Article Text

Abstract
Background: Previous studies have presented conflicting results regarding the predictive effect of various clinical symptoms, signs, and plain imaging for intracranial pathology in children with minor head injury.
Aims: To perform a meta-analysis of the literature in order to assess the significance of these factors and intracranial haemorrhage (ICH) in the paediatric population.
Methods: The literature was searched using Medline, Embase, Experts, and the grey literature. Reference lists of major guidelines were crosschecked. Control or nested case-control studies of children with head injury who had skull radiography, recording of common symptoms and signs, and head computed tomography (CT) were selected. Outcome variable: CT presence or absence of ICH.
Results: Sixteen papers were identified as satisfying criteria for inclusion in the meta-analysis, although not every paper contained data on every correlate. Available evidence gave pooled patient numbers from 1136 to 22 420. Skull fracture gave a relative risk ratio of 6.13 (95% CI 3.35 to 11.2), headache 1.02 (95% CI 0.62 to 1.69), vomiting 0.88 (95% CI 0.67 to 1.15), focal neurology 9.43 (2.89 to 30.8), seizures 2.82 (95% CI 0.89 to 9.00), LOC 2.23 (95% CI 1.20 to 4.16), and Glasgow Coma Scale (GCS) <15 of 5.51 (95% CI 1.59 to 19.0).
Conclusions: There was a statistically significant correlation between intracranial haemorrhage and skull fracture, focal neurology, loss of consciousness, and GCS abnormality. Headache and vomiting were not found to be predictive and there was great variability in the predictive ability of seizures. More information is required about the current predictor variables so that more refined guidelines can be developed. Further research is currently underway by three large study groups.
- CT, computed tomography
- GCS, Glasgow Coma Scale
- ICH, intracranial haemorrhage
- craniocerebral trauma
- head injury
- brain injury
- meta-analysis
Statistics from Altmetric.com
Despite the fact that we are now approaching the 30th anniversary of the publication of the Glasgow Coma Scale (GCS),1 there is still controversy regarding the categorisation of minor traumatic brain injury in children. In the UK there are 1 million head injuries per year,2 and 50% of these are children.3 Among the children with a minor head injury the challenge is to identify those who are at low risk of intracranial complications and safely discharge them. The remainder would form the high risk group requiring combinations of imaging and admission. In the UK the admission rate for minor head injury currently varies between 10% and 20%.4–6 However of those admitted, the risk of intracranial complications is still very low: between 1% and 3%.6–8 Therefore our selection of these children turns out to be incorrect in 97% of cases.
The situation is similar in the USA where only around 3% of children admitted after computed tomography (CT) scanning for traumatic brain injury go on to require a neurosurgical intervention.9 The American Academy of Pediatrics recently performed a systematic review in order to address this issue,10 but concluded that the current literature was unable to assist them in making tighter recommendations for either admission or computed tomography.
However, the research base is shortly set to increase substantially, with the Children’s Canadian Head CT rule (CATCH study),11 the International Study on Head Injury at Pediatric age (ISHIP study),12 and our own multicentre observational cohort study of 21 000 head injured children in the UK. Therefore, prior to the publication of these large studies we felt that it was important to summarise the current evidence in the field of children’s minor head injury, by meta-analysis, in order to highlight areas of uncertainty and controversy.
METHODS
Criteria for selecting studies
A full systematic review of the literature was conducted in order to identify suitable papers for meta-analysis. Cohort or nested cohort studies that presented data on childhood minor head injuries in terms of the presence or absence of intracranial haemorrhage were considered. Papers containing adults and children were included where the child specific data could be extracted. Papers were judged to be of adequate quality if they presented a series of patients greater than 100 in number, either retrospectively or prospectively, and documented a reliable gold standard for the detection of intracranial haemorrhage in all patients in the study. A combination of CT and follow up was deemed to be an acceptable gold standard, but papers reporting only operated haematomas were not accepted unless CT was also performed. Intracranial haemorrhage was defined as any intracranial abnormality detected on CT scanning due to the traumatic presence of extravascular blood. Although we defined a minor head injury as a patient with a GCS of 13–15, papers that included all severities of head injury were included; their range of severity is documented in table 1. Consecutive cohorts were accepted, but non-consecutive cohorts were only accepted for this meta-analysis if they used consistently applied reference standards.
Childhood head injury papers that predict intracranial haemorrhage
Seven clinical correlates were deemed suitable for data extraction (see table 2). Many other clinical correlates were considered for data extraction, but data were not presented with adequate consistency to justify extraction from the original papers.
