Article Text

Abstract
Aims: To investigate the correlation of pH, partial pressure of oxygen (PO2), partial pressure of carbon dioxide (PCO2), base excess (BE), and bicarbonate (HCO3) between arterial (ABG), venous (VBG), and capillary (CBG) blood gases.
Methods: Patients admitted to the paediatric intensive care unit (PICU) in Çukurova University between August 2000 and February 2002 were enrolled.
Results: A total of 116 simultaneous venous, arterial, and capillary blood samples were obtained from 116 patients (mean age 56.91 months, range 15 days to 160 months). Eight (7%) were neonates. Sixty six (57%) were males. pH, PCO2, BE, and HCO3 were all significantly correlated in ABG, VBG, and CBG. Correlation in PO2 was also significant, but less so. Correlation between pH, PCO2, PO2, BE, and HCO3 was similar in the presence of hypothermia, hyperthermia, and prolonged capillary refilling time. In hypotension, correlation in PO2 between VBG and CBG was similar but disappeared in ABG–VBG and ABG–CBG.
Conclusions: There is a significant correlation in pH, PCO2, PO2, BE, and HCO3 among ABG, VBG, and CBG values, except for a poor correlation in PO2 in the presence of hypotension. Capillary and venous blood gas measurements may be useful alternatives to arterial samples for patients who do not require regular continuous blood pressure recordings and close monitoring of PaO2. We do not recommend CBG and VBG for determining PO2 of ABG.
- arterial
- venous
- capillary
- blood gases
- correlation
- ABG, arterial blood gases
- BE, base excess
- CBG, capillary blood gases
- PCO2, partial pressure of carbon dioxide
- PICU, paediatric intensive care unit
- PO2, partial pressure of oxygen
- RDS, respiratory distress syndrome
- VBG, venous blood gases
Statistics from Altmetric.com
- ABG, arterial blood gases
- BE, base excess
- CBG, capillary blood gases
- PCO2, partial pressure of carbon dioxide
- PICU, paediatric intensive care unit
- PO2, partial pressure of oxygen
- RDS, respiratory distress syndrome
- VBG, venous blood gases
Arterial blood gas (ABG) sampling represents the gold standard method for acquiring patients’ acid-base status. The most common complications associated with arterial puncture are pain, arterial injury, thrombosis with distal ischaemia, haemorrhage, and aneurism formation.1 The risks increase with repeated arterial punctures, especially in children with small arteries and with insertion of a catheter when performed by inexperienced individuals. Capillary (CBG) and venous (VBG) blood gas samplings may be useful alternatives to arterial blood gas sampling. Capillary and venous blood gas samplings are easier to obtain and a less invasive way of evaluating acid-base status in the paediatric intensive care unit (PICU). Both avoid the risks of arterial punctures. Several studies have shown good correlation between capillary blood, venous blood, and arterial blood gas values.2–4 Escalante-Kanashiro and Tantalean-Da-Fieno showed that capillary blood gases were a useful alternative to gasometric evaluation of critically ill children, even in the presence of hypothermia or hypoperfusion.2 Gennis and colleagues showed a high correlation for pH, partial pressure of carbon dioxide (PCO2), and bicarbonate (HCO3), but the accuracy of predicting arterial values from venous values was limited.3 In another study, Harrison et al documented that capillary blood gases accurately reflected arterial pH and PCO2 in most of the PICU patients.4
The purpose of this study was to investigate the correlation between simultaneous ABG, VBG, and CBG values, to determine the correlation between patients with diverse pathological conditions, and to establish whether capillary or venous blood gases could correlate and replace arterial blood gases in the PICU.
METHODS
Patients admitted to the PICU at Çukurova University between August 2000 and February 2002 were enrolled in the study. Blood gases were obtained if the patient needed blood gases for clinical decisions. Heart rate, respiratory rate, temperature, arterial blood pressure, oxygen saturation by pulse oxymeter, and capillary refill time were recorded simultaneously with each sample.
Arterial and venous samples
If the patient had a central venous or arterial line, they were used for blood sampling. After withdrawing 5 ml of blood from the lines with a non-heparinised syringe, 1 ml of arterial/venous blood was obtained with another similar syringe and transferred, as soon as possible, to a heparinised 0.75 ml capillary tube. Arterial and venous blood samples of the neonates were all obtained from umbilical catheters. If the patient did not have a central venous or arterial line, arterial and venous blood vessels were punctured with a needle after aseptic cleaning, and blood gases were obtained directly into an identical capillary tube.
