Article Text

Abstract
Aims: To investigate the differences in perception of quality of life between parents of chronically ill children and paediatricians at diagnosis and follow up. Quality of life was assessed using the (HUI3).
Methods: Longitudinal study (July 1999–January 2002) of 37 paediatricians and 181 parents of patients (children aged 1–17 years) with cystic fibrosis admitted for a pneumonia or patients with newly diagnosed acute lymphatic leukaemia, juvenile idiopathic arthritis, or asthma. Main outcome measure was percentage agreement on the attributes of the HUI3 between parents and paediatricians.
Results: Differences in perception of health and wellbeing between paediatricians and parents of children with a chronic disease were found, not only at diagnosis but also after a period of follow up. Differences were particularly clear in the subjective attributes emotion (range of agreement 28–68%) and pain/discomfort (range of agreement 11–33%). In all patient groups, at baseline and follow up, the paediatrician assessed the patient to have less pain/discomfort in comparison to the parents. Despite a prolonged patient- paediatrician relationship, differences at follow up did not decrease compared to baseline.
Conclusion: At the onset of a chronic disease, but also after a period of follow up, quality of life of paediatric patients may be misunderstood by healthcare professionals, especially in the subjective attributes. Systematic assessment of quality of life may contribute to better understanding between physicians and parents.
- ALL, acute lymphoblastic leukaemia
- CF, cystic fibrosis
- CF-adm, children with CF admitted for pneumonia
- HUI3, Health Utilities Index mark 3
- JIA, juvenile chronic arthritis
- QoL, quality of life
- Health Utilities Index
- chronically ill
- longitudinal
- quality of life
Statistics from Altmetric.com
- ALL, acute lymphoblastic leukaemia
- CF, cystic fibrosis
- CF-adm, children with CF admitted for pneumonia
- HUI3, Health Utilities Index mark 3
- JIA, juvenile chronic arthritis
- QoL, quality of life
To monitor the effectiveness of clinical practice and to determine the efficacy of new treatment strategies general indicators of outcome are essential. Physicians predominantly use conventional clinical, laboratory, and radiological measures to assess the success of an intervention and implicitly estimate the wellbeing of the patient. In addition to these measures the importance of quality of life (QoL) assessment is increasingly recognised. In randomised clinical trials QoL is becoming an important secondary outcome.1–5 As improved treatment leads to substantial gains in survival rates (for example, in most cancers and cystic fibrosis), the prevalence of children with a chronic disease is increasing.6 Differences in perception of the wellbeing of patients between patients and their physicians may interfere with the effectiveness of treatment.7 Little is known in the literature about the differences in perception of wellbeing between paediatric patients and physicians. A recent meta-analysis showed that on more objective attributes (sensation, self-care, and mobility) the agreement between parents and physicians was higher than on attributes with a subjective nature (emotion, cognition, and pain/discomfort).8 However, none of the reviewed studies revealed the direction of the differences in perception of QoL between parents and physicians.
The aim of the present longitudinal study was to analyse the differences in perception of QoL between parents of chronically ill children and paediatricians at diagnosis and follow up, and to describe the direction of these differences. QoL was assessed using the Health Utilities Index mark 3 (HUI3). In children under the age of 10 years, parents generally act as a proxy for their child. Children 10 years and older are capable of giving reliable answers about their health status. However, until the age of 17 years, parents still have a crucial role in medical decisions concerning their child. In these decisions, parents rely on their perception of the health status of their child. Therefore, parents were asked to act as a proxy and to assess the QoL of their children. Patients with acute lymphoblastic leukaemia (ALL) were chosen because the HUI has been successfully used in this group.9–11 Patients with juvenile chronic arthritis (JIA), cystic fibrosis (CF), and asthma were included because our hospital aims to be a centre of excellence for these diseases. Furthermore, we expected the attributes of the HUI3 to match well with major complaints of these patients.
We hypothesised that differences in QoL outcomes between parents and paediatricians would be greatest for the subjective attributes. We had no a priori expectations about paediatricians over- or underestimating QoL in comparison with parents of chronically ill children.
