Article Text

Abstract
Aims: To analyse retrospectively all referrals to the assessment unit during a seven year period, to determine their sources and destination.
Methods: All referrals over the seven year period were analysed. Parental satisfaction was determined using a questionnaire in some of the patients. The disease pattern and the investigations performed were determined. The community nurses’ working hours and type of work done were analysed.
Results and Conclusions: A total of 43 496 children were seen in the unit. Over 65% of the patients were referred by the general practitioners; 13 517 (34.2%) of those referred to the unit were discharged directly from the unit. Respiratory disorders and gastrointestinal problems were commonly seen. The children discharged from the unit did not have significantly more tests done on them. Most of the parents whose children were discharged from the unit were happy to be managed at home. The community nurses attended many children who needed intravenous therapy and advice on fluid rehydration. Community nurses reduce admission to the wards by working with other members in the assessment unit. This in turn provides a single point of entry and bridges the gap between primary and secondary care. We suggest recommendations on setting up such a unit.
- referrals
- assessment unit
- lessons
- community nurses
- ICP, integrated care pathway
- PAS, patient administration system
Statistics from Altmetric.com
The health service has witnessed escalation in emergency referrals to assessment units and accident and emergency departments.1,2 To ensure quality of care, patients’ needs and their views have been put first. The parents’ perception of their child’s illness has been given as one of the reasons for increased referrals.3
The trend of acute referrals to short stay facilities and accident and emergency departments has been increasing. Most of those children, if admitted to the wards, stay for less than 24 hours.4 This trend has continued despite improving social and economic conditions for most children, and improved child health with falling infant and child mortality rates. There has also been an improvement in training for general practitioners, with an increased availability of outpatient appointments.
There have been some concerns whether the establishment of such units encourages further referrals. There are more worries whether such units have sufficient time to provide health education as well as managing the acute illness. The time allocated for emergency consultations in general practice does not allow for such a comprehensive package of care for the children.
Health education to individual families reassures parents and gives them the opportunity to manage their children at home with or without additional support. The provision of that education, however, requires sufficient time and personnel.
Short stay facilities help in patient management and reduce admissions to hospitals. It has been shown that the unscheduled return visits by patients can be as low as 2%.5 Hospitals at home are being evaluated, and perhaps this might further reduce the number of children being admitted to hospital.
The development of guidelines to deal with the commonest medical problems would assist hospital and primary care staff as well as parents in ensuring that communication and management issues are dealt with efficiently.6
The modernisation programme for children and the national service framework needs to address access for all to emergency service. The impact of short stay facilities on quality of care is difficult to assess, and the views of parents also need to be taken into consideration if such facilities are going to be adopted nationwide to assist in planning of reconfiguration of children’s services.
We have run an assessment unit for the past seven years and have audited our data to determine the impact of an assessment unit on emergency referrals. We have also assessed parental satisfaction and the workload of the community nurses.
UNIT FACILITIES AND OPERATIONAL POLICY
The study was conducted in the assessment unit, which is a designated area adjacent to the children’s wards staffed by nurses who have no inpatient responsibility. There are specialist nurses in diabetes, asthma, epilepsy, cystic fibrosis, and critical care. There were two community nurses until December 2000, when one left and is due for replacement.
There is a specialist registrar and a senior house officer during normal working hours, 0800 to 2030. The unit opened in November 1994. We have been operating a consultant of the week for the past four years but before that we operated a consultant on call for the day. Other details and operational policy have already been published.5
The main emphasis is a full assessment, including social circumstances. A decision to admit a child is based on whether the child’s medical problem can only be managed safely in hospital. Thus the other options could be: discharged home without further input from anybody, a period of observation in the unit before going home, review in the assessment unit within 72 hours, see a family doctor, see a specialist nurse, or an outpatient appointment. Health education and information leaflets are offered as necessary. An experienced member of staff registrar grade or consultant of the week effects the discharge from the unit. The object of our audit was to determine whether the unit consistently offers a safe service for children and the role of the community nurses.
METHODS AND ANALYSIS
The data have been collected over the past seven years since the unit first opened (between November 1994 and November 2001). Demographic information was collected and stored on a database within the unit. This has been cross checked using the hospital patient administration system (PAS), and a hand written register based in the unit. The demographic data and outcome of the consultation have been analysed retrospectively.