Capillary samples
Capillary blood gases were obtained without warming the extremity. The heel in newborns/infants and ring finger in children were punctured to obtain the samples. After aseptic cleaning the lateral distal portion of the heel/finger was punctured with a lancet and blood gases samples were obtained by “contact” with the capillary tube’s tip. Two sides of the tube were closed by fingers to avoid air bubbles. All samples were obtained by the investigators. Samples were analysed in a blood gas analyser located in the PICU (AVL-Omni, Switzerland) within five minutes of extraction. pH, partial pressure of oxygen (PO2), partial pressure of carbon dioxide (PCO2), base excess (BE), and bicarbonate (HCO3) values were recorded.
Capillary refill status was used as a criterion for peripheral perfusion. It was considered normal if it was <3 seconds.5 Blood pressure was determined with a sphygmomanometer. Hypertension was diagnosed if the systolic blood pressure was above the 90th centile of the normal for age.6 Hypotension was defined as two standard deviations below the age appropriate mean.7 Hypothermia was diagnosed if axillary temperature was <36°C and hyperthermia when axillary temperature was >38°C.
Statistical methods
SPSS.10.1 for Windows was used for statistical analysis. Pearson correlation coefficients were determined for correlation and regression analysis was performed for arterial values on venous and capillary variables. For all analyses, p<0.05 was considered statistically significant.
The protocol was reviewed and approved by the local ethics committee of the Faculty of Medicine.