METHODS
Patients
Patients were enrolled at four tertiary care centres (Wilhelmina Children’s Hospital, University Medical Centre Utrecht, Utrecht; Sophia Children’s Hospital, Erasmus University Medical Centre, Rotterdam; Emma Children’s Hospital, Academic Medical Centre, Amsterdam; and Asthma Centre Heideheuvel, Hilversum) in the Netherlands during the period July 1999 to January 2002. Eligibility criteria included children admitted with newly diagnosed ALL, children with CF admitted for pneumonia (CF-adm), children with the diagnosis of JIA or asthma and their first visit to the outpatient clinic, aged 1–17 years (patients with asthma, 4–17 years old), and the ability of the parents to understand and read the Dutch language.
Data collection
QoL was assessed using a 42 item interview questionnaire (baseline) and a 15 item self-complete questionnaire (follow up) developed for parents. At baseline parents completed the interview questionnaire administered by the principal investigator (AJJ). The interview was completed during the first week following admission (ALL, CF-adm), or after the first visit to the paediatricians in the outpatient clinic (JIA, asthma). The follow up assessment was completed after induction therapy, before the start of methotrexate according to the SNWLK-ALL-9 protocol (ALL),12 6–8 weeks after admission (CF-adm), three months after the first visit (asthma) or six months after the first visit (JIA) in the outpatient clinic. The follow up interval for each disease was different and determined by the time needed for stabilisation of the initial therapeutic effect according to consensus reached during meetings with clinical experts. In patients with ALL the follow up time was determined by the SNWLK protocol.12 Following the consultation or admission of the patient, the paediatricians completed the Multiattribute Health Status classification System HUI3 (described by Feeny et al).13 The paediatricians completed the HUI3 independently from the parents. Parents and paediatricians were asked to consider the health status of each patient for the preceding period of four weeks.
Information from these questionnaires was converted to health state vectors in the HUI3 formats by an established algorithm.14 The Health Utilities Index mark 2 and mark 3 (HUI2 and HUI3) are generic multiattribute health status classification systems.13 They have been used in a number of clinical studies of children with cancer,15–25 extremely low birth weight infants,26,27 and survivors of paediatric intensive care.28 The HUI3 has been described in detail by Feeny and colleagues.13 Briefly, it consists of eight attributes. Each attribute consists of 5–6 levels representing the range of functioning from normal (1) to severely impaired (5 or 6). The attributes forming the HUI3 system are vision (1–6), hearing (1–6), speech (1–5), ambulation (1–6), dexterity (1–6), emotion (1–5), cognition (1–6), and pain/discomfort (1–5). For example, the attribute emotion represents the following levels: level 1, happy and interested in life; level 2, somewhat happy; level 3, somewhat unhappy; level 4, very unhappy; and level 5, so unhappy that life is not worthwhile.
Consent and ethics approval
Written informed consent was obtained from all parents and of patients over 12 years of age who agreed to participate in the study. The medical ethics committees of all participating centres approved the study protocol.
Statistical analysis
Patients were divided into four groups based on their diagnosis. For each group of patients the following procedure was used.
Absolute differences between physicians and parents for each attribute at baseline and at follow up were calculated using the formula: attribute level physician − attribute level parent. The outcome was dichotomised into presence (“1”) or absence (“0”) of difference between physician and parent. All outcomes zero become “0”, all negative and positive outcomes become “1”. Next, the percentage agreement between pairs of physicians and parents for each attribute were calculated exactly. Subsequently, the proportions of differences between parents and physicians ( = percentage disagreement/100) at baseline (P1) and at follow up (P2) for each attribute were calculated. The differences in proportions at baseline and follow up were given by P1–P2, 95% CI were calculated using the formula P1–P2 ± 1.96* SE [P1–P2].29 95% CIs for differences in proportions that did not include 0 were considered statistically significant. A non-parametric test for paired samples (McNemar test) was used to test the null hypothesis that differences in perception between parents and physicians were the same at baseline and at follow up. Baseline differences in perception for pairs with and without missing data at follow up were tested using a χ2 test (for a two way frequency table). A p value <0.05 was considered statistically significant. The change in the differences (delta) for each attribute was calculated for all pairs by subtracting the absolute differences at follow up from the absolute differences at baseline.