Between August 2000 and December 2000 data were collected for each of the 1033 patients referred to the assessment unit. Parents of every child in this subgroup filled in a form as part of patient evaluation of the service. This information was followed by a telephone call to the parents within one week of attending the assessment unit. The data collection form was designed using the FORMIC package, which allows the form to be read by a scanner. The data were then analysed using SPSS.
A further 300 randomly selected patients’ notes were analysed to determine the investigations performed on those admitted for inpatient care and those discharged from the assessment unit.
The community nurses’ service was analysed by looking at caseload referrals and type of care provided from January 1999 to December 2000. The number of extra hours worked by the community nurse has been used to estimate the ratio of community nurses required per patients referred per year.
RESULTS
Figure 1 shows the total number of admissions over the seven year period. It is evident that the number of children staying in hospital for less than 24 hours gradually increased, but there has been a decline over the past two years. There is a similar trend for those staying in hospital for more than 24 hours, but the total numbers are significantly less than those staying less than 24 hours. These numbers include children who were admitted during the night when the assessment unit closes.
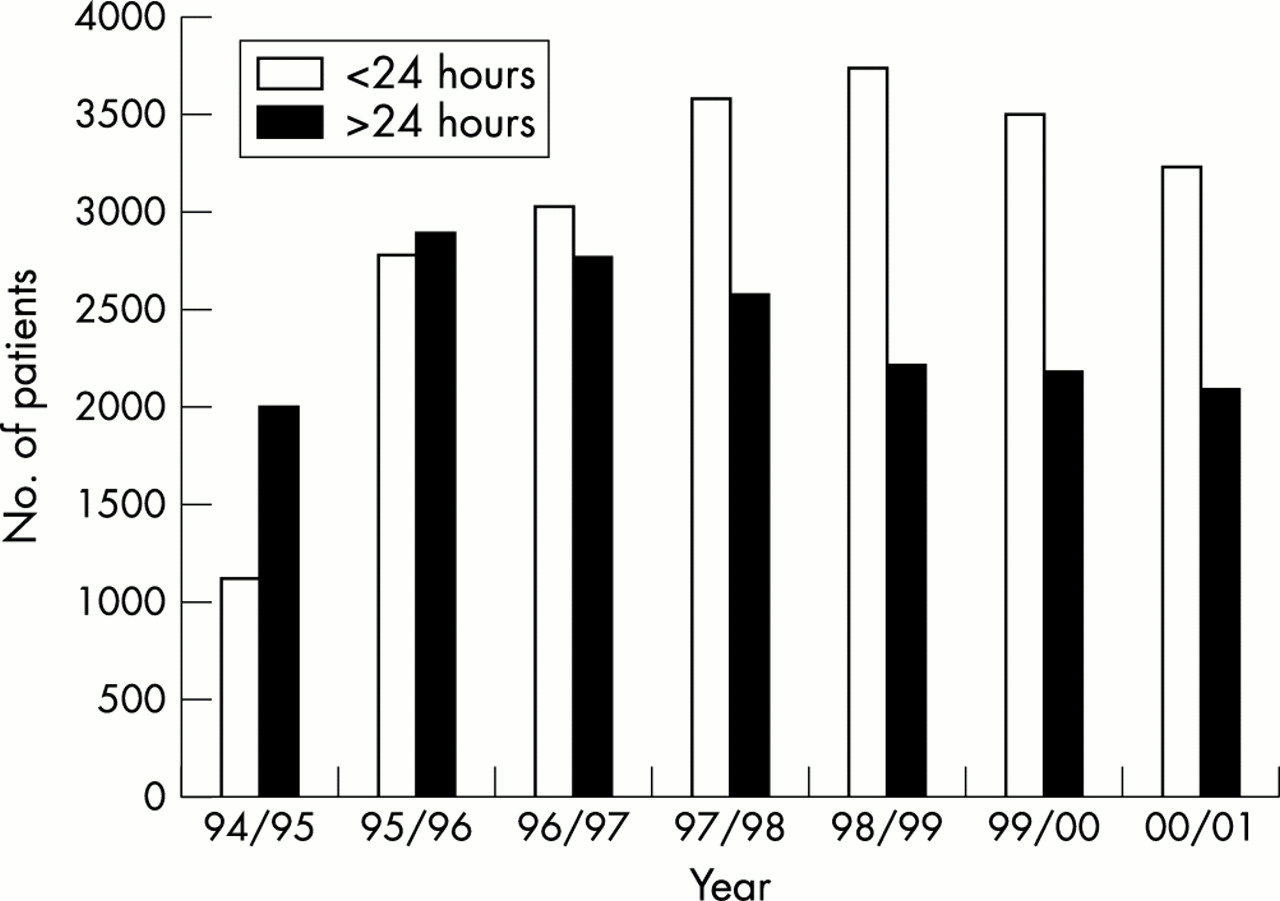
Length of stay on the wards.