RESULTS
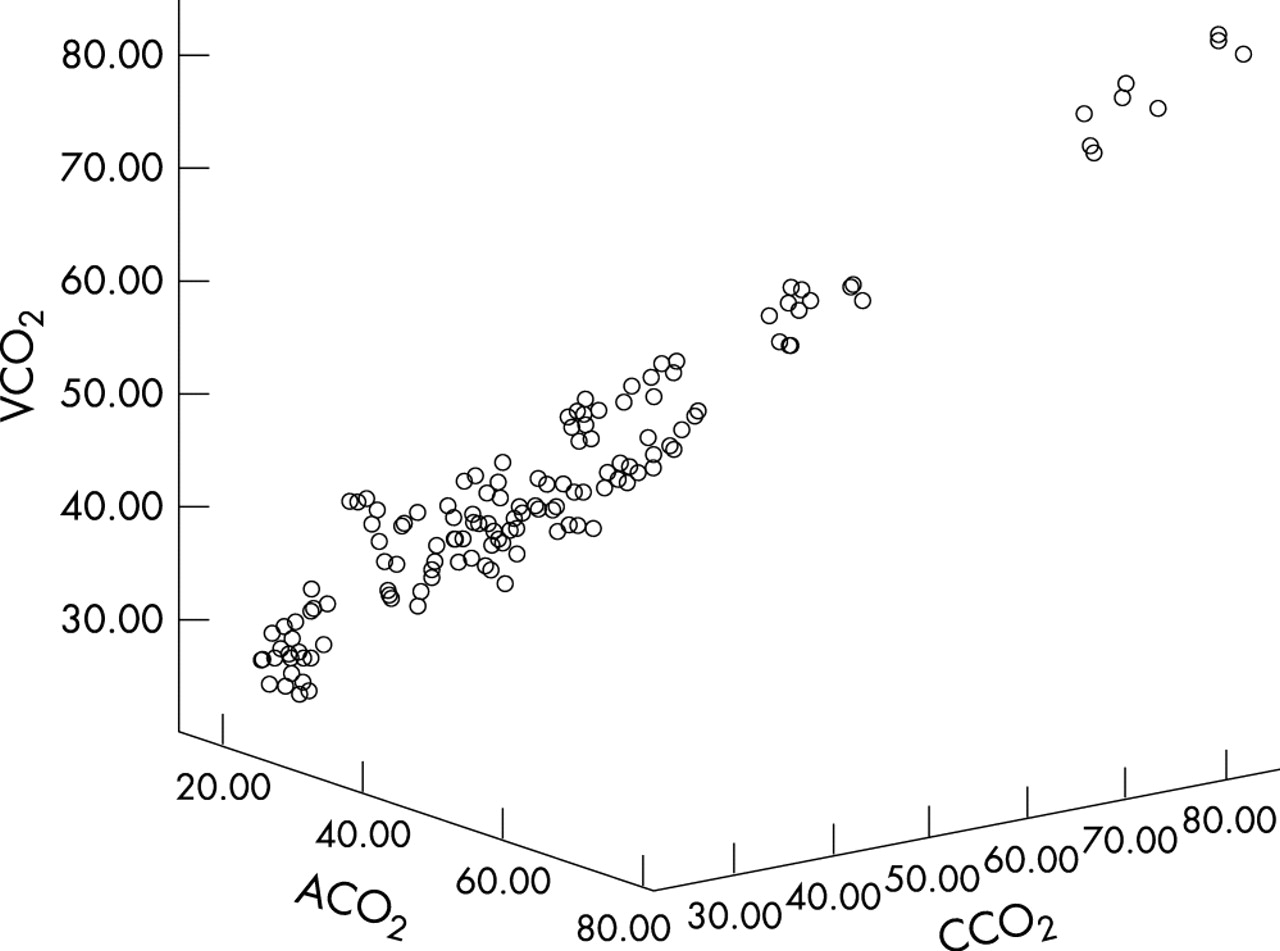
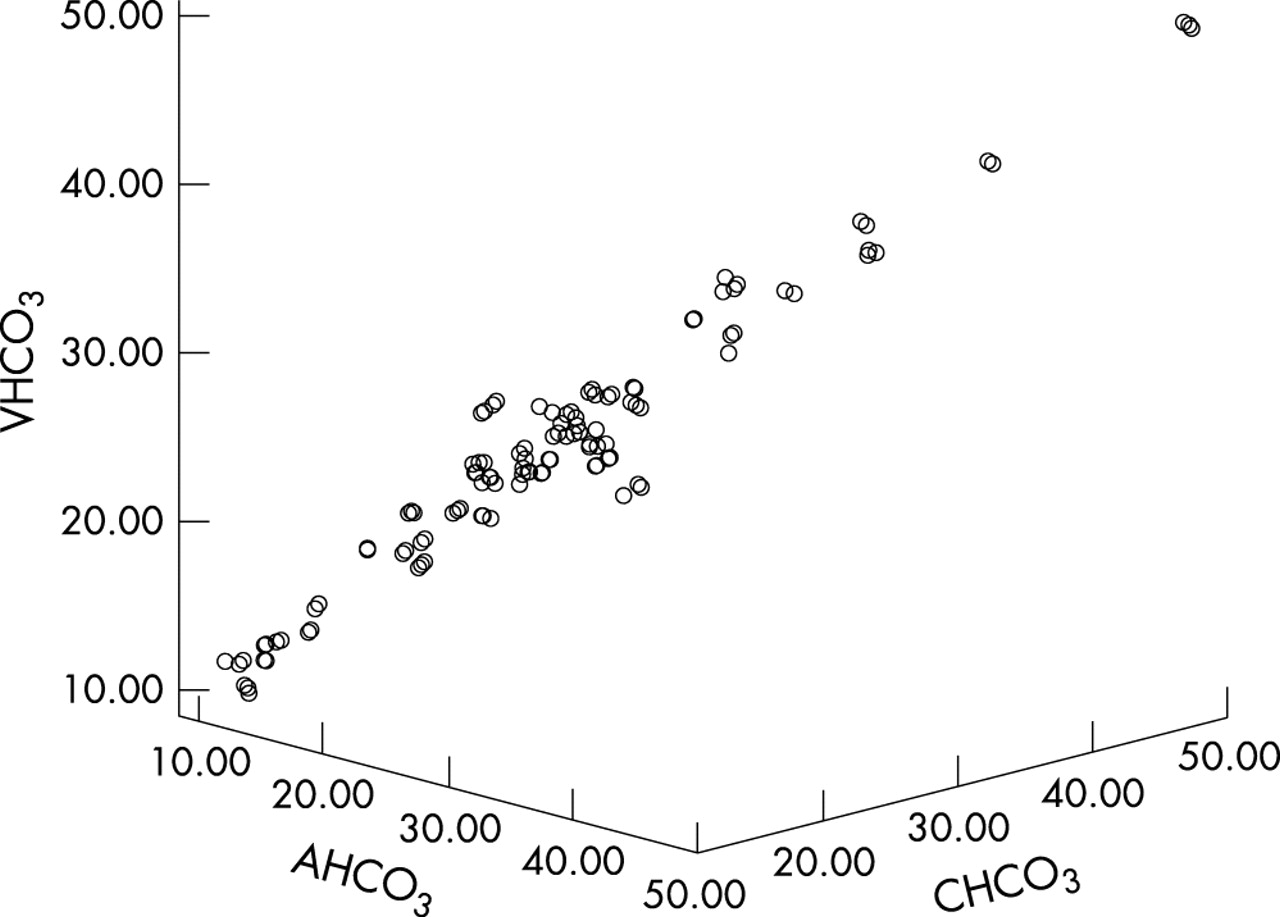
A total of 116 simultaneous venous, arterial, and capillary blood gases were obtained from 116 patients. Admission diagnoses included pneumonia, sepsis, encephalitis, congenital heart disease, respiratory distress syndrome (RDS), burn, intoxication, status epilepticus, severe dehydration, bronchiolitis, croup, metabolic encephalopathy, diabetic ketoacidosis, hepatic coma, cystic fibrosis, meningitis, Guillain-Barré syndrome, and others (table 1). The mean age of the patients was 56.91 (SD 49.09) months (range 15 days to 160 months); eight (7%) were neonates. Sixty six (57%) were males and 50 (43%) were females. Table 2 shows characteristics of the patients. Thirty (28%) of the patients were intubated and samples were obtained while the subjects were receiving FiO2 >0.21 torr. pH, PCO2, BE, and HCO3 were all significantly correlated in ABG, VBG, and CBG (tables 3–4, figs 1–4). Table 5 shows the correlation in hypotensive agents. The correlation for PO2 was also significant, but less strongly so (table 3, fig 5). The correlation for pH, PCO2, BE, and HCO3 was similar in the presence of hypothermia, hyperthermia, and prolonged capillary refilling time, but in hypotension there was a weak correlation for PO2 between only VBG and CBG (r = 0,49, p<0.001); the weak correlation between ABG–VBG and ABG–CBG disappeared (table 5, fig 6).
Clinical diagnoses of the patients
Characteristics of the patients