Results of meta-analysis
Search strategy
Medline and Embase were searched from January 1990 to June 2002. Our expert panel agreed that prior to 1990 there would be very few well conducted studies with a high CT scan rate that would usefully contribute to our study and any that existed would be picked up using our other search strategies. Non-English papers were translated if abstracts were deemed to be of interest. Search terms were constructed to find all papers with data on intracranial complications after head injury. No age limits were used in the initial searching, although for data extraction a child was defined as any person less than 18 years of age. The grey literature was searched at the British Library and experts were contacted for additional papers. The reference lists of guidelines developed by the American Academy of Pediatrics, the Eastern Association for the Surgery of Trauma, the Scottish Intercollegiate Guidelines Network, and the Royal College of Surgeons of England were also searched.10,13–15 experts were contacted and asked whether they knew of additional papers of relevance that were not found in our search. The expert group consisted of the National Institute of Clinical Excellence (NICE) Working Group for Head Injuries, the members of which represent every stakeholder organisation in the development of guidelines for head injury in the United Kingdom.
Statistical methods
A pooled estimate of the common relative risk ratio was performed, using a random effects model as described by DerSimonian and Laird, with confidence intervals calculated using the Woolf method. Homogeneity was established using the Breslow-Day test.16 Of note, for good inter-study agreement, we required the Breslow-Day statistic to have a p value >0.1 rather than >0.05, as it is generally acknowledged these tests provide conservative estimates of heterogeneity.18 The analysis was performed using STATA version 7.0 (STATA, Stata Corporation, Texas, USA)
RESULTS
The abstracts of 1454 Medline and 680 Embase papers were identified. These abstracts were assessed by two independent reviewers who reduced the number to 98 for full paper review. During the full review process each paper was graded according to the level of evidence that it provided. Level 1 evidence was defined as a consecutive cohort study with good reference standards that validated a decision rule. Level 2 evidence was defined as a consecutive cohort study with good reference standards. Level 3 was defined as a