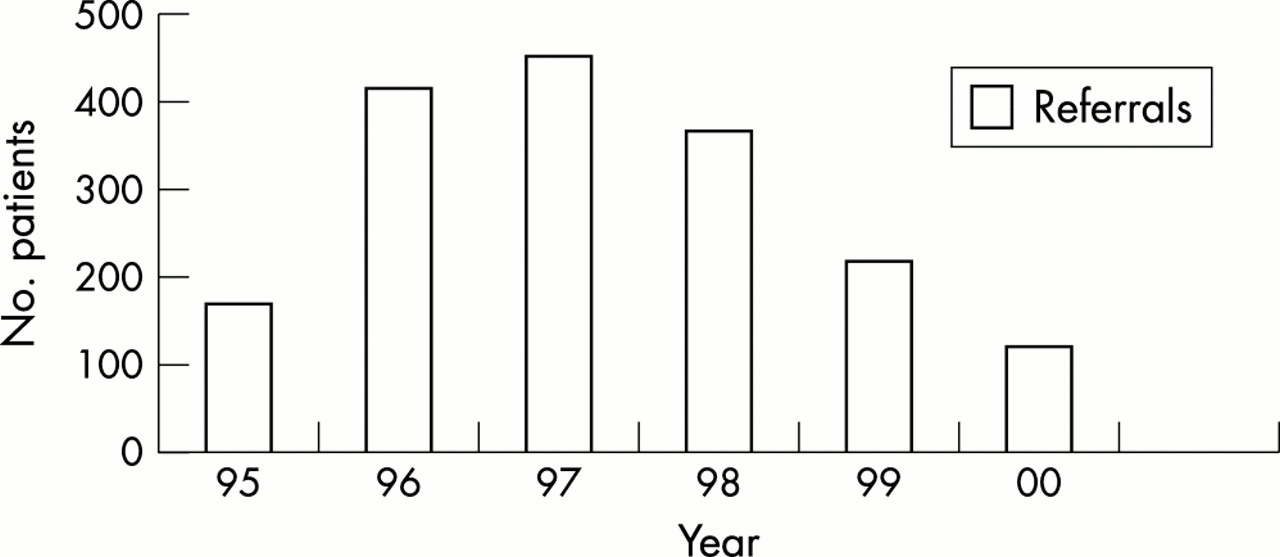
Figure 2 represents the referrals to the assessment unit over the same period. Historically, a referral equated to an admission before the unit was opened. Since the opening of the unit, 34.2% of the children referred to the unit have been assessed and sent home. The average period of stay in the assessment unit was 123 minutes for children who were sent home. Observation in the unit, waiting for medication from pharmacy, or waiting for results of investigations were the main contributors to the prolonged length of stay in the unit.

Referrals and discharges.
Table 1 shows the sources of the referrals. Most patients were referred by the family doctors and by the accident and emergency department. The number of self referrals is very small. Other sources include the community paediatricians and specialist nurses. Table 2 represents the disease pattern of patients seen in our unit; it is not different from that seen in other hospitals.5,6
Sources of referrals
Frequency of medical problems
Table 3 shows the views of those parents whose children had been admitted. Of 1033 children, 682 were admitted. The majority of those would have been happy with home care if there had been sufficient support for them, but 45% were happier to be managed in hospital. At least 5% were unsure what would have been most appropriate.
Parents’ views
Of those that were discharged from the assessment unit, 0.4% were seen in hospital again for the same problem within three days; another 15.9% spoke to either the family doctor or someone else—either a nurse in our unit or a non-medical person for reassurance.
Of the 300 children whose notes were analysed for investigations performed, 150 had been admitted and 150 discharged from the assessment unit. The group admitted to the ward had 213 investigations performed, compared to 62 investigations in the group that was discharged. Urinalysis was the commonest investigation in both groups, followed by a full blood count and tests for acute phase proteins. Thus children discharged from the assessment unit in this cohort did not have excessive tests performed on them.