A 10% random sample of all the collected data was taken (SPSS version 10.0), entered twice into the computer by two different persons, and verified (SPSS data entry builder version 1.0). The error rate was acceptable with 0.33%. The SPSS statistical software (version 10.0) was used for all calculations.
RESULTS
Study sample
At baseline the parents of 185 of the 187 eligible children gave consent to participate. Reasons for refusal were the feeling of interference with the disease (JIA, n = 1) and psychological distress when faced with the diagnosis ALL (n = 1). Four other patients were excluded from further analysis because the paediatricians did not return the questionnaire. The final baseline analysis included 181 patients. Complete pairs at follow up were available for 145 of the 181 patients. Reasons for failure to participate at follow up were death (1 patient), no appointment or not showing up at the outpatient clinic (26 patients), and no returned questionnaires (6 patients and 3 physicians). Table 1 shows characteristics of the study group.
Patients’ characteristics
Differences between parents and paediatricians at diagnosis and follow up
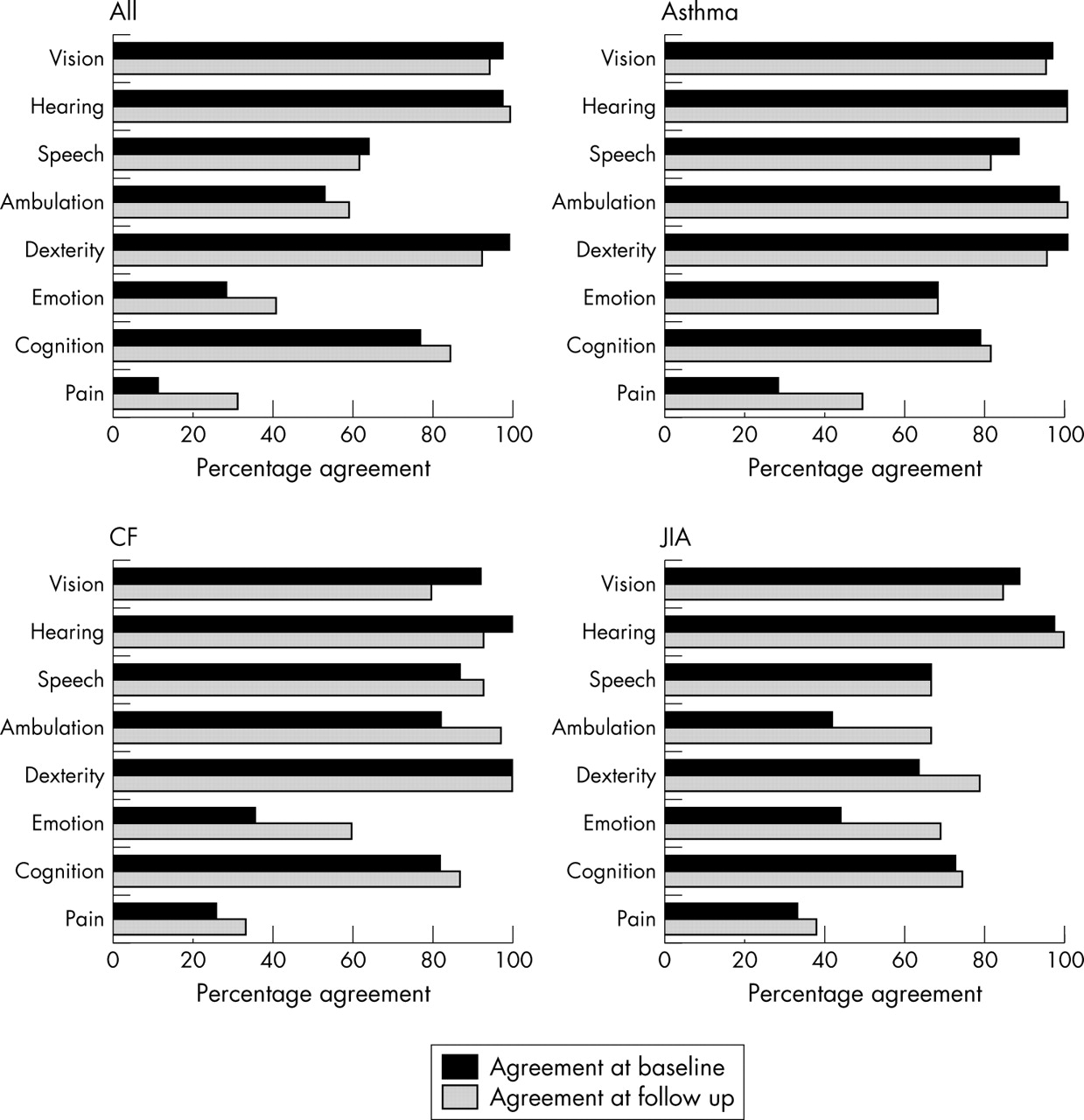
For each group of patients the percentage of pairs with exact agreement between parents and physicians is given in fig 1. For all patient groups the agreement for the attributes vision and hearing were above 90%, in contrast to the agreement for the attributes pain/discomfort and emotion, which were low in all groups. There were no baseline differences for patients without and with missing data. The proportion of differences for the attribute pain/discomfort in patients with asthma and the attributes ambulation and emotion in patients with JIA were significantly lower at follow up than at baseline (table 2). For all other attributes no significant differences were found in the proportion of differences at baseline versus at follow up. Figure 2 shows the direction of the differences in QoL perception between paediatricians and parents. Positive values indicate the paediatrician assessing more impairment than the parents did, and negative values represent the parent assessing more impairment than the paediatrician did. The differences for the attributes vision, hearing, dexterity, and cognition were relatively small and are therefore not shown. For the attribute pain/discomfort the differences were most perspicuous. In all patient groups, at baseline and follow up, the parents assessed the patient to have more pain/discomfort than the paediatricians thought them to have.
Proportion and change of differences at baseline and follow up

Percentage agreement between paediatricians and parents of chronically ill children (ALL, asthma, CF, and JIA) for each HUI3 attribute at baseline and follow up.

{kind=link}
{kind=link}
Number of pairs of disagreement between paediatricians and parents of chronically ill children (ALL, asthma, CF, and JIA) for the HUI3 attributes speech, ambulation, emotion, and pain/discomfort. The HUI3 attribute levels of the parents were subtracted from the levels of the paediatricians. The positive bars represent the number of pairs for each attribute where the paediatrician scored a higher level of impairment within attributes than the parent at baseline (1; black) and at follow up (2; dark grey). The negative bars represent the number of pairs where the parent scored a higher level of disturbances within attributes than the paediatrician at baseline (1; grey) and at follow up (2; white).