non-consecutive study or without consistently applied reference standards. Level 4 was defined as case-control study or non-consecutive study with poor or non-independent reference standards (and thereby excluded from our analysis) These grades are consistent with those used by the Oxford Centre for Evidence-based Medicine and the National Institute for Clinical Excellence in the UK for areas of research where prospective randomised controlled trials are not possible.
Thirty four papers were deemed to be of adequate quality for inclusion but many did not publish data that could be used for meta-analysis. The reason for this in many cases was the lack of ability to break down the data presented into child and adult groups.19–29 In addition some papers did not present enough data on individual clinical correlates for inclusion,30–33 and some were consecutive studies but in cohorts too small for inclusion.34–36
Nineteen papers provided data for children after minor traumatic brain injury.6,9,37–50 Three of these papers were rejected either due to the lack of CT scanning to diagnose ICH (both were written in the 70s)51,52 or due to poor quality.53
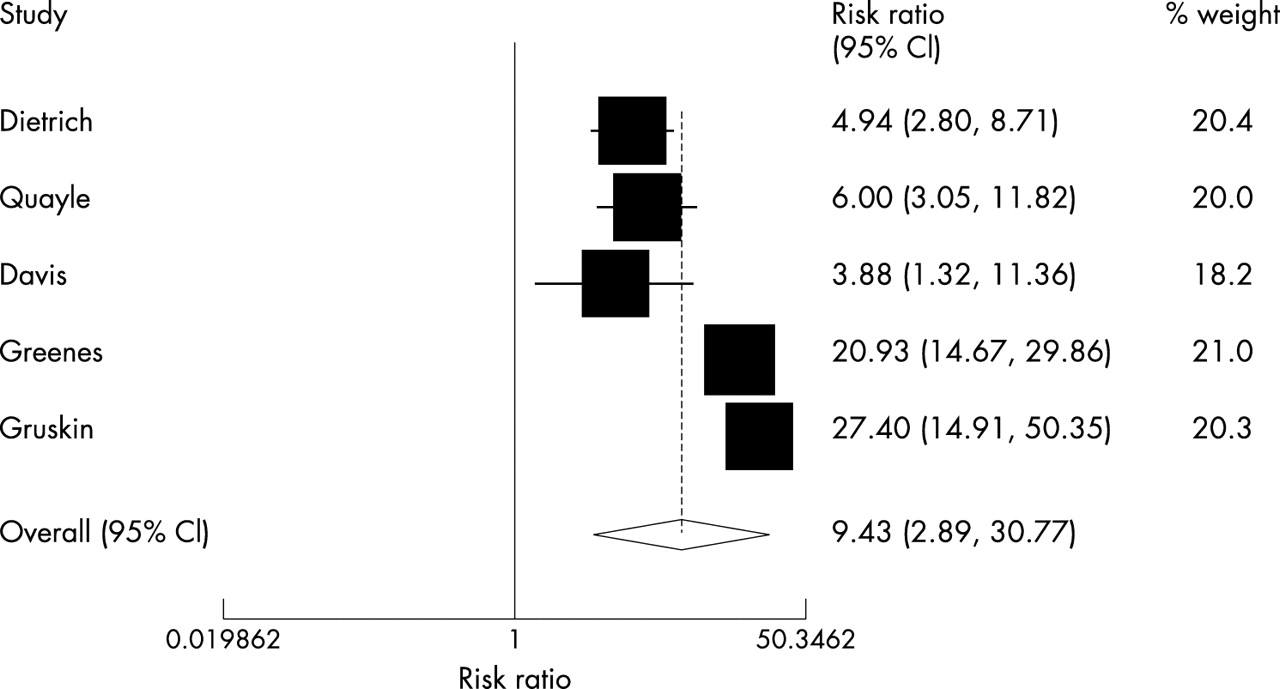
The 16 papers finally selected for inclusion contained a total of 22 420 patients and are summarised in table 1; the full results of the meta-analysis are shown in table 2. The results show a significantly increased relative risk of intracranial haemorrhage for reduced conscious level (5.51), focal neurology (9.43), skull fracture (6.13), and loss of consciousness (2.23). Vomiting did not significantly increase the relative risk of an intracranial haematoma in pooled results from 14 092 children and seven studies, even though these studies showed good homogeneity. Headache, after meta-analysis of 1136 patients from four studies showed no significant increase of risk, even though there was also good agreement among these studies. More surprisingly seizure, although giving a common relative risk estimate of 2.82 from 14 092 patients across seven papers did not reach significance. This must be read with caution as there was considerable heterogeneity in this group. In addition all the factors that did show a significantly increased risk for intracranial haemorrhage, also showed a considerable inter-study heterogeneity. This heterogeneity is most clearly seen in the Forest plots for each variable (figs 1–7).
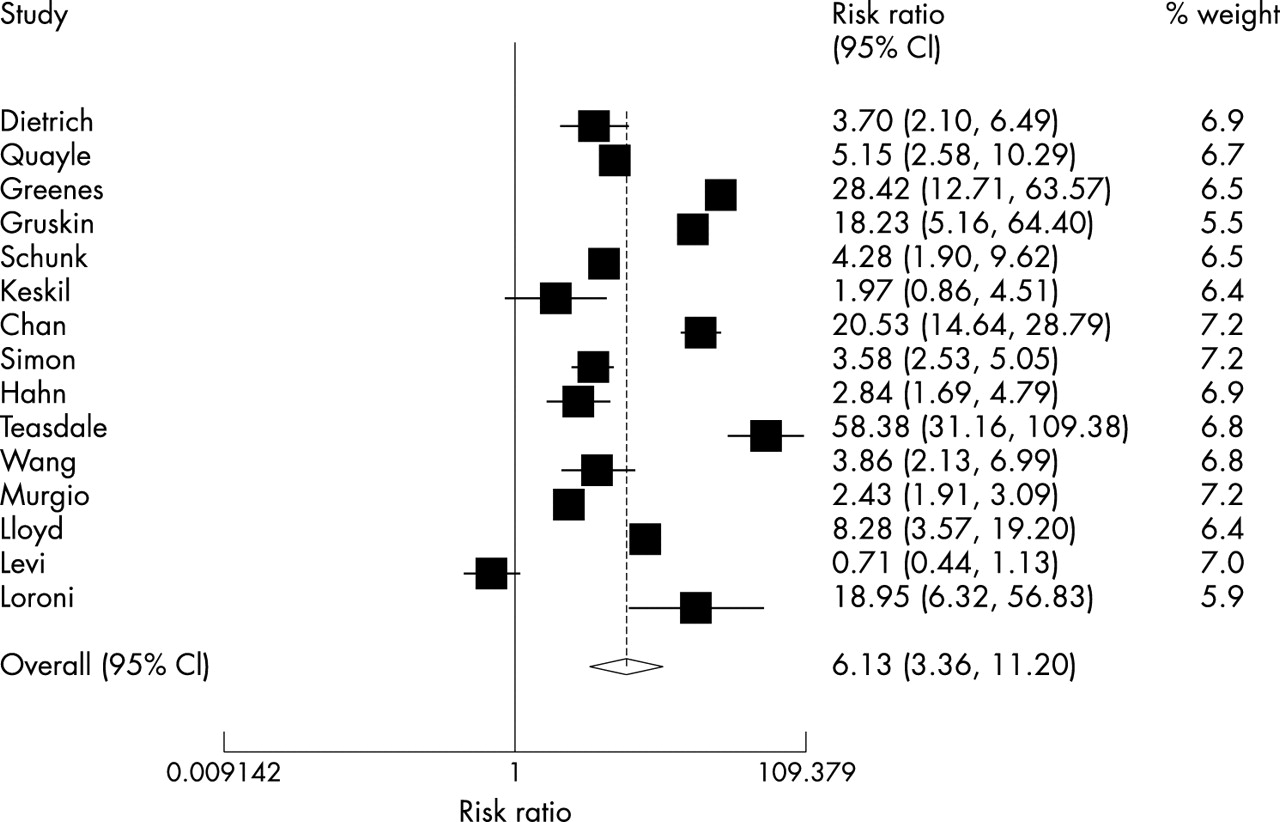
Forest plot of ICH versus skull fracture.