Correlation of arterial, venous, and capillary blood gases for pH, PO2, PCO2, BE, and HCO3 in PICU patients
Regression of arterial blood gas values on venous and capillary blood gas values
Correlation of arterial, venous, and capillary blood gases for PO2 in hypotensive patients

Correlation of arterial, venous, and capillary blood gases for pH.

Correlation of arterial, venous, and capillary blood gases for PCO2.

Correlation of arterial, venous, and capillary blood gases for BE.

Correlation of arterial, venous, and capillary blood gases for HCO3.

Correlation of arterial, venous, and capillary blood gases for PO2.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation of arterial, venous, and capillary blood gases for PO2 in the presence of hypotension.
DISCUSSION
Acid-base analysis is an essential method in PICU, yielding valuable information about a variety of disease processes.1,3,5 Non-invasive methods, such as pulse oximetry, transcutaneous monitoring of oxygen and CO2, and end tidal CO2 have been proven to be useful,1 but they do not give information about pH, PO2, and bicarbonate. Arterial blood gases are frequently determined in the PICU. This is, however, an invasive way of monitoring blood gas and there are complications, mostly local haematomas related to arterial puncture. The procedure itself is technically difficult and painful in children. Arterial lines are usually placed in unstable patients in the PICU who need close monitoring of PO2. When an arterial line is not in place, CBG or VBG values continue to be obtained and used for clinical monitoring and management decisions.