DISCUSSION
We have found that differences in the perception of health between parents of children with a chronic disease and their paediatricians exist at diagnosis and after a period of follow up.
In general, the percentage agreement between parents and physicians for each patient group was found to be higher in the objective than in the subjective health attributes. Our earlier findings from the literature showed a pooled percentage agreement of 84–89% for the objective attributes and of 69–77% for the subjective domains.8 In the present study the agreement for the attribute pain/discomfort was remarkably low for all patient groups. For the attribute emotion, the agreement was lower than expected from the literature.8 Probably, in our study the agreement for these attributes was low because most patients consulted the physician in the acute phase of the disease, whereas in the literature the HUI has been used mostly in survivors of childhood cancer.15–20,23–25 It is known from the literature that QoL of patients can change dramatically during treatment. For example, the QoL of children with recurrent acute otitis media and/or chronic otitis media with effusion significantly improved after surgical intervention,30 whereas the QoL of children with chronic viral hepatitis temporarily deteriorated during alpha-interferon therapy.31 Also, differences in perception of QoL between parents and physicians and the magnitude of these differences are likely to be susceptible to change in time. In a study of adults with cancer it was found that the agreement for the more private domains (such as feelings, social functioning, overall QoL, and pain/discomfort) was slightly higher at follow up than at baseline. Firstly, it is suggested that monitoring the patients’ QoL over time may increase the caregivers’ awareness of wellbeing of the patient.32 Secondly, the objective domains are visible and more concrete than the subjective domains. Therefore, a higher agreement can be expected in the former.33 However, in our study the agreement did not essentially change over follow up periods, although patients were treated for their acute symptoms and patients and physicians became acquainted to each other. At follow up the rates of (dis)agreement remained fairly stable. Only for patients with asthma (pain/discomfort) and for patients with JIA (ambulation and emotion) did the agreement improve at follow up. We found obvious differences in four of the eight attributes. Paediatricians rated more emotional problems (ALL, CF, JIA) and problems with ambulation (JIA). Parents rated more pain/discomfort (all patient groups) and speech impairments. In our study we did not use the children’s’ assessment of their quality of life. However, for the attribute pain/discomfort it is known from the literature that physicians have the tendency to underestimate the intensity of the patient’s pain/discomfort.32,34–36 A possible explanation for the disagreement on speech impairment is that in young children paediatricians tend to interpret HUI level 1 as language development according to age, while parents scored level 3 as development according to age.