Forest plot of ICH versus headache.

Forest plot of ICH versus vomiting.

Forest plot of ICH versus focal neurology.

Forest plot of ICH versus seizures.

Forest plot of ICH versus LOC.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of ICH versus reduced GCS.
DISCUSSION
The DerSimonian-Laird (D–L) random effects model was used to generate a common relative risk ratio, in preference to a fixed effect model such as the Mantel-Haenszel method. The random effects model was chosen as it was clear that patient inclusion criteria varied across studies and therefore a similar background population of patients for each study could not be assumed.54,55
A large amount of heterogeneity was found between the studies. The reason for this is perhaps most clearly shown by looking at the prevalence of intracranial haemorrhage. This varied from 1.3% to 36% among the 16 studies (see table 1). The variation in the ICH prevalence rates is mainly explained by the variability in the inclusion criteria. Those studies that had low prevalence rates studied every patient that was treated for head injury attending the emergency department, whereas the studies with high prevalence rates used criteria such as ‘all children admitted for observation with loss of consciousness’.
A second reason that may have contributed to the heterogeneity is the definition of intracranial haemorrhage used in each study. In the adult literature Stiell and colleagues56 used a standardised definition after formally surveying 129 academic neurosurgeons, neuroradiologists, and emergency physicians. All brain injuries were judged to be clinically important unless the patient was neurologically intact and had one of: solitary contusion less than 5 mm in diameter; localised subarachnoid blood less than 1 mm thick; smear subdural haematoma less than 4 mm thick; isolated pneumocephaly; or closed depressed skull fracture not through the inner table. However, in the childhood head injury literature there was no single definition of a clinically significant brain injury and therefore some papers with higher rates of reported abnormalities on CT scanning may have been using more liberal definition than others.
We fully acknowledge that heterogeneity was introduced by these factors; however, in our systematic review we felt that using a single strict inclusion criterion would have resulted in loss of a large number of studies from the meta-analysis with potential loss of useful data. This approach has allowed us to both create relative risks from a very large number of patients and also to openly display the results of all these studies by forest plot so that clinicians are able to see the range of disagreement in the literature. We do caution the reader in the utility of a common odds ratio when there is significant variability among studies17,18 and encourage careful assessment of the forest plots presented here. However in contrast to the application of meta-analysis to randomised controlled trials where the confidence intervals of the estimate are of paramount importance, our aim was to provide an estimate of the relative risks for commonly used variables to enable these to be compared to one another. Therefore although there was statistical heterogeneity we feel that these results remain clinically useful.
Our results show that reduced conscious level, focal neurology, skull fracture, and loss of consciousness are strong risk factors for an intracranial haematoma (ICH). Seizure is classically seen as a well established predictor and indeed we did show an estimated relative risk of 2.82 for this variable. However, due to the great variability across the studies in the reporting of this variable this did not reach significance. The results of this study have shown that the variables headache and vomiting have not been reliably shown to be predictive risk factors for ICH.
Headache is a symptom that is difficult to elicit in the young and often not quantified in the literature pertaining to minor head injury. Some studies have reported headache as a dichotomous variable whereas others attempt to differentiate it into mild, moderate, and severe. In the adult minor head injury population, headache as a dichotomous variable (present or absent) has not been found to be predictive of ICH. In contrast severe headache has been shown to be predictive of ICH.22,23,56 In our meta-analysis the papers were found not to consistently sub-divide headache to allow comparison of severe headache and ICH, and thus we were not able to assess the utility of this potentially very useful variable. Future research needs to assess more carefully the severity and time course of headache in relation to the presence of intracranial injury in large populations.
