to the clinicians who contributed cases. We thank Mrs Joyce Robinson for her substantial administrative help and Richard Lynn and Chris Verity of the BPSU for their support. Philip Rees and Roger Parslow assisted with the postcode analysis. Darren Greenwood of the Biostatistics Department, University of Leeds gave invaluable help with statistics.
REFERENCES
Footnotes
Competing interests: none declared