Before further interpretation of our results, some methodological issues need to be addressed. A strong feature of our study is that the participation rate was high and that it had very few missing data at baseline. Furthermore, we used a validated instrument to measure quality of life as judged by both physicians and the parents. Physicians completed the assessments independent from parental HUI measurements. Some other points need attention. Complete follow up data were available for 80% of the patients. Because the differences in perception of QoL at baseline were the same for patients with and without complete follow up data, we expect our results to be valid. Each paediatrician (n = 37) completed the HUI several times (range 1–34). In 90 patients the same paediatricians completed the assessment both at baseline and at follow up. Due to a learning effect of the paediatrician the percentage agreement in this study might be higher than would have been found in regular clinical practice. The HUI has been validated originally for children of 6 years and older.13 For young children only a few QoL questionnaires are available (Functional Status, RAND, and the TAPQOL).37–39 In a study assessing the health status in a heterogeneous population of children admitted to intensive care, it seemed feasible to classify children over 1 year of age reliably, using the HUI by an observer well known to the patient.40 In our study the HUI3 questionnaire was administered to the parents by an interviewer at baseline and was self-completed at follow up while the HUI3 was self-completed by the paediatricians (both assessments). In the literature different results are reported about the effect of the mode of administration of HRQoL questionnaires. Grootendorst et al found that subjects participating in the Ontario Health Study, completing the interviewer administered form, reported less dysfunction than subjects completing the self-reported form.41 However Verrips et al reported that the mean number of affected attributes was higher and the mean utility score was lower when children (preterm born infants now 14 years old) and proxies were interviewed than when they self-completed the questionnaire.27 Both studies used the HUI3 to assess the health status. In our study the participating paediatricians preferred the self-completed form because of their time schedule at the outpatient clinic.
With regard to the implications of our study, we conclude that QoL should be given a fair amount of attention in chronic paediatric illnesses. Good medical practice requires an optimal relationship between physicians, patients, and parents for mutual understanding of the impact of the disease. Whatever the reasons for discrepancies of perception, physicians should be aware that parents and physicians may look differently at the impact of the disease. This is particularly important for discrepancies pertaining to the attributes emotion and pain, which are vital to the child’s wellbeing. Physicians have the tools to improve on this, by better and more explicitly discussing these issues with patients and parents. As differences in perception of QoL between parents and physicians may be different for various countries/populations, replication studies are needed. QoL evaluation may have a prominent role in assessing the changes of a patient’s condition in the natural course of the disease or in the follow up of therapeutic interventions. In this way, better mutual understanding of perception of QoL between physician and the parents of the patient may enhance effects of treatment.
What is already known on this topic
-
Little is known in the literature about the differences in perception of quality of life between patients and physicians
-
Objective attributes of health had a higher agreement between parents and physicians than the more subjective attributes
-
The magnitude of the difference in perception of quality of life between parents and physicians is unknown
What this study adds
-
Clear differences in perception of health and wellbeing between parents of children with a chronic disease and physicians were found
-
In all patient groups, the physicians assessed the patient to have less pain/discomfort than the parents thought
-
Quality of life may contribute to better understanding between physicians and parents
Acknowledgments
We are grateful to all parents of the patients and all clinicians of the participating centres for their efforts of taking part in this study.
Special thanks are extended to E Visser and I van der Vaart, research nurses Sophia Children’s Hospital, for their practical help, and to C Tims for her assistance with the data management.
REFERENCES
Footnotes
-
Role of the funding source: the sponsors of this study had no role in study design, data collection, data analysis, data interpretation, or writing of the report
-
Competing interests: none declared
Linked Articles
- Atoms