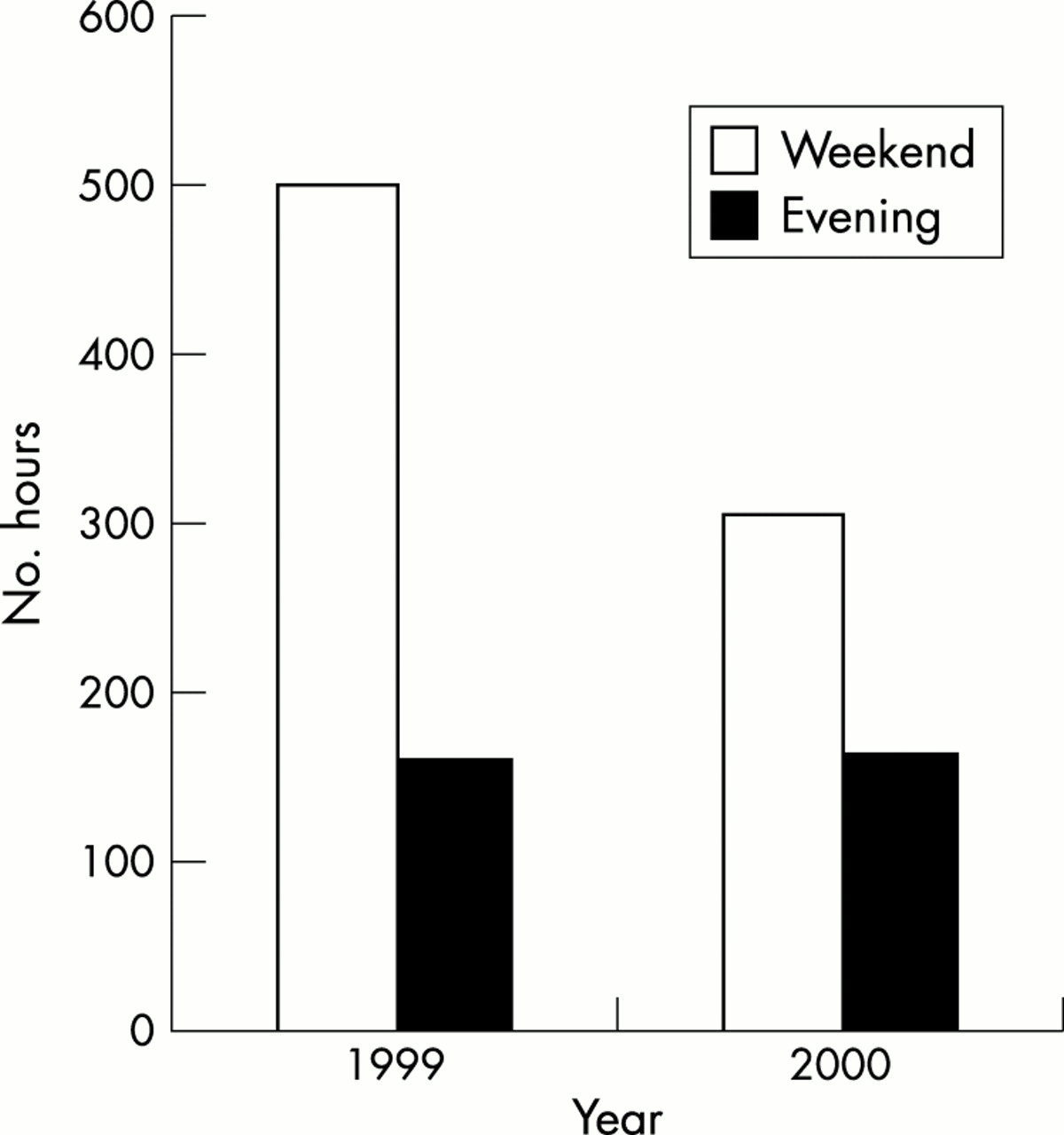
Figures 3 and 4 show the increasing workload referred to the community nurses. The quantifiable work was administration of intravenous antibiotics, but a considerable amount of reassurance and health education was also provided. We have not included analysis figures for 2001 as one of the community nurses had left. The figure also shows the number of extra hours performed by the community nursing team.
Referrals to the community nurse.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Extra hours worked.
DISCUSSION
This paper provides information on the effect of an assessment unit on emergency referrals: investigations performed within the unit; community nurse work load; and for the first time, a parent’s view on the performance of the unit.