Similarly vomiting was not found to be a predictor of ICH. This is not surprising because clinical experience dictates that even repeated vomiting over a limited period of time may not be any more significant than a single vomit in the paediatric population. This is in contrast to the adult population where repeated vomiting has been shown to be more significant than a single vomit.56,57 Many of the papers that we assessed in this study did not distinguish between a single vomit or more than one vomit, and hence we were not able to test whether repeated vomiting over several hours is more predictive than a single vomit in the paediatric population. In the same way that we feel that headache has been inadequately investigated, future research needs to analyse the duration and frequency of vomiting in the hope that vital additional information that is easily available in the emergency department could be use to select high risk children with minor head injury for CT scanning.
Several other potentially important clinical variables were not amenable to meta-analysis due to the variability of the reporting that did not allow pooling of the results. In particular age and mechanism of injury could not be analysed. The age of the patient is of paramount importance when considering many clinical correlates such as headache, focal neurology, and loss of consciousness, as in younger age groups these variables become unreliable or impossible to ascertain. Larger cohort studies in the future must have adequate power to sub-analyse all clinical correlates by age, especially in the infant age ranges.
Mechanism of injury is considered by many to be an important predictor variable and is used in several head injury guidelines.49,56,58 Other variables such as dizziness, drowsiness, nature of superficial injuries, and painful distracting injuries have been analysed in adult cohorts with minor head injury. However, these factors were not consistently reported as potential predictor variables in any of the paediatric papers presented here.
Significant loss of consciousness is used by most American hospitals as a criterion for admission and CT scanning. Our study supports the view that loss of consciousness increases a patient’s risk for intracranial injury. Focal neurological signs has been a classical indication for head tomography following head injury. This study has shown that although uncommon, this is a strong predictor for intracranial injury.
This study has also shown that a skull fracture is predictive of intracranial injury. If skull fracture is used as an additional variable to the history and examination in the decision to perform CT, it is useful in that we have shown that a fracture increases the risk of intracranial injury by four times. However, it is important to differentiate this from its utility as a diagnostic test. If used as a diagnostic test our analysis shows its sensitivity to be 59% and specificity to be 88% over the 15 studies, which is certainly unacceptable. The widely different usage of the skull x ray between the United States and the United Kingdom largely stems from this contrast between regarding it as a diagnostic test where it performs poorly and regarding it as an additional variable in the triage for CT scanning for which it has some use. However, we feel that future, well conducted large cohort studies will be able to optimally utilise clinical correlates from the history and examination to triage those requiring CT scanning with a high specificity, without the need for skull radiography.
We found that the issue of timing of the CT scan could also not be assessed using current data. This is a cause for concern as a small number of children may develop delayed subdural and extradural haematomas.59–61 Avoidance of ultra-early CT scanning or possibly a second delayed CT scan have both been proposed as management strategies that will avoid missing these worrying cases, but we found no evidence in support of this as part of a validated clinical guideline.
The results of this meta-analysis reinforce the findings that there are few reliable predictor variables for intracranial haemorrhage in children with minor head injuries. The development of well formulated paediatric head injury guidelines is hampered by the lack of information regarding many aspects of possible predictor variables in paediatric minor head injuries. Many of the studies have poor reference standards and lack accurate power estimates. Because of this, guidelines for childhood head injury suffer from a lack of specificity. This results in a large number of children undergoing admission or CT scanning despite a relatively low risk of an intracranial haematoma. We believe that the application of rigorous and accurate data collection applied to a large cohort of patients will allow the derivation and validation of far superior, evidence based clinical decision rules resulting in fewer unnecessary admissions and investigations. This has been acknowledged internationally and there are currently three major studies that are underway that may further our knowledge in this area.
Conclusion
The results of this study have shown that reduced level of consciousness, focal neurology, skull fracture, and loss of consciousness are predictors for intracranial haemorrhage in the paediatric population with minor head injury. We also found that neither headache nor vomiting increased the risk ICH, and that many other potentially useful clinical correlates have not been adequately investigated for use in risk stratification of minor head injury.
Current evidence does not allow the construction of a highly specific triage tool for children’s head injury, but future studies may soon make this possible.
REFERENCES
Footnotes
-
Funding for this study was provided solely by the Royal College of Surgeons of England. We are grateful for the support of the Enid Linder Research Fellowship from the RCS. None of the authors receive additional funding from any commercial companies.
-
The authors certify that they have no affiliations with any other organisations or companies other than those mentioned in the manuscript, that might unduly influence the findings of this study.
Linked Articles
- Commentary
- Atoms