Capillary gas sampling is a less invasive way of evaluating acid-base status in a well perfused patient. Most patients need a venous puncture for other laboratory work, and a VBG sample can be obtained at the same time. If a blood gas value determined by venous or capillary samples could be used to show patients’ acid-base status and guide their management with the same accuracy as arterial sampling, this would be preferable because of ease of blood sample collection. For many years, clinicians have been looking for alternatives to ABG sampling in both children and adults, and studies have investigated ABG, VBG, and CBG samples and the correlation between the values.8–17
Studies comparing ABG and CBG, ABG and VBG samples in diabetic ketoacidosis, and ABG–CBG blood gases values in stable PICU patients have shown good correlation among ABG, VBG, and CBG samples.4,9,11,12 However, there have been no studies comparing a large number of simultaneously obtained ABG, VBG, and CBG samplings in stable and unstable PICU patients. We studied 116 simultaneously obtained ABG, VBG, and CBG of 116 PICU patients and showed pH, PCO2, BE, HCO3 were all correlated in arterial, venous, and capillary blood gases in normotensive, hypertensive, hyperthermic, and hypothermic patients as well as in the patients with normal or prolonged capillary refilling time. Although there was a significant correlation for PO2 in these patients, it was lower. Similar to our findings, McLain et al, in preterm infants, found good correlations for pH and PCO2 in CBG and ABG, but unsatisfactory correlation for PO2.13 Gandy et al compared ABG and CBG of 66 healthy and 40 sick children and found good correlation for pH and PCO2 in healthy children older than 3 hours old, but poor correlation in sick subjects.9 On the other hand, Thomsen studied pH and pCO2 in infants and Courtney et al studied pH, PCO2, and PO2 in CBG and ABG in neonates; they found no correlation for pH, PCO2, and PO2.8,10
A large group of children who are mildly to moderately ill can benefit from acid-base status determination for assisting in diagnosis, management and progression of illness such as renal disorders and dehydration, diabetic ketoacidosis, altered level of consciousness, intoxications and metabolic disorders. In these situations ABGs are not really needed, VBG or CBG samples may be satisfactory. McGillivray et al studied 78 CBG and VBG in acute ill, well-perfused patients. There was excellent correlation between values obtained from venous and capillary sources and they concluded that venous gas value provided acceptable means for assessing severity of illness and response to treatment in well-perfused patients.14
Most of the studies comparing various blood gases have been done mainly in stable patients. Some articles showed poor correlation when hypothermia, hypoperfusion, or shock were present.9,15 However, patients with these kinds of conditions are those who need more frequent evaluation of their pH, PCO2, PO2, BE, and HCO3. There have been two recent reports about the correlation among ABG, VBG, and CBG blood gas values of PICU patients.2,4 Harrison et al showed that capillary gas values accurately reflected arterial pH and PCO2, and capillary samples did not significantly underestimate arterial hypercarbia or acidosis in most of the PICU patients.4 Escalante-Kanashiro and Tantalean-Da-Fieno showed good correlation between CBG and ABG, even in the presence of hypothermia and hypoperfusion.2 Similarly, in the present study we showed that neither temperature nor peripheral perfusion altered the correlation of pH, PO2, PCO2, BE, and HCO3. In the presence of hypotension, however, the weak correlation in PO2 between ABG–VBG and ABG–CBG disappeared, while correlation between VBG–CBG was similar. Perfusive conductance of oxygen, diffusion of oxygen from capillary to mitochondria, and blood flow distribution are the major determinants of oxygen uptake at the tissue level. Besides these, red blood cell transit time is another factor which can determine the diffusion of oxygen to tissues.18 In hypotensive patients, because of the possible changes in blood flow distribution (heterogeneous distribution of blood flow) as well as possible increased transit time of red blood cells, capillary and venous PO2 values may be similar. This may explain the non-significant relation between arteriolar PO2 values and venous and capillary PO2 values.
We did not warm the extremity before obtaining the sample. It is not reliable to control the degree of warming from patient to patient, and it is not practical to warm the extremity in intensive care units.
In summary, we have shown a good correlation in pH, PCO2, PO2, BE, and HCO3 among ABG, VBG, and CBG values, but in the presence of hypotension there was only a weak correlation in PO2 values between VBG and CBG. Capillary and venous blood gas measurements may be useful alternatives to ABG samples for patients who do not require regular continuous blood pressure measurements and close monitoring of PaO2 measurements. We do not recommend CBG and VBG for determining PO2 of ABG. Further studies with a greater number of unstable patients may extend the use of capillary and venous gases to arterial blood samples.
Acknowledgments
The authors would like to thank Sadi Kurdak for his invaluable assistance in discussion.