The assessment unit was established to reduce the number of admissions to the wards, the philosophy being that only children whose conditions can only be managed in hospital should be admitted. The patients’ and parents’ perceptions had to be addressed as well as those of general practitioners, and medical and nursing staff in the community.7–9
Improved primary care alone does not prevent the admission of children to hospital.10 This is not surprising given the expectations of parents, and the pressure and constraints on general practitioners’ time.
An assessment unit bridges the gap between primary care services and secondary care services. It also provides a single point of entry to secondary care services. The unit also allows for a period of observation to ensure that the patient is stable and parental concerns addressed. The average period of observation for those sent home was two hours. This is comparatively shorter than what has been observed in other units.11
The assessment unit ensures a high quality service and reassures both primary care teams and parents. Although the referral rate has not declined significantly, the admission rate has shown a decline over the past seven years. This decrease can be attributed to confidence, experience of the members of staff, and the availability of community nurses. The ambulatory service has also been accepted by both parents and general practitioners.
We however, witnessed a significant increase in referral rates soon after the opening of the unit. We do not have an explanation for this increase. There may be several reasons, including the fact that family doctors may have felt that parents needed reassurance, parental demands, or lack of time for the family doctors. The other possibility is that this was a new service available.
This trend has declined, but the referrals to the community nurses’ team have also increased. Intravenous antibiotic administration is one of the main reasons for the community nurse visiting in addition to education and reassurance. Parents share the guidelines and are assisted by the community nurses wherever necessary. The admission rate to the wards continues to go down. Where necessary, a scheduled appointment is issued for review in the unit, but this is always kept to a minimum.
We have shown that at least 34% of children referred can be discharged home safely. We have also shown from a subgroup analysis in our sample that 48% of those who were admitted to the ward and managed as inpatients would have been happy at home. This, however, could only be made possible if further support was available at home.
Temperature control, fluid replacement, and reassurance are required, necessitating a longer period of observation and health education on the specific problem.5
In our cohort, respiratory tract problems were the commonest disorders seen, followed by gastrointestinal problems—mainly gastroenteritis. Conway and Newport found that all gastroenteritis cases which had been admitted to hospital could have been managed away from the hospital environment.12
In this study, the parents whose children were sent home directly from the assessment unit did not experience any problems and were happy for their children to be managed at home; 82% of those parents were happy to be contacted by a member of our team, either by phone or a visit. Thus, although some parents needed further reassurance, it did not necessitate a visit either to the family doctor or back to the hospital, except in a very small percentage (0.4%). Such consultations can be avoided with the help of community nurses.
Investigations need to be planned properly to avoid unnecessary waiting. We found that urine microscopy was the commonest test done. Although respiratory illnesses were the commonest problems seen, there were few chest x ray examinations done. It is reassuring to note that more investigations are not performed as a prerequisite to sending children home.
The cost effectiveness of an assessment unit is difficult to quantify.13–15 We know that family disruption is minimal, and transport and childminding expenses are reduced. For the hospitals, hotel services are reduced. We feel, however, that planning to set up an assessment unit should not be looked at as a money saving programme, but be considered as a quality issue.
There are other benefits, which include education and training for both parents and staff. Undergraduate and postgraduate students have a chance to experience the teamwork of both primary and secondary care services. Doctors on vocational training and accident and emergency programmes, learn a considerable amount about common paediatric problems. We feel that this provides a basis for planning the future of efficient paediatric emergency services.
The experience over the past seven years has taught us a few lessons which would benefit those planning to set up a similar unit.
Planning
Planning such a unit requires input from the primary care team and health authority to look at the needs of the community. We had such a meeting and we were assisted with funding. The family doctors needed to understand how the unit could be used for the benefit of patients and themselves. Others parties include pharmacy, x ray, and laboratory departments, and the ambulance service. Involvement of the ambulance service ensures that all medical emergencies go to the right place and not to the main accident and emergency department. This is assisted by installation of a two way communication system.
Space
The size and location of the unit are important for ease of access and being adjacent to the inpatient unit. We started with a small unit that needed expansion; our new facility will be bigger to allow for a longer period of observation and privacy. The interface with the outpatient department is a problem, as non-emergency but urgent referrals to outpatients need a different facility. Office accommodation for both clinical and non-clinical staff must be made available.
Staffing
Adequate medical and nursing staff is critical for the success of the unit. Experienced children’s nurses are required, as well as a mother figure to help parents with little experience of child rearing. The mother figure provides education on issues such as nutrition and nurturing. A separate team should deal with outpatient type work. NHS Direct and a clear understanding of referral processes might help in this regard. Clerical staff must be available every day to ensure adequate communication to the family doctors.
Assessment
Assessing children requires experienced staff, but also time. We believe that the time spent with the parents gives them an opportunity to see what is being done. They are then reassured that they can do it at home and observe the child getting better. Their perception of the illness can be addressed, and where necessary an agreed plan is explained in detail. The amount of time taken requires more staff, and we believe that the outreach nurses working in both primary and secondary care are best placed to bridge this gap. We started with two community nurses, but estimate from a calculation based on extra hours (fig 3) that there is a need for another four community nurses. This equates to one community nurse per 1000 referrals per year. The planned expansion in this area would reduce the extra hours worked at weekends, and enable a service to be available every day.
Opening hours
We believe that if children are observed for a longer period, our average being two hours, it is possible to reduce further the number of admissions; this, however, influences the opening hours. More staff and therefore more resources are required.
Of those children who were admitted, some were admitted because they came towards the later part of the day and could not be observed in the unit. Other reasons were because of single and unsupported parents with little experience, lack of transport, and children under the age of 5 years.
The needs of individual families vary and therefore further evaluation is needed. However, parents whose children stay less than 24 hours often require only a period of observation, temperature control, fluids, and reassurance. We would recommend that integrated care pathways (ICP) for common minor illnesses be agreed between the primary care and secondary care teams, to be facilitated by the outreach nurses to ensure safety for patients.
Transport
We would recommend that when planning to set up an assessment unit in a place without an inpatient facility, transport arrangements similar to the retrieval service in neonatal and paediatric intensive care should be agreed. This would be very important for children who are usually seen late in the evening when the unit is due to close. Although children may not be seriously ill, parents may not have their own transport.
Communication and discharge
It is important to know what the family doctor’s concern is when a referral is made. When a parent’s or child’s perspective is addressed, the correct decision is then made in the interest of the child. We provide a discharge letter to the parent and a copy sent to the general practitioner. We believe that electronic mail or faxed messages are the way forward, to ensure rapid communication, both at referral and discharge.
Reviews
Both scheduled or unscheduled returns can be minimised if adequate outreach nurses are in place to contact the parents at agreed times. When parents are contacted by phone, their worries are alleviated and unnecessary trips are avoided. Where necessary a trip to the unit can be arranged without the need to go back to the general practitioner so long as it is in relation to the original problem. There is a 72 hour window for parents to contact us with reference to the original problem. This creates a considerable amount of work on the telephone; perhaps it could be made shorter.
Investigations
A microscope for urinalysis is essential. Training of both nursing and medical staff ensures early diagnosis and plan of subsequent investigations.
Training and education
Traning in basic life support and paediatric life support measures should be prerequisites for staff in the unit. An invitation should be offered to all general practitioners and paramedic ambulance crews to familiarise themselves with the mechanics of the unit. A one day seminar for the local community is a very good way to introduce the service to the primary care team. ICPs can reassure both the general practitioner and parents that a condition which they thought could only be managed in hospital can be dealt with at home safely.
Medical staff
An experienced paediatrician at registrar level or above should be available. In addition to seeing the children, he/she also offers phone advice on a variety of both medical and social problems. However, senior house officers and preregistered house officers are invaluable, and will also learn a considerable amount about child health.
Research and audit
There is a need to establish a common database to provide more information on common illnesses. This will lead to the development of appropriate ICPs designed on evidence based practice. This might also assist in agreeing the appropriate tool to help in deciding which patients to discharge.
Cost effectiveness
This is always difficult to calculate. Six community nurse at £20 000 per year will cost £120 000 plus travel expenses; 110 children per month discharged from the assessment unit at an estimated saving of £200 per night would save £264 000 per year. This presupposes that all medical staff and the nursing staff based in the unit would be required if children were admitted to the ward. The calculation does not take into account the family disruption, but still appears to be cost effective.
Conclusion
In summary, if we were to start all over again we would ask for more space, more staff, transport, and better information technology for better communication.
In conclusion, we have shown the impact of an assessment unit on acute paediatric referrals leading to reduced admissions. We have also learnt some lessons that might help others who would consider setting up their own facilities. Parental satisfaction has been documented and continued use by the general practitioners has ensured its success. We have also shown the need for community (outreach) nurses to maintain safety for all children.
Primary and secondary care teams working together can reduce admissions to the hospital, to the satisfaction